


Efficacy by Procrastination?
Is "severe efficacy" just a byproduct of sitting out Alpha and Delta? Also: Throwing a wet blanket on supposed refutations of the biology of severe efficacy.

Let’s take another look at the severe efficacy controversy, shall we?
As always, the disclaimer applies:
When it comes to severe efficacy for the Covid vaccines, my position has always been that [severe efficacy] does not mean anyone should take them. Even in the most “high-risk” groups, most people do not progress to severe disease. Most individual people therefore cannot benefit from severe efficacy; they can only incur the added risk of the experimental transfections. I have said this a million times; I am saying it again now.

i. Severe Efficacy Is Biologically Possible
A recent fad is to boldly claim that circulating IgG antibodies for spike protein cannot possibly protect against severe disease.

The apparent new “gotcha” is that IgG can’t get to the lungs, and so it can’t possibly have an impact on disease or viral loads (to vaguely paraphrase). Really? That’s all been tested, has it? Or are we just back here again:
It is not that there is no argument at all here.
For example, in natural infection, Sterlin, et al. found that IgA responses seem to activate earlier than IgG; in particular, IgA-producing plasmoblasts with mucosal homing profiles were highly expanded in early days, suggesting that the immune system was taking the fight straight to the mucosa, and the systemic front (i.e. the bloodstream) was an afterthought.1 But the same study found that:
IgG concentrations were consistently higher than IgA in the tested [Bronchoalveolar Lavage] samples, except for one patient (fig. S5F), but IgA concentrations were higher than IgG in saliva […]. Consistent with these findings, previous reports demonstrated an increased IgG:IgA ratio along the respiratory tract, as measured from the nasal compartment to the lungs
In Bronchoalveolar Lavage, the “lavage” stands for washing. A tube is stuck into the lungs, and some saline is squirted in and then sucked back out, to soak up some of what is down in that “dry” space.2
