


Polio series contents, and three post updates
"Are you saying that you know of a disease who's distribution in a given geography looks like an unending power law increasing to the right instead of a gaussian distribution with a peak and decline?"

Yes. (Duh.)

This post provides a table-of-contents for my polio series (it will be expanded with further updates, some planned updates are named here). It also provides three substantial updates made to previous posts.
The first update is the most relevant, since it corresponds to a challenge issued to my last post on the polio vaccines (in which it was shown that they worked). I was asked whether any disease has just increased without a “curve” over time; yes, this has happened, and several examples are shown. I write, in conclusion:
One does not suppose that when a door is closed, and the draft goes away, it’s just a silly coincidence, or a natural restoration driven by sacred mathematical laws.
The second update adds comments on why the symptoms of polio are inconsistent with “toxins” (no harm to more complex neurological functions like cognition and personality, which is often the first and most long-term symptom in toxic exposure).
The third update fleshes out the picture of how polio epidemics were not determined by statistics, but real-time observation of cases showing up to physicians and hospitals, promptly communicated to local governments and media over the phone.
This collection of updates might in fact serve as the best “starting point” for future readers who are new to the series, as they provide a wide-ranging sample-pack of what “thinking about the polio problem” looks like. Therefore new and old readers alike are (if interested in the polio topic) encouraged to browse (starting below the table of contents here).
Polio series contents:
Introductions to the problem:
Explaining polio:
Explaining polio, pt 1: The mechanism of polio provocation↗
Explaining polio, pt 2: The circumstantial case for provocation as the driver of polio epidemics.↗
Explaining polio, pt 3: But is provocation as the driver really plausible? (to be published)
The polio vaccines worked.↗ (Further expanded below)
IPV, OPV, or natural virus: Which is better long-term? (to be published)
We can never stop vaccinating: If polio goes away, it can just come back (evolution from related enteroviruses or lab release). (to be published)
(The problems with) alternate theories:
What polio is not:
Survey of (non-conspiratorial) explanations that fail to explain polio:↗
Hygiene↗
Misdiagnosis (lab verification verified polio; another example is in the reclassification section below)↗
Genetics↗
Transportation↗
Imagination / Over-reporting↗
Medical intervention (it was only partially this)↗
Evolution of the virus (it may have partially been this) (to be published)
The polio “toxin” theory
Pt 1: Problems with the theory.↗
Doesn’t match symptoms (focus on lead theory)↗
Doesn’t match timing↗
Doesn’t match immunity↗
Doesn’t match the disappearance of polio right after the vaccines↗
Also, DDT was sprayed into millions of homes and polio did not increase (focus on DDT theory)↗
Pt. 2: The polio vaccines worked.↗
Polio was trending upward (US) or was level (global) before the Salk vaccine, not downward↗
Vaccinated kids had less polio in all Salk-era epidemics↗
An earlier vaccine also worked, and could have been used↗
Pt. 3 (to be published):
Of course polio epidemics were associated with agricultural activity and exposure to chemicals (because this is what Americans did for a living at the time)
General problems with Turtles’ approach to the evidence and to the reader in the polio chapter
The polio “reclassification” theory
No or very little reclassification occurred:↗
No increase in “alternate” deaths after polio deaths disappear↗
What lab verification looked like when epidemics happened before Salk↗
What lab verification looked like when epidemics happened after Salk↗
Update 1: The decline of polio after 1954 should not have been expected (in US or globally) — and in fact was not expected.
This update was made to the most recent polio post, “The Polio Vaccines Worked.” Although the post generated only limited engagement, there was one challenge to my conclusion issued mere seconds after publication (this is not a way to demonstrate that the post has been read and all arguments considered).
The commenter in question took me to task for suggesting that the yearly polio trend in 1954 should have continued, apparently believing that such a thing was impossible under epidemiological laws.
"Are you saying that you know of a disease who's distribution in a given geography looks like an unending power law increasing to the right instead of a gaussian distribution with a peak and decline?"
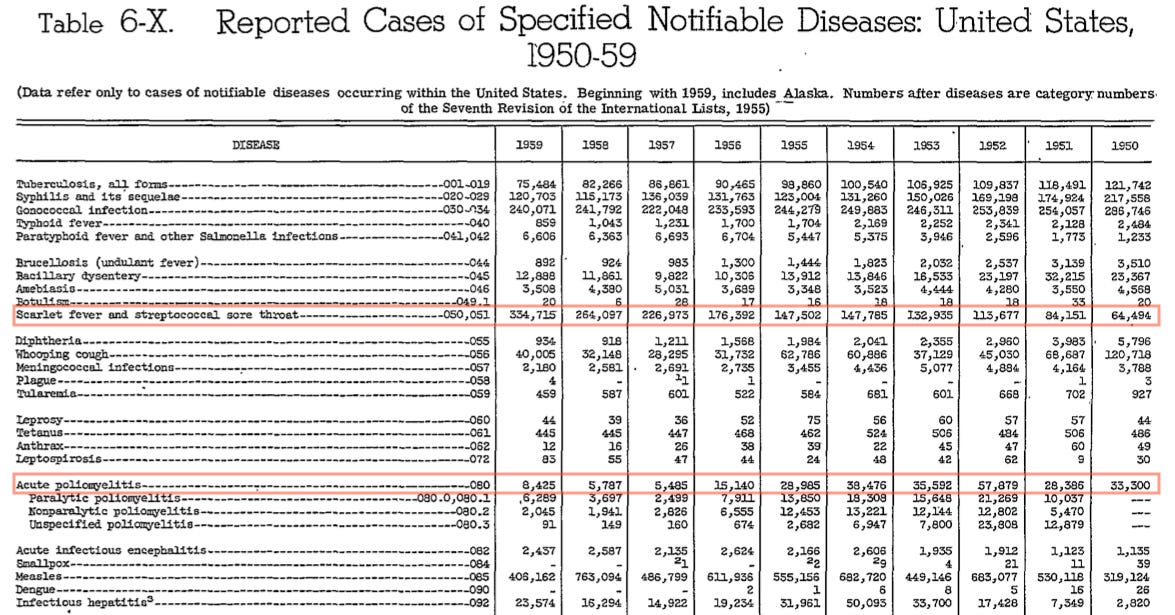
Examples are shown below from the US during the time period of polio’s rise and decline — so yes, I do “know of a disease” that does this. Parenthetically: It was also true of diphtheria in the late 19th Century, almost everywhere in the West, though reliable statistics are limited to England and Sweden.

