
Omicron did not change whether the vaccinated make N antibodies
Rebutting a silly claim.


Alex Berenson (who, thank God, seems to have finally discovered that not just his iPhone can be used to generate screen-captures for blogs, any actual computer can do it too) has just advanced a bold theory regarding Omicron and N antibodies.
He has done this in response to the surge in N positivity in blood donors sampled by the UKHSA starting at the very end of last year.
In countries that didn’t use the mRNAs, N-antibodies rose much more quickly as Delta spread in 2021. An Indian survey found that almost 40 percent of people had detectable N-antibodies by mid-2021, almost three times as many as in Britain [read: in self-selecting UK blood donors; not a survey] at the time.
But just as they do not stop Omicron, the mRNAs also do not stop most people from developing anti-N antibodies after Omicron. Surveillance data from the United Kingdom shows that after barely rising for much of 2021 despite repeated waves of coronavirus infection, levels of anti-N antibodies soared in 2022.1
Berenson is wrong; both his premise — that “the mRNAs” ever stopped anyone from making N antibodies after infection — and his reconciliation — that Omicron reversed the drag in N positivity in donors — are not correct.
N antibody controversy timeline
For newer readers, who may not remember why they subscribed and may not understand why they are reading anti- “The Official Anti-Covid-vaccine Narrative” dissent in an anti-Covid-vaccine journal, here is the timeline of events:
October, 2021:
The UKHSA observes that N antibodies aren’t rising very quickly in blood donors. They toss off a comment that “recent observations” show the Covid-vaccinated not making N antibodies, with no source whatsoever.

As classic as the Coca-Cola logo. Source: gov.uk (pdf, landing page) Berenson proposes that this comment is a cosmic edict revealing immune dysfunction in the Covid vaccinated:2


Ok, but:
Who said anyone in the UKHSA blood donor set was infected?
Again, what source was there for the “recent observations?”
So this is simple reading comprehension being tested here. A remark about “recent observations” after infections being attached to the chart doesn’t make the donor pool in the chart reflective of responses after infections. The authors of the UKHSA comment have no idea whether their donors were infected or not. They are authoring words, not authoring facts. Berenson, at best, should have said, “Provocative theory from the UKHSA — But it is based on very weak data. Since we don’t live in the world where literal donors don’t automatically introduce bias, I would like to see a study that looks at this with verified infection.”
Wait — Just how does one know that there is bias in the donor set? Well, look back at the graph from October, 2021. The S positivity (and hence Covid-vaccination rate) was virtually 100%.

Oh. That… looks like bias. Injection coverage in adults at the time was reported from between 55% to 95%, depending on age group.3 55 to 95 is not ~98. Because the unvaccinated did not donate, the donor pool self-excluded a quarter to a third of all adults.
So if donors do not represent the UK at large (no non-vaccinated), there is also no guarantee that they represent the Covid vaccinated at large (no post-vaccine infected, recovered). If one exclusion bias is possible (and proven), so is the other. (The donor pool could have been excluding the portion of Covid-vaccinated adults who had “breakthrough” infections in the summer.)