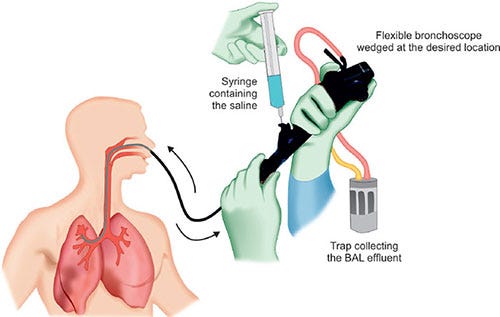
A fun “fact” about these washings of the lung’s “dry” space is that humans consistently have IgG antibodies there.3
Now, consider these additional “Facts.”:
Humans barely understand viruses or the immune system. This fact may be cause for anger, but it isn’t to any extent ameliorated by the same. And so as a general rubric, more confidence indicates more ignorance. Nihilists are always the most confident of all; and as such the least interesting.
Injected vaccines have been used for flu for almost a century despite the limits of IgG.4 This is the example par excellence of the limits of serum antibodies, but it isn’t a wholesale refutation. Flu vaccines seem to work for a limited time, especially with new subtypes, and “a limited time” still describes human experience with SARS-CoV-2. Hilleman whipped up a vaccine for H2N2 in less than a year and it seemed quite adequate at preventing infections in 1958, even if administered during waves.5
Covid vaccines seem to induce some localization of spike-specific T Cells in the lungs; though unsurprisingly less than vaccination plus infection. These T Cells seem to stick around for several months. From a preprint uploaded in January (Mitsi, et al.):6
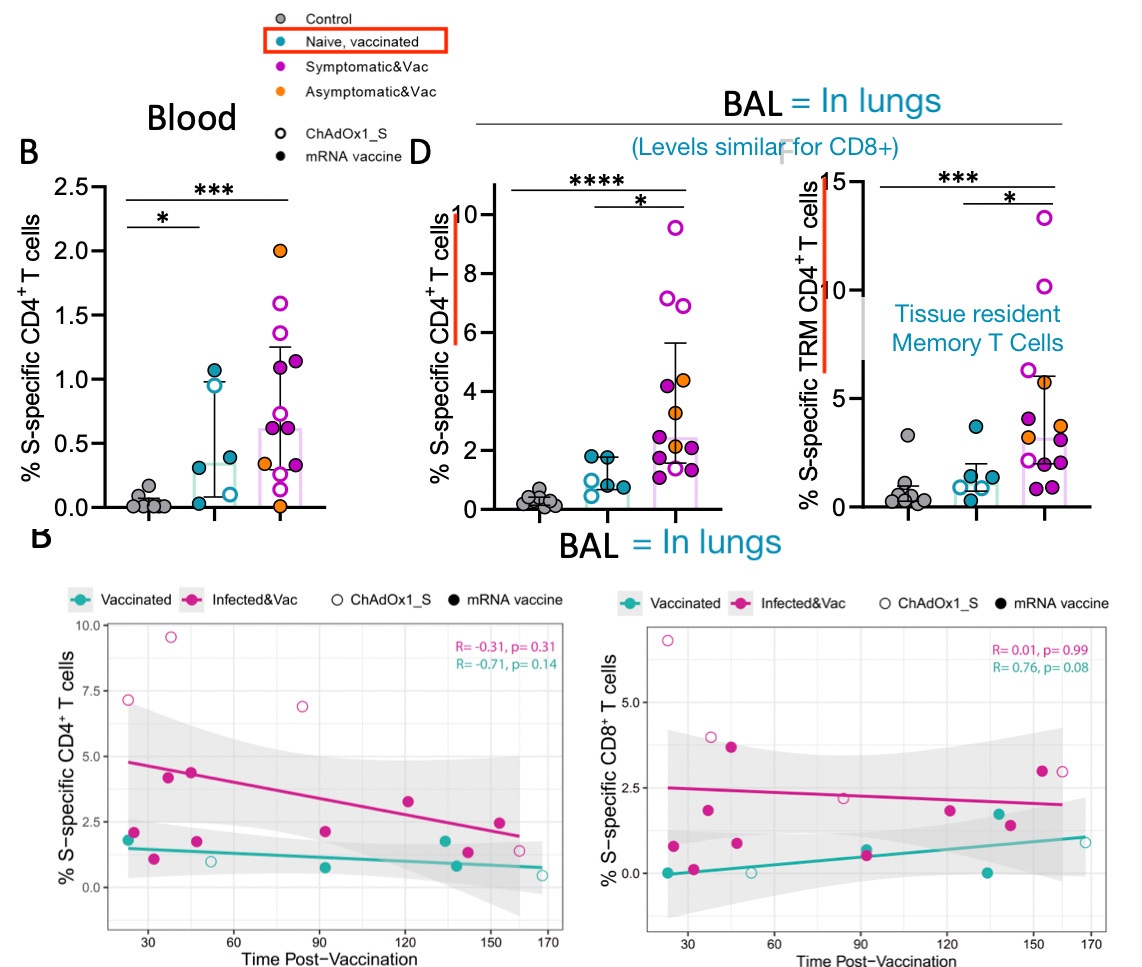
Mitsi, et al. Lest one imagine that this study (due to originating from the University of Oxford) is pro-vaccine propaganda, the authors characterize the infection+vaccine response as “robust,” and vaccine alone as “not” so. As discussed, above, serum IgG is known to seep into the mucosa (transudation).7 Covid vaccines therefore also result in the presence of IgG in the lungs. Again from Mitsi, et al.:
Serum (i.e. bloodstream) IgG can limit severe disease in other plausible ways.
Tagging infected cells for destruction (before IgG4 conversion (a.k.a tolerance) disables this benefit). This could presumably happen on either “side” of the respiratory epithelium in alveolar and other spaces.
