


TASD Contents; On severe efficacy denialism
Brian "punches back" on severe efficacy and Paxlovid; it gets spicy!

Now that the “Tolerance and severe disease” series is complete, a table of contents has been added to all posts.
This post is both to announce the change and to invite readers who found elements of the series off-putting to observe that there was a point to all parts:
Contents to “Tolerance and severe disease”:
The myth of secondary bacterial pneumonia.
Sky-high rates of antibiotic use among hospitalized “Covid-19” patients.
The case for inflammation being (mostly) a bystander to Covid-19 pneumonia, not the cause.
I could not offer my theory for why the Covid vaccines may doom children to a lifetime of persistent infections with potential downstream cardiac risks without dismantling a ton of myths, including, yes, myths that Paxlovid and the injections don’t appear to reduce (rare) severe outcomes in older adults (that’s in Part 2).1
Nor could I make my case while cramming every single section full of caveats and context.

Severe efficacy is real, but was never the final word on whether “jabs bad”
For example, when it comes to severe efficacy for the Covid vaccines, my position has always been that this does not mean anyone should take them. Even in the most “high-risk” groups, most people do not progress to severe disease. Most individual people therefore cannot benefit from severe efficacy; they can only incur the added risk of the experimental transfections. I have said this a million times; I am saying it again now.
With that said: The evidence for severe efficacy in adults (not kids) is consistent and robust2 (retroactively; going forward, if the IgG4 situation for example becomes worse and worse, things may change*).
You are certainly welcome to imagine that this evidence is somehow all and everywhere an artifact of healthy user bias and fraud. (However, if you are under the impression that this assertion has been actually demonstrated by anyone to be true, you are incorrect. It remains a naked assertion substantiated with “razzle-dazzles” made out of data artifacts or flat-out errors.)
But what you cannot do is engage in true debate against the Covid vaccines if all you can bring to the podium is denialism about the evidence for severe efficacy (as opposed to cost-benefit and risk-based arguments); denialism is a one-sided anthem, it is preaching to the choir in the church of spaghetti monsters.
*And when it changes, I will be first in line to point out the same. Because my position on severe efficacy has never been about what I “need” to be true.
To be clear: I am not injected with the idiotic stupid poisons; nor am I so worried about my choice to be not injected with the idiotic stupid poisons that I have to constantly invent wild excuses for why severe efficacy is not real; I have no dog in the “do idiotic stupid poisons work” fight. I only care about the subject because it helps illuminate what the disease “Covid-19” is; i.e. it leads to better understanding of the virus and its host’s response in past, present, and future.3 If nothing else, insane, reckless medical experiments on the entire human race are good at producing knowledge (weird but true).
Accusations of “shilling” for Paxlovid are silly nonsense
Paxlovid is a therapeutic, and appears effective at reducing severe outcomes (particularly in the unvaccinated).4 And yet advocating for use of Paxlovid as something that, like HCQ and other interventions, make the experimental Covid vaccines a stupid and redundant medical risk, somehow seems to touch a nerve in the Covid vaccine skeptic space. (I’m not even advocating for it; but as with the Covid vaccines, merely acknowledging effect of a medicine is presumed to be “advocating,” which I would like to point out reflects internalization of medical dependency; i.e. “if medicine X works, everyone must have to take it.”)
After all, “It’s got ‘Pfizer’ on the box! Pfizer bad!”
I would like to remind readers once again that Pfizer is not instrumental in the development or deployment of the Covid vaccines. They don’t even know how they work, and they don’t care. Their role in the “trial” was totally perfunctory; just as was the FDA’s; just as was Trump’s. All of these organizations and individuals are just puppets dancing on strings pulled from above, performing a pantomime of “regulation” and “regulatory capture” 🐴 to distract from overt military countermeasure deployment.

Paxlovid-suspicion essentially has no coherent place in a worldview that perceives Pfizer and the FDA’s irrelevancy in the grander scheme. Yes, it causes rebounds, which is hilarious (but also biologically cool). Yes, it is a corporate handout and there are arguments to be made that suppression of cheaper alternatives is still costing lives. Yes, it too may be a military countermeasure. However, I would note that chloroquine, rather than HCQ, is (I believe) recommended in China, and there are no mRNA vaccines, and yet Paxlovid is in high demand. Make of that what you will.
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