October, 2021 part 2:
I immediately take the counter-bet. The Covid-vaccinated can make N antibodies just fine. The UKHSA comment was an artifact of sampling bias and bad word choice.
The other portions of the statement, meanwhile, strongly argue against extrapolating from the blood donor seroprevalence charts to the rates that would be found in the general population. The sample, again, likely selects both for high rates of Covid-vaccinated and low rates of post-infection donors (with the latter bias increasing with age).4
(This marked the beginning of my crusade to dismantle the stupidly named, fraudulently conceived myth of “Original Antigenic Sin.”5)
December, 2021:
“Omicron” (BA.1) becomes the dominant variant in the UK. Donor N antibodies begin to rise more rapidly.
April, 2022:
I point out that donor N antibodies are now rising rapidly and my “bet” is on course to being the winning one.6 The Covid-vaccinated can make N antibodies just fine.
October, 2022:
Berenson notices that donor N antibodies are now quite high. Instead of publishing an acknowledgement that his initial “urgent” remarks were refuted by reality, he proposes an X factor that rescues his initial remarks: Omicron itself. Thus, the “urgent” remarks were correct in the Delta era, but not in Omicron. Now reality owes him an explanation for this incredible mystery.
First, how much of a role has the increase in anti-nucleocapsid antibodies played in reducing the threat of Covid? Second, why are vaccinated people more likely to produce those antibodies when they are infected with Omicron than with Delta? What changed?
And now the reader is up to date.
The genius of the X factor
Berenson’s proposal that Omicron restored N antibody seroconversion is brilliant for turning a loss into a win. Instead of, “The rise in antibodies observed after Omicron proves I was wrong that the Covid-vaccinated can’t form an immune response to infection,” Berenson offers, “The rise in antibodies observed after Omicron proves I was right that they weren’t being generated before.”
As we will see, this once again is a case of making conclusions about what happens after infections without taking actual infections into account.
So: What Changed
Answer: Not much.
The apparent effect of Omicron on (donor) N antibodies needs to be normalized to the effect of Omicron on rates of infection. There are multiple ways of doing this; I am going to default to the crudest possible.
I have endeavored not to distort the data to my own benefit; the reader is nonetheless encouraged to consider me an interested party waging one side of an argument, if not a hostile witness. Another person could potentially present the data in a way that seems to come up with a different result. Feel free to try for yourself.
And so, here is the worldometers path for cumulative reported SARS-CoV-2 cases in the UK, overlaid with the (month-old; they will update on Thursday) blood donor seropositivity rate.
I am using the age-stratified view, so we can rule out that an outlier age group is driving any overall trends.
Beware of the offset — I don’t like offsetting of graphs, but I also didn’t like how the 12-week average used by the UKHSA was “pulling cases from the future” (as shown by the 17-29 group circa week 25, 2021).
Finally, spring, 2021 was chosen as the “virtual 0” baseline to match the paths, since there were no infections going on at the time. Whatever effect the injections have on blood donor N antibodies before then is therefore not measured.
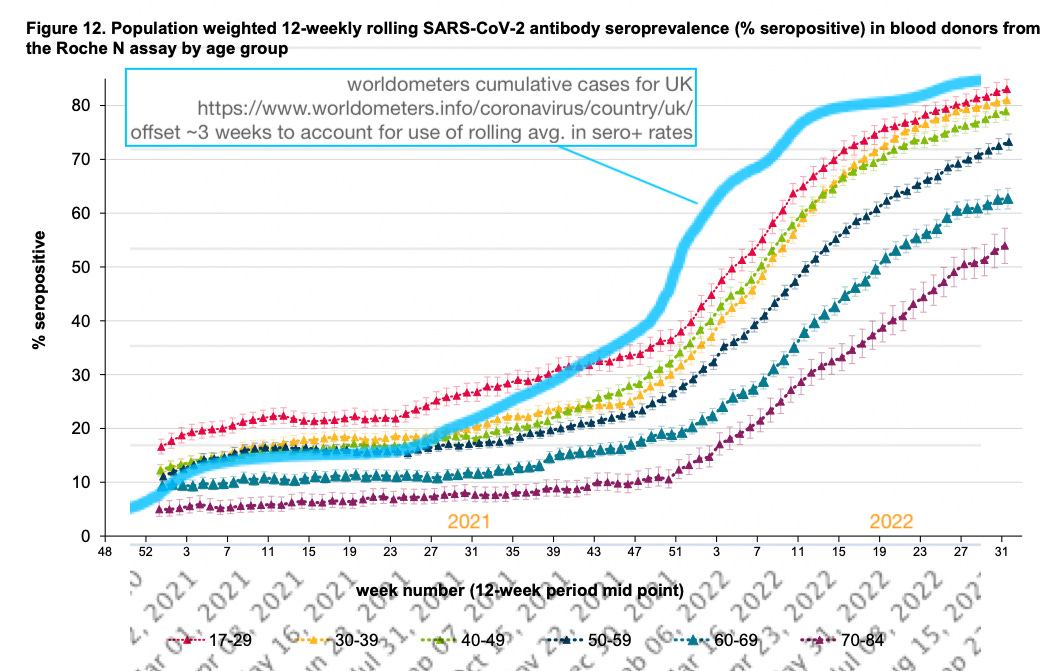
As we can see, the rate of N positivity after week 51, 2021 is rising, but still not at the normalized rate of cases.
Instead, N positivity continues to lag compared to case rates in the BA.1 portion of the Omicron era, and unsurprisingly outperform the case rate in the later Omicron era (because testing grinds to a near-halt!).