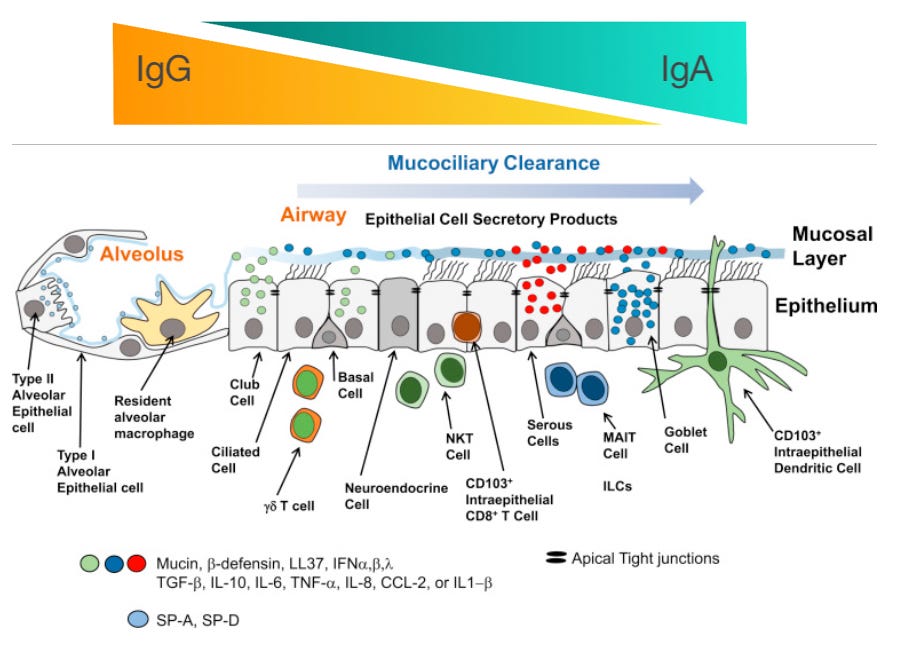
The deeper into the lungs, the more friendly the environment for IgG rather than IgA. Further, alveolar macrophages, the must abundant innate immune cell in the alveolar space, bear receptors for IgG (but, again, not in the IgG4 form); so IgG helps them see and eat (phage) infected cells.8 IgG clearly seems to have a role for protecting the lower respiratory tract that goes beyond neutralization (which is low in early natural immune responses).
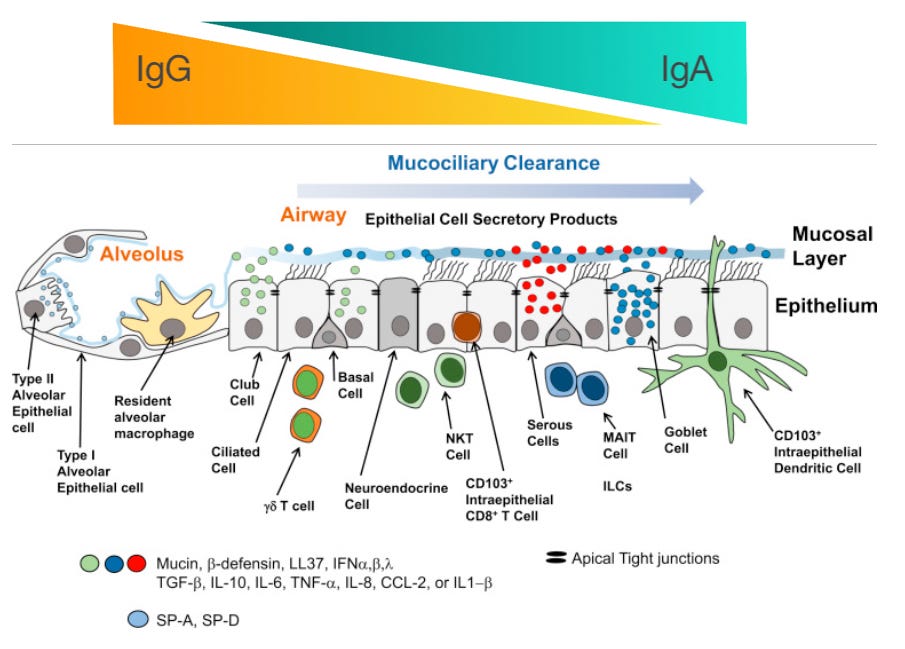
Denney, L. Ho, LP. (2018.) Fig. 1 with added sliders for IgG / IgA. Importantly, IgG-mediated eating of infected cells may substantially reduce the poorly-understood toxicity of other viral proteins in the lungs, i.e. if infected cells are acting as toxin factories that pump out M protein to sabotage the plumbing of the lungs, then there is no reason to trollishly discount an IgG-mediated benefit regarding strictly-defined Covid-19 pneumonia.
Reducing viremia, i.e. preventing the virus from using the bloodstream to spread.
Potentially nullifying the coagulatory effects of the spike protein.9


These are not only plausible but important suppositions, because they also explain why most people do not need these injections.
