
The Worry Window Is Not Real Post, Pt. 2
Alas, the torturous series continues.

Continued from Part 1, which establishes why outright fraud, not mere “getting off on a technicality,” would have been required in the Pfizer trial if the Worry Window were true.
This is Part 2: Before the studies, some wave-gazing. I ran out of time to address both waves and the studies; and I want to kick out a post on one of several other topics tomorrow before finishing this series.
What Is the “Worry Window”?
The Worry Window is the theory that injection with the experimental Covid vaccines has a magical property of increasing infections immediately after the first dose, and that this magical property is either magically self-hiding in most of the data on post-injection-infection-rates or has been systematically hidden by guilty researchers who know that the Worry Window is real.
Because the Worry Window is real (per the theory), all reported values for infection rates in the Covid vaccinated are not valid. Real Covid vaccine infection efficacy is probably always negative.
What Isn’t the “Worry Window”?
Real.

iv. Look at the waves!
I don’t want to look at the waves! But ok.
Post-emergency-injection waves are widely held to have been exacerbated by emergency injection roll-outs — countries that injected experimental gene therapy vaccines earlier and harder had more infections, is the general claim. Likewise, the authorization of triple-dose “boosters” in mid-August is assumed to have worsened Delta waves.
This is a popular source of Worry Window Post Generator Material because it allows for mathematically torturing data to suggest a result discordant with what (I would assert) most people remember from actually experiencing 2021. There were apparently loads of people getting infected right after their first dose, despite the fact that no one could see them in real life.
(Anecdotes to the contrary are certainly welcome in the comments, but I had not encountered a single anecdote of post-injection-infection before July, 2021, when infection efficacy evaporated. And as previously stated, I am more impressed with the evidence for bivalent “boosters” promoting infections.)
At the same time, I don’t want to claim to “speak for” any specific Look at the Waves argument or post. Maybe no one has actually claimed the UK should serve as an example, even though I am going to use it as a counter-example. Oh well. It’s a counter-example.
Anyway, problems with the “look at the waves” theory:
Faulty premise.