The surge created by the transition to the Omicron era is driven by more infections, not at all or not totally by a greater rate of donor N seropositivity per-infection.
Robust, precise “math doing” could probably tease out whether there is still some normalized per-infection increase. (Also, to be fair, cumulative infections will outpace cumulative infected more in the Omicron era thanks to reinfections.)
So I am not saying there is no potential change at all here; I am saying that the case-rate clearly drives much of the week 51 inflection. So much so that I am not sure it is worth anyone’s time to look into the question further.
Runner-Ups: Maybe a Little Change in Donor Biases
If there is still any change in the per-infection rate hiding in the raw numbers, consider that Omicron may have also adjusted the bias in the donor pool. In the Delta era, the Covid-vaccinated, infected were self-selecting out of the blood donation pool en masse; in the Omicron era, they stopped doing so.
Omicron could plausibly have removed two biases that were causing the UK blood donor pool to have an extreme bias for the not-yet-infected:
Now that “everyone” was getting the virus, younger infected Covid-vaccinated (previously and going forward) were less likely to perceive themselves as being a “failure.” This change in self-perception would influence behavior after infection. For it to influence an altruistic (and, in my lifelong opinion, frankly weird) behavior like donating blood is not implausible.
Now that the virus was less pathogenic, older infected Covid-vaccinated (going forward) were less likely to die or have a severe course of the disease that would exclude them from the donor pool.
I still believe that the first bias is important; it did exist, it was removed with Omicron: If not, I don’t know if the N antibody rate would ever have gotten so high in the young.
As for the older groups, they do not appear to show any add-on effect from a second “survival bias;” so I would say the “stigma bias” was the only or main driver for excluding the infected in this group as well.
Alright, This Blood Donor Nonsense Is Totally Dumb, Can We Just Actually Look at a Study of Whether Covid-Vaccinated People in the UK Made N Antibodies After Delta Infection?
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Berenson, Alex. “Goodbye Covid (part 2).” (2022, October 4.) Unreported Truths.
Berenson, Alex. “URGENT: Covid vaccines will keep you from acquiring full immunity EVEN IF YOU ARE INFECTED AND RECOVER.” (2021, October 21.) Unreported Truths.

See “(Not) Coming Up”
See “The Hot Spot”
'anti- “The Official Anti-Covid-vaccine Narrative” dissent in an anti-Covid-vaccine journal'
I think of you as our devil's advocate. Keeping us honest. From a dictionary: 'One who debates from a view which he or she may not actually hold, usually to determine its validity or simply for the sake of argument.' It's a valuable role.
It's kind of discouraging that so many on Team Skeptic expect everybody to hew to an identical narrative. That's one of the things we criticize about Team Mainstream Narrative, after all.
Not being a paid subscriber, I can't comment on Berenson's article, so I will inflict my sarcasm on you. He quotes some paper or other: 'Researchers [said?] that mice which produced both anti-N and anti-S antibodies had “better viral control [than those that had anti-S antibodies alone], including against the Omicron variant.”'
Well, duh!
At the risk of sounding stupid, am I the only one who thinks this is so patently obvious that it doesn't need saying? It's the reason why I initially became an mRNA vax skeptic, because natural immunity gives you *both* (and other good stuff besides), and PTB were claiming the spike-based vaccines had better protection.