As long as the immune system mounts a prompt response to the virus, with IgA and IgG / IgM, there is little danger of severe disease. Here, again, I would cite the results in the placebo group of the Paxlovid trial, in which early IgM or IgG-havers were protected against severe outcomes.
So the vaccines can prevent severe disease by front-loading this early response; but most people do not need to front-load this response, they will mount it on their own; and therefore should not be undertaking experimental gene transfection in order to do so.
ii. The notion of trace protection
Let’s simplify the whole question to what is at the “front lines” during “breakthrough” infections — trace spike-specific tissue resident T Cells and IgG antibodies.
IgG transudation in the context of the Covid vaccines is poorly-studied (again, no one still really knows what they do in the body), but is not a wild conjecture. Regardless of mechanism, both IgA and IgG are apparently induced in the mucosa to some extent after vaccination (though IgA rapidly recedes, just as after infection).10
Is it plausible that there is some grey area between leaked (transuded), super-high serum IgG antibodies protecting against infection (along with temporary IgA further up in the respiratory tract), and dropping to levels that no longer stop infection, but can still tamp down on initial viral spread? Well, just why exactly wouldn’t there be?
It is entirely reasonable to expect (and there is no obvious reason not to) that there is a period of partial protection in which vaccine-induced IgG acts as “training wheels” for natural immunity, allowing grandma’s immune system to ride out the virus without bumping her head.

And — wait a second — isn’t this, isn’t this…
Isn’t this exactly what is being proposed when we advocate for therapeutics and early treatment?

Once again, nihilism is just a self-own. Without acknowledging and understanding why it is biologically plausible that the vaccines are protective, one no longer has a coherent argument for why they are not necessary (i.e. that innate immunity and early adaptive responses can do the job just fine for most; or that treatments can help for those who need it).
If Lee is correct about “dry” lungs, on the other hand, then why aren’t I correct to post this:
iii. An additional insight: “Mucosal Covid vaccines” are likely a pipe dream
If we embrace an understanding of the surprising, indirect induction of trace protection in the mucosa from the current Covid vaccines, we are left with a corollary conclusion: “Mucosal” vaccines probably will not perform much better than injected ones at generating immunity to respiratory viruses.
Just as with the poorly-substantiated efforts to blame the eventual futility of flu vaccines (they appear to work for a short while, but not for long) on antigenic drift and superstitious, ridiculous notions of “Original Antigenic Sin,”11 blaming the failure of the Covid vaccines to prevent infection entirely on their route of administration is excuse-making.
The reason vaccines do not replace natural immunity is because they are not natural. You cannot make synthetic nature. Humans must learn to accept that in the game of immunity, there is no gain without pain; otherwise we would all have just been born with our mother’s B Cells; it’s not like evolution could not have thought that one up.
And, again, once we accept that natural immunity can only follow from infection, it becomes obvious that reducing severe outcomes (for those who need it) from therapeutics during infection is more sensible than pre-injection.
iv. But Was Severe Efficacy Nonetheless Real, or Illusion?
Despite having found the previous evidence for severe efficacy compelling enough, I have recently begun to entertain doubts.
The Astounding Rate of Natural Immunity Debt
Specifically, my previous notions were based on the assumption that the injected and boosted were still being infected. I.e., if infection efficacy were zero, but severe outcomes still more rare in the injected, then you could trust that the signal was there (regardless of the user bias question, which I don’t find that interesting).
But since the summer, it’s become clear that “gobs” of the boosted were still totally naive to the virus before then. This means that many weren’t actually being infected before. For a review of the evidence for persisting natural immunity debt in the über-boosted, see “It Will Always Be Catchup Effect.”
As a discrete example, consider reported infection rates among those recently seeking a bivalent shot in Nordic countries:12

94% of recent booster-getters (who, granted, represent only 4% of the population) in Norway report no previous infection. Such outlandish rates of immune debt encourage caution on interpreting all previous calculations of severe efficacy, as it’s not clear if the fat lady has even put on the Viking hat yet.