It is not actually surprising that “Pandemic Winter 2” waves were more intense than “Pandemic Spring 1” waves in a lot of places. It would have been surprising if they weren’t.
The virus, perhaps owing to late acquisition of the B.1 mutation quartet which seems to have improved fitness vs. the Wuhan model, failed to get a foothold in 2020 until it was already colliding with warmer weather. At the same time, this left the virus off of footing for a summer wave.
Establishing seasonality is rough when you are a lab-grown, intentionally released coronavirus, ok?!
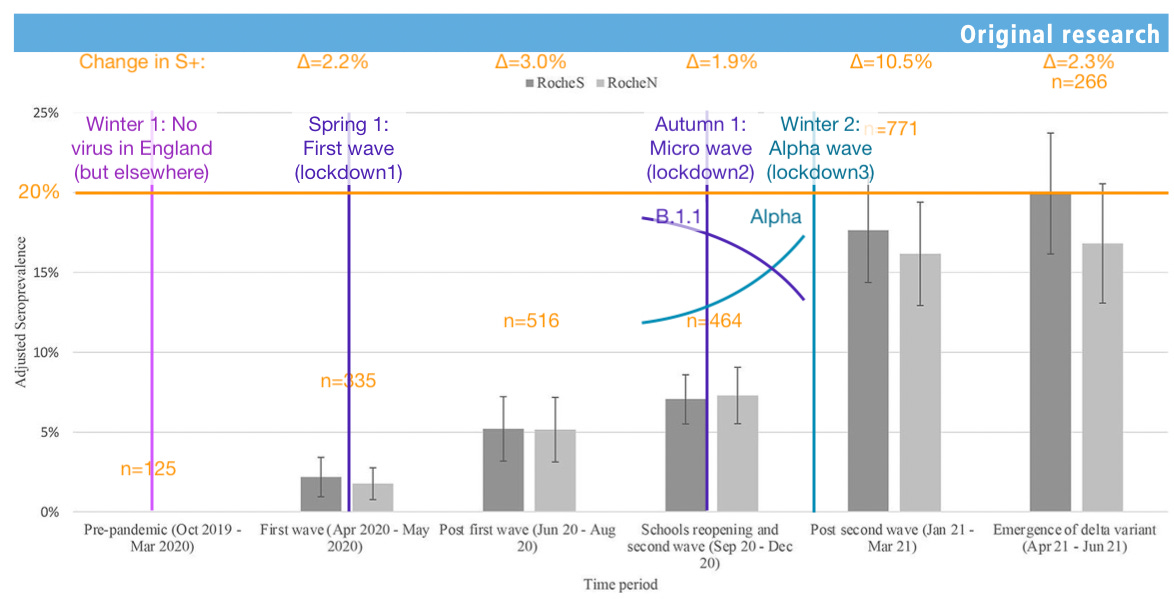
So there is no “need X factor to explain” as far as the winter wave. There was abundant fuel (non-immune individuals, or susceptibles) still left even after winter, since the virus tends to recede when seropositivity is still low in lockdown-compliant countries.1
The apparent resilience of regions with lower vaccine uptake to these increases can be ascribed to extreme differences that were already prevailing in this dynamic. For example, in urban Bangladesh, S antibody seropositivity in children residing in or near slums in Dhaka and Chattogram, Bangladesh was already 65.5% in samples taken between October 2020 and February 2021 (70% in adults).2 It should not be surprising that locked-down countries, which had faster access to the experimental injections (save for Australia), would primarily be the ones with gains in 2021.
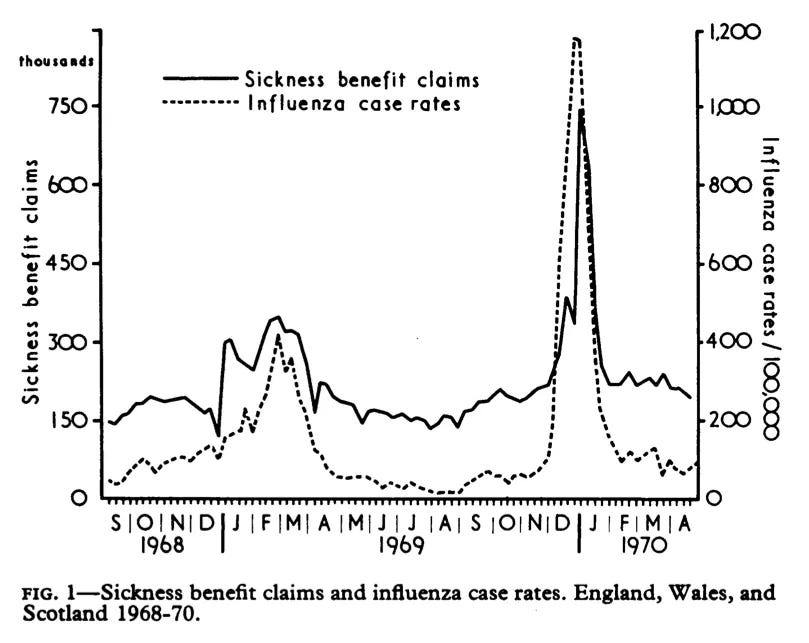
Finally, it is also not the case that prior, not-lab-released viruses have never had bigger second year waves than first year waves. Besides probably happening all the time but not being obsessively measured, it was also observed for the 1968 H3N2 flu.3
Any assertion of a maxim to the contrary, similar to claims that “viruses want to get milder,” is simply a modern evolutionary meme without evidentiary basis. Humans don’t know what viruses want to do. We didn’t invent them (except this one).
Meanwhile, it is arguable at least for Alpha and Delta that these exhibited intrinsic fitness gains over the ancestral B.1 virus. There is no reason therefore to explicitly discount the other (more lab-reproducable) evolutionary meme that viruses undergo rapid fitness-increasing mutations after transferring to a new host as applying in this case; with the fact that no such rapid mutation occurred between B.1 and the “Variants of Concern” implying that they would represent the next step forward in that process.4
Look-at waves could happen too soon.