The original version of this post used “ton of stupid myths;” I removed “stupid” in edit because it does not apply to all topics, i.e. both “myths and stupid myths” were tackled in the series.
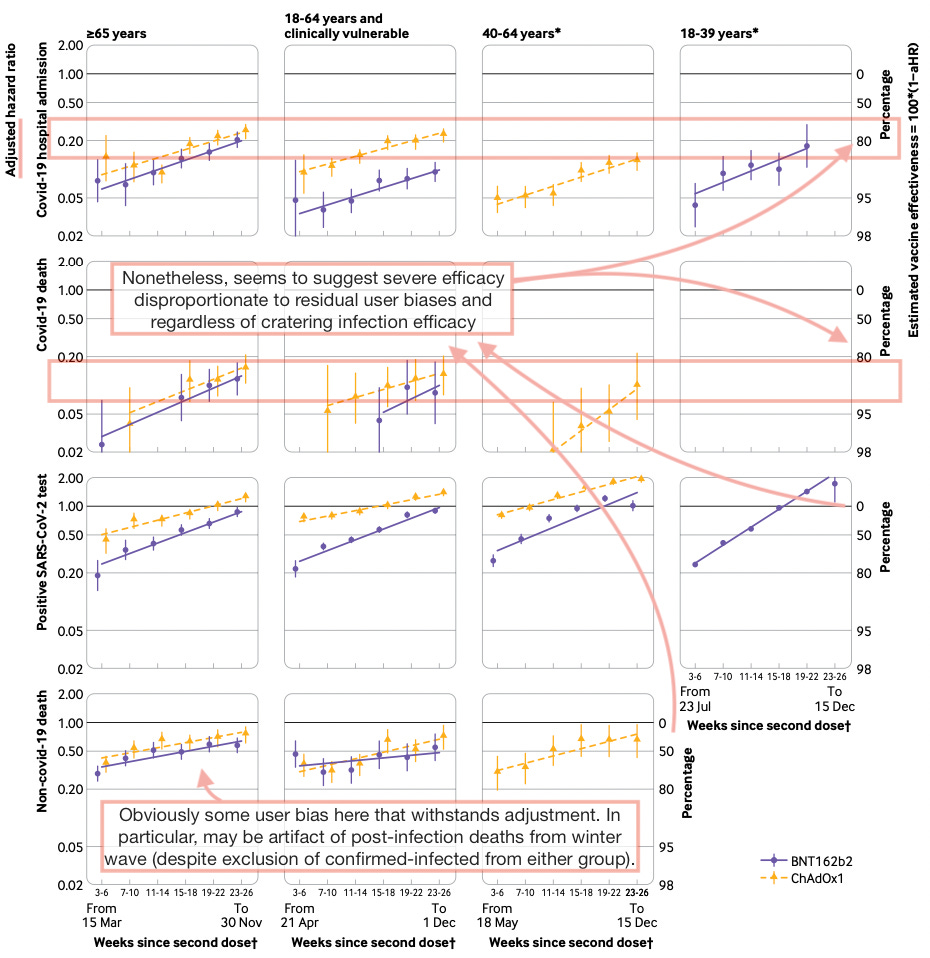
So much so that citation is not required. However, I generally regard Horne, et al. as the best quality real-world study for outcomes in 2021:
Horne, EMF et al. “Waning effectiveness of BNT162b2 and ChAdOx1 covid-19 vaccines over six months since second dose: OpenSAFELY cohort study using linked electronic health records.” BMJ. 2022 Jul 20;378:e071249.
As for severe efficacy after November 2021, i.e. in the Omicron era, this is difficult to discern due to the unvaccinated “control group” having all gained natural immunity by now; the statistically chaotic quality of “boosters;” and the putative milder-ness of the Omicrons (which may have deattenuated by now, without any way to tell due to the previous two factors).
Any claims about negative efficacy that don’t take the currently-dominant “catch-up effect” into account, however, are of poor quality.
For example, did the second little piggy have “negative wolf efficacy” because on day 2, only his house was being blown down? Or was it a wash (it was a wash)?
Last year I also considered the severe efficacy question important for arguing against boosters. i.e., you couldn’t argue that severe efficacy was holding out ok and that repeat injections were therefore futile if you didn’t acknowledge severe efficacy to begin with. However, at this point, round 3 and 4 boosters are a lost cause, and the people still going back for more are also a lost cause.
To recycle my citation from pt. 2, the trial has now been partially substantiated by a few real-world studies, though all of these have their own potential biases including healthy user bias:
Evans, A. et al. “Real-world effectiveness of molnupiravir, nirmatrelvir-ritonavir, and sotrovimab on preventing hospital admission among higher-risk patients with COVID-19 in Wales: a retrospective cohort study.” medrxiv.org
-Note apparent healthy user bias in all treatments and in Covid-vaccination status.
Dryden-Peterson, S. et al. “Nirmatrelvir Plus Ritonavir for Early COVID-19 in a Large U.S. Health System.” Annals of Internal Medicine.
-Note <20 week since last dose group will have artifacts of changing age groups since two waves were observed, and the “second booster” was authorized in the first wave.
A third study has now made a big splash on this topic; however, this one is less impressive due to the “control” group including so many same-day hospitalizations (which Dryden-Peterson took care to exclude).
You've been putting out a lot of thought-provoking posts that have strayed from the consensus on both sides which is always needed.
I think the biggest issue is that new information tends to override older information, and instead it's the weighing of each evidence that's important.
The biggest problem with the vaccines weren't efficacies but uncertainties in adverse reactions which became more apparent after more time. It was only later that we gained more evidence of the vaccines not being sterile even though that probably should have been the assumption from the start.
The same goes for PAXLOVID. We didn't have to argue that PAXLOVID didn't work. Instead, the argument was that there was a message other treatments did not work, and therefore you can only rely on PAXLOVID and Molnupiravir for at-home treatment. In this case it was the inability for doctors to prescribe things that was the issue.
Then take that into monoclonal antibodies which everyone assumed was the best thing that should have been used widely, then a little study comes showing very low dosage of monoclonals may induce ADE in very specific cell lines (inherently a very limited study) and all of a sudden people are suggesting that monoclonals were always evil.
I think a lot of this may be more reflective that many people are being exposed to information but aren't quite parsing or reconciling with it constructive manner. Just throw information at some people and it can become the new narrative.
I appreciate that you're being scientific about this Brian. I agree that the shots seem to have kept some people from infection, severe covid and death. With you I didn't want to try the gene therapy, betting instead on my immune system with some therapeutics. Ok so maybe Paxlovid saved some people from a bad case of covid. Again, let those who want it try it. But I wasn't going to.
What's unethical was the stampede to mandate the gene therapy and now to push it at pregnant women, infants, everyone. But hysterics and unbased claims from the anti-vax camp don't help.