This all leads to a question on how to interpret the following, in the country where vaccine uptake was rampant, but so, apparently, have “breakthrough” infections been:

Obviously I could have used cumulative deaths instead of clunky, manual area-under-curve hashes; but this makes for an easy way to split deaths during transitions between variants.13
Essentially, the figures from the UK seem to lead to a paradoxical argument: The vaccines must certainly have reduced deaths from Delta (compare with low-vaccine-uptake states in the US); but this simply seems to have left a debt that has come due in the Omicron era. This (or a combination of this and high rates of other types of infections) best explains the rise in excess mortality in late 2022, which itself is best explained by comparing vaccinated all-cause death rates in late 2022 with earlier months:
This also shows that deaths (absolute and rate) have become higher [in December 2022] in the 3rd-dose group, whereas it was fewer-dosed elderly who drove deaths the December before. This supports a role of “catch-up” infections with SARS-CoV-2 in the excess mortality trend.
The same comparison could be repeated for previous months (which I have yet to format); and may support the general picture that the Covid vaccinated elderly are steadily dying at above-2021 rates throughout late 2022.
But a “postponing infection” theory of efficacy should predict that the vaccinated, having missed Alpha (by pure survivorship bias) and Delta, should be winners by mere virtue of “Omicron ex machina” — a new version of the virus descended from heaven to pluck them from impending danger — and the advent of Paxlovid. But it’s not clear that they are actually winning at all.
The only natural interpretation of this paradox is that the vaccines never had any severe efficacy at all. They only postponed infection.
However, this interpretation is problematic for the simple reason that the system being interpreted is so extremely complex. Assumptions that many people were really infected with the virus before the Omicron era, in particular, must be set aside — instead, the virus was still “playing with its lunch.” Relative to the population as a whole, “the pandemic” doesn’t begin until Omicron.
Attempting to normalize deaths to infections
Test-based official “cases” are an unreliable measure of this effect, since testing rates dropped after March, 2022. We can instead consider rates of positivity for antibodies to Nucleocapsid, which can be measured in blood donors. The problem is that these antibodies wane over time — akin to a bucket with a leak — and that our age groups of interest — the elderly — all have different levels, reflecting differences in immune response, survival rates, and donor biases (do the infected stop donating?).
As noted previously, Omicron nonetheless exerts an inflection in N seropositivity rates:

It is almost certain that 70 - 84 year olds are dropping out of the donor pool after infection, because the confidence interval continues to widen throughout the entire observation window (i.e., bigger brackets around the shapes mean fewer donors). This is true in the 60-69 group as well, until a reversal in mid-2022. The point is that the lower end of the range — 12 and 70 — must under-state true infection rates.
Bearing in mind the other problem of antibodies waning, I will just use the top of the range (50-59's) and weight deaths by change in elderly N positivity. I'll use .03 as a provisional value for the first wave (based on the super-low seropositivity rates recorded in school-kids14), to allow removing the first wave from the mix (on the assumption that those deaths were exacerbated by various means). Eyeballing the graph above for the other figures (everything here is really just provisional anyway) gives the following progression:
Very back-of-napkin attack rates per era (excluding reinfections):
B.1: .03
Late B.1 and Alpha: .17 - .03 = .14
Delta: .28 - .17 = .11
Omicrons: .87 - .28 = .59
Excluding reinfections is both unfair and not — presumably they are measured by N positivity due to “re-upping” lowered antibodies.