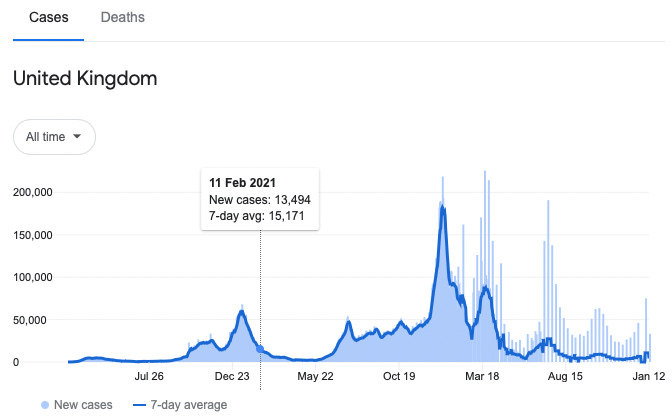
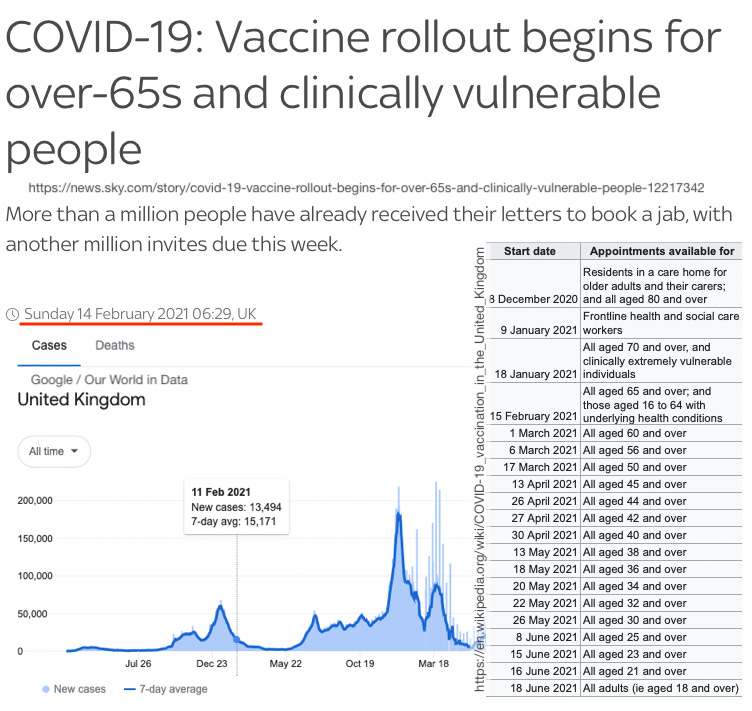
The 2020/2021 winter waves predominately would have been driven by age groups that were not yet eligible for injections. This is starkly visible in the “early”-adopting UK. The wave was over by the time the vaccine was expanded to those under 70.
It is thus not significant, to me, if Look-at waves are associated with some regions’ vaccine roll-outs (if broader adult approval is taken into account), or statistically there is some relationship between roll-out and Look-at waves. Look-at waves did not need people to (actually) get injected in order to happen, as in the UK.
If the reader is not satisfied with my dismissal of the statistical case, that is fine. It is still true that the UK experienced a larger wave sans mass Covid-vaccination.
Actual Worry-Window-influenced waves should have clear signatures in by-age infection rates. They don’t.
Here, we can stay in the UK, although the reversion of the Alpha wave before adults under 70 were eligible is problematic. There is nonetheless no signal in the Alpha wave for age groups becoming more infected. Meanwhile, what can be observed about the 20 year-olds is that the are already rising in infections at the beginning of the Delta wave (before approval), because unlike older groups, they do not have (temporary) infection efficacy:

Highlights:
80 year-olds experience depressed rates of infection vs. trend immediately after approval in this age-group and care home residents and workers.
70 year-olds experience depressed rates of infection vs. trend after approval in care home residents and workers, and nothing remarkable occurs after approval in 70 year-olds generally.
50 year-olds are approved during a minor bump in case rates in that extends the tail of the wave (a frequent feature of waves still dispersing to less population-dense areas after reverting in cities). However, they fall in with the older groups in not experiencing this bump.
30 year-olds do not reflect any apparent exacerbation of cases despite being approved as the Delta wave is beginning to show.