This results in the following arbitrary “deathiness-per-sort-of-elderly-infection-rate” values:
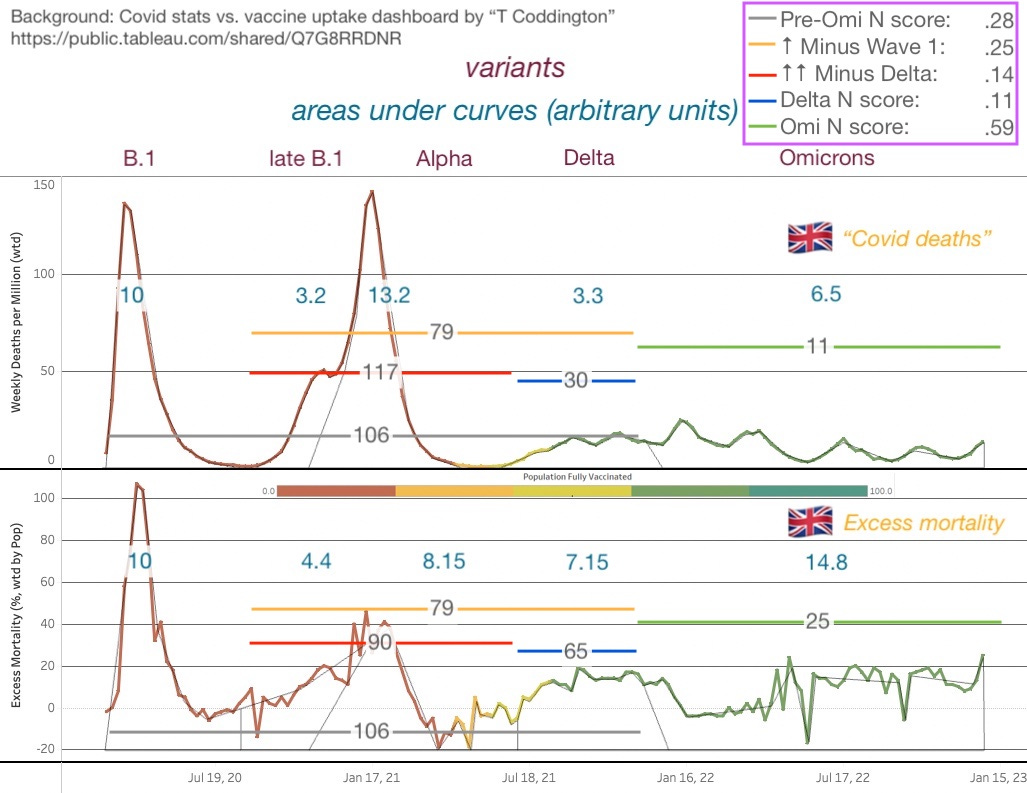
Besides revealing some weird accidentally matching ratios in areas under the curve (B.1 / (Late B.1 to Delta) is the same on both graphs), has the paradox persisted, or not? Deaths-per-badly-estimated-elderly-increase-in-elderly-seropositivity argues for severe efficacy in the Delta era. Omicron… well… applies an additional discount. So now you have reduced deaths from both severe efficacy and a family of heaven-descended milder variants (vs. would have occurred if the same rise in infection rate had occurred without both elements). Perhaps there’s no problem here after all?
Overall, I remain (newly) doubtful. If I have overestimated the true number of elderly (especially vaccinated elderly) Delta infections, the whole argument is out. A few points difference changes the excess deaths score from 7.15/.11 = 65 to 7.15/.08 = 89, which is just the same as the pre-vaccine wave.
v. Why not propose (again) that both things are true
Leaving aside the counter-argument in the previous section, let’s just go back to asserting that there is too much vaccinated death in the Omicron era to substantiate a belief in severe efficacy, prima facie. Why not simply suppose that the paradox resides in the biology itself?
Severe efficacy is real; and so is some form of “negative severe efficacy.” This could be due to the arrival of IgG4 tolerance, which potentially turns vaccine-induced IgG into a viral cloaking device in the lower lung and elsewhere. Or, it could be due to general degradation of the immune system. As I have speculated previously, this could be leading to negative outcomes, including post-infection death, from exacerbated “Long Covid” due to persistent infections.

If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Sterlin, D. et al. (2021.) “IgA dominates the early neutralizing antibody response to SARS-CoV-2.” Sci Transl Med. 2021 Jan 20; 13(577): eabd2223.
Presumably “dry” is meant to be understood as not submerged.
Reynolds, HY. “Immunoglobulin G and Its Function in the Human Respiratory Tract.” Mayo Clin Proc. 1988 Feb;63(2):161-74.
However, it is fair to argue that there is a traditional school of thought that vaccine efficacy against severe disease depends on viremia as an intermediary stage of disease, as in the case of the research leading to the polio vaccines. I would argue that this conclusion was not correct to begin with, and viremia in polio is not as dangerous as pseudo-autoimmune attack. See “Decoding Polio.”
Obviously there is more that can be said about the effectiveness and limits of flu vaccines. Suffice it to say that many of the cited limits of flu vaccines are poorly-substantiated; my own guess is that the main problem with vaccines is that the unvaccinated are constantly building up superior natural immunity, resulting in the control group outperforming the vaccinated when the virus returns next season. “Hoskins’ paradox” is not some great biological mystery, but simple futility (see “OAS Lit. Review / Timeline Pt. 2”).
Mitsi, E. et al. “Long-term respiratory mucosal immune memory to SARS-CoV-2 after infection and vaccination.” biorxiv.org
And serum IgG alone has been shown to correlate with protection against severe disease from RSV, another respiratory virus. As previously reviewed:
Collins, PL. Graham, BS. (2008.) “Viral and Host Factors in Human Respiratory Syncytial Virus Pathogenesis.” J Virol. 2008 Mar; 82(5): 2040–2055.
Virus-neutralizing antibodies in the respiratory tract likely contribute to viral clearance and certainly play an important role in protection against reinfection. They include secretory immunoglobulin A (IgA) and transudated, serum-derived IgG. […] Serum IgG antibodies are somewhat more efficient in accessing the lower respiratory tract and can provide substantial protection in that compartment. In RSV-naïve infants, the maternal serum antibody titer is positively correlated with a reduced level of severe RSV disease. The clinical experience with palivizumab also shows that serum antibodies alone can provide substantial protection [55% in at-risk infants] from severe disease.
The original version of this post stated that alveolar macrophages do not have receptors for IgA; it seems they have been found to do so.
Or I could say “presumably,” since otherwise it is difficult to understand why vaccine harms related to clotting don’t seem to have a dose-dependent effect when it comes to serial injection (i.e. boosters). Pre-existing antibodies seem to protect against future transfected spike (but not against the first dose spike that generated those antibodies); so why wouldn’t they protect against viral spike.
Azzi, L. et al. “Mucosal Immune Response in BNT162b2 COVID-19 Vaccine Recipients.” EBioMedicine. 2022 Jan;75:103788.
See, again, “OAS Lit. Review / Timeline Pt. 2”
Andersson, NW. et al. “Comparative effectiveness of the bivalent BA.4-5 and BA.1 mRNA-booster vaccines in the Nordic countries.” medrxiv.org
Also note I replaced the boundary between B.1 and late B.1 in excess deaths, as the original version (a blended transition) made no sense. Accordingly, I changed to using each plot’s B.1 wave / 10 as a baseline (instead of late B.1).
See “The Quiet Corona-Can,” which reviews:
Ratcliffe, H. et al. “Community seroprevalence of SARS-CoV-2 in children and adolescents in England, 2019–2021.” Arch Dis Child. 2022 Jul 20;archdischild-2022-324375.
This is in relation to another of your articles. It was one that said that there wasn't a drop in antibiotic levels prescribed. I have just come across the chart from the UK that was in a substack by Dr Paul Alexander https://palexander.substack.com/p/devastating-four-4-graphs-in-uk-that and it includes a chart (about 3/4 of the way down) showing that in the UK the actual usage of antibiotics was significantly less than the predicted amount.
I agree with our view that we really don't understand viruses much yet. This article by one of the disinformation dozen was thought provoking for me https://greenmedinfo.com/blog/how-microbiome-destroyed-ego-vaccine-policy-and-patriarchy
Regarding this particular post. I worked in a hospital 20/21 and know a lot of older people. They basically all went into hibernation and hardly any of them would have been exposed to covid until mid to late 21 or into 2022. So I do think that they just didn't catch it. But when they did it was in the period after boosters and almost everyone got it within a one month period. Same thing happened again in Dec 22.
I have an unsubstantiated theory based entirely on personal observation.
I have had covid three times (no vx) (Feb 20, Oct 21, Jun 22). On each occasion my symptoms were not the same and it felt like completely different illnesses.
Major symptoms were:
1st time Swollen glands in throat, feverishness, then dizziness and then three days in bed feeling generally ill, bleeding gums mouth ulcers (still not quite gone away).
2nd time loss of taste & smell, ill for a couple of weeks again about three days ill in bed
3rd time (this was the worst) I got brain fog, couldn't read or write on computer. I believe it is described as 'loss of executive function'. I was hallucinating at one point, I almost passed out sitting down spent several days in bed. The brain fog took weeks to clear (nicotine tablets helped hugely) and it is only recently that I feel fully better.