The elevation in 20 year-olds is consistent with their “natural” performance in the prior two waves, and with simultaneously not-eligible teens (in both prior and the burgeoning Delta wave). All that is different about the Delta wave in June is that older adults are not yet rising; they would rise later in staggered intervals, leading to the UK’s “forever wave.”
Summary: Because of age-staggered rollouts, the Worry Window makes a claim whose proof would essentially have no way to hide in the by-age data. However, it is not there.
The Worry Window is not a naturalistic interpretation of (alleged) associations between injection and waves.
If waves follow injections, that would be naturalistic evidence suggesting that Covid vaccines inject literal SARS-CoV-2 virus.
This conclusion, for some reason, is never acknowledged by the Worry Window purveyors as an alternate possible explanation for the (alleged) association of waves and injections. After all, no one wants to be labeled a “conspiracy theorist.” So “immunity 101” is carted in to provide the explanation for the allegedly proven association.
Of course, actual injected-virus would lead to easily-verifiable, widespread observations of by-age fluctuations in infection and death, as well as of universal anecdotes of test-confirmed post-injection-infection. They aren’t there. No one, I assert, would find this conspiracy theory to match observed reality (regardless of its intrinsic plausibility or lack thereof). “Look at the Wave” arguments for the Worry Window ought to be held to exactly the same standard of skepticism, regardless of whether that theory is more “science-y” than an outright conspiracy theory.
Next: The studies, for real this time.
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Ratcliffe, H. et al. “Community seroprevalence of SARS-CoV-2 in children and adolescents in England, 2019–2021.” Arch Dis Child. 2022 Jul 20;archdischild-2022-324375.
with inset for Alpha dominance loosely derived from
Volz, E. et al. “Assessing transmissibility of SARS-CoV-2 lineage B.1.1.7 in England.” Nature. 2021 May;593(7858):266-269.
Editors. “Higher COVID-19 seropositivity observed among residents in Dhaka and Chattogram.” (2021, June 22.) icddrb.org
Miller, DL. et al. (1971.) “Epidemiology of the Hong Kong/68 Variant of Influenza A2 in Britain.” British Medical Journal. 1971 Feb 27; 1(5747): 475–479.
Simmonds, P. Aiewsakun, P. Katzourakis, A. (2019.) “Prisoners of war - host adaptation and its constraints on virus evolution.” Nat Rev Microbiol. 2019 May;17(5):321-328.
The peculiarity of the evolutionary leap between B.1 and the VOCs was discussed in “The (2020) Variants: Not Guilty.”
Continuing my rant... if you have got your worry window exposition out of your system Brian.. I wish you could refocus your copius neurons on questions of immunology. What questions? Maybe you saw this piece; https://www.eugyppius.com/p/the-history-of-failed-hiv-vaccine
Title: The history of failed HIV vaccine trials confirms that overvaccination causes class-switching towards non-inflammatory IgG4 antibodies, reducing the effectiveness of the immune response
My sense is that there is something we are missing when it comes to the conditions that invoke IgG4. The Eugyppius post shows that we should have known, in some sense, that injecting epitopes isolated away from the viral whole was somehow a bad idea... and these (HIV gp120-related) proteins weren't even self-replicating.
Since the substack post is paywalled, the paper of interest is here;
https://www.researchgate.net/publication/260950633_Polyfunctional_Fc-Effector_Profiles_Mediated_by_IgG_Subclass_Selection_Distinguish_RV144_and_VAX003_Vaccines
These folks dance around the question, and basically admit we don't know why our immune systems treat "allergy" antigens differently (eventually invoking IgG4) vs. viral antigens.
"The uncharacteristic induction of high levels of IgG4 in the alum based VAX003 regimen may be related to the repeated administration of seven large doses of vaccine antigens in the absence of sufficiently potent adjuvant signals that may have driven excessive B cell receptor triggering. Allergy studies have similarly observed that continuous exposure to high doses of antigen can result in suppressed inflammatory responses through elevated levels of antigen-specific IgG4 (28). However, little is known about the mechanism by which vaccines tune Ab subclass selection."
Little is known indeed.
I never heard of the worry window. I always did think it was strange that they didn't count people as vaccinated until after 2 weeks. Looking at the UK waves, respiratory infections are seasonal. I think that's why they released the vaccine in November and December, because respiratory infections were likely to go down in the coming months.