I became a bit unwell Dec 22 and because every one else seemed to have covid I think it probably was covid again but I didn't test for it. It was no worse than a cold. I have recently been in close contact with someone who had covid and I didn't catch anything. So my hope is that we will all catch all the main strains once and then have some level of immunity then it does become like having a cold.
I have not seen anything in reality that supports that the vax did any good at all. People who were vxd who worked in the hospital all got covid just as often as I did and some were def more unwell than I was. There were one third of people who did not come into work the day after the first injections. Everyone had to go over two days unless they refused.
I am very concerned that the vax has caused many other illnesses that are taking a while to show up and so are not being included in safety reviews or counted as vax injuries.
The exerpts below are from UK gov May to Dec 22 report https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/excessdeathsinenglandandwalesmarch2020todecember2022/2023-03-09
Some of these are are shocking.
'Deaths remained substantially above the five-year average between May to December 2022, after subtracting deaths due to COVID-19. The remainder of this section discusses this period.
Deaths (excluding deaths due to COVID-19) were above the five-year average for 16 of the 20 age groups. The age group with the highest proportional excess was people aged 75 to 79 years (21.3% increase, 8,935 excess
deaths), followed by people aged 10 to 14 years (16.2% increase, 31 excess deaths).
The months with the most excess deaths continue to be April 2020 (43,796 excess deaths) and January
2021 (16,546 excess deaths); these were also the months which had the most deaths due to COVID-19.
Between March 2020 and December 2022, the leading causes of death with the highest numbers of
excess deaths in England and Wales were Symptoms, signs, and ill-defined conditions, associated with old age and frailty (12,170 excess deaths), Cirrhosis and other diseases of liver (4,846 excess deaths), and
Cardiac arrhythmias (4,375 excess deaths).
The age group with the most excess deaths that were not due to COVID-19 was those aged 75 to 79 years for both males (7,870 excess deaths, 7.8% above average) and females (6,187 excess deaths, 7.6% above average).
The place of occurrence with the most excess deaths due to causes other than COVID-19 was private
homes, with a 105,211 excess (29.1% above average).
While Symptoms, signs, and ill-defined conditions was the leading cause of excess mortality for females in this period (2,568 excess deaths, a 41.4% increase). For males, the leading cause of excess mortality was Ischaemic heart diseases, with an excess of 2,609 deaths (11.4% above average).
December 2022 saw a particularly high number of excess deaths due to causes other than COVID-19. This increase was driven by diseases of the respiratory system, such as Influenza and pneumonia (598 excess deaths, a 25.1% increase) and Chronic lower respiratory diseases (494 excess deaths, a 17.0% increase).
Diseases of the circulatory system also saw notable excesses. These include Ischaemic heart diseases with 454 excess deaths (a 9.5% increase) and Cardiac arrhythmias with 244 excess deaths (a 38.9% increase).
Deaths due to Accidental falls were higher than average in many months of the period studied (2,795 excess deaths). They saw particularly notable excesses in the months of June to October 2022, with 1,019 excess deaths (a 40.6% increase). This excess was largely accounted for by people aged 80 years and above, with an excess of 703 deaths (a 40.7% increase). This was observed similarly across both England and Wales'.
I would agree that more people at dying at home, this does not tie in with delayed ambulance calls but supports the concerns that people are dying without warning and before they can call an ambulance. I am hearing of lots of people falling which ties in with the numbers. It is not normal falling, these people are more collapsing than falling. There are a lot of people falling over who are not hurt so not going to hospital. Could be mini strokes? What doesn't match is that I am hearing of lots of people with cancer, its not showing here, could be it is being hidden in the non excess deaths? Ethical Skeptic has shown how it can be hidden. The largest group is so vaguely described one would expect it should be the catch all for anything that is missed, it doesn't make sense that it is the largest group.
Lastly it mentions that the worst months in terms of numbers of deaths are in the same months that covid cases peaked. There does appear to be a correlation between the two. I am of the view that getting covid is triggering at least some of the 'not from covid' deaths. I really hope this does tail off once everyone has caught had all strains and no more boosters are given.
Thank you for your excellent articles. Sorry my unstructured post littered with many punctuation errors and lack of factual information may be letting the side down!
'Humans barely understand viruses or the immune system. This fact may be cause for anger, but it isn’t to any extent ameliorated by the same. And so as a general rubric, more confidence indicates more ignorance.'
I'm saving this quote.