As for the specific question of what should have happened with polio after 1954, there are myriad circumstantial reasons why, no, it is not plausible that cases would have declined substantially — rates would likely have plateaued at some level, eventually, but this plateau could have been much higher than the record year of 1952 (or it could have been some amount lower; but it would not have been zero).
Those specific, circumstantial reasons are given below — but I refused to discuss any of them in the comment thread in question, as to do so would have validated the false premise that I “need” to do any such thing (because of an incorrect notion that polio had to decline at some point):
Just a Curve™?
I received pushback in the comments based on the impish notion that the American polio case trend of the early 1950s was merely the left-hand side of an Epidemiologic Curve™.
This is not an appropriate or valid way to interpret year-on-year case rates. “Epidemiologic Curves™” operate on the scale of days and weeks — including for polio (literally, see the curves in the urban Salk-era epidemics above). And yet:
They are not an iron mathematical law which must (absent mechanical justification) apply to anything labelled an “infectious disease” at all times.
They have no great relevance for yearly rates, especially when tracking polio over a large area (polio was extremely heterogeneous in geographic distribution).
Regarding (1), “Curves™” are habitually irrelevant when it comes to most infectious diseases in the tropics. For example, even a so-called “epidemic” of Dengue Fever will tend to present without a bell-curve distribution.

The acolyte of “math rules epidemiology” might counter that, well, tropical, insect-borne viral illnesses are subject to special rules: Very well, such a cop-out merely verifies the more important point: Mere “epidemiologic-ness” and mere “infectiousness” are not the limit of considerations in how infectious disease cases should be distributed over time. Other stuff counts. “Other stuff” could be insects, or it could be human interventions… like the polio vaccine.
For polio specifically
The tendency before 1947 was for particular regions to go several years between relatively large epidemics. The tendency afterward was for regions to experience epidemics multiple summers in a row. Polio transitioned from highly sporadic to semi-sporadic. This transition was the engine driving an increasing baseline underneath yearly variability (light and heavy years relative to the increasing baseline).
This was simply an observational reality. No one observing it in 1951-54 could have, or did, predict that “Relentless Polio” must simply cease to be observed in precisely 1955, or any other year, because Look This Math Law. Relentless Polio — constantly increasing cases — was simply the “new normal.”
One thing to note about the constant increase in American cases in the early 1950s is, as noted in part i, a substantial heterogeneity. Because in the 1952 surge for example the East Coast was rather uninvolved, nothing about the selfsame surge could have prohibited new, record-high epidemics in the ensuing years — given that the East Coast had traditionally been the flag-bearer for polio epidemics in the US. (No such epidemics happened; but here the Salk vaccine plausibly can claim credit for preventing the falling of the shoe in question.)
This same heterogeneity was the one-and-only “rule” that could be applied to polio — and it meant that wherever cases were collated nation-wide, there were no “rules” dictating that yearly increases must reverse. There was plenty of unspent fuel in 1954, everywhere.

(How much spent fuel? This could be litigated by sero-surveys, which give an idea of how many people have accumulated natural immunity; except that few took place in 1955, and reliable comparison to historic antibody rates before 1950 are not possible.)
Anyway, it remains that in certain select regions, in the early 1950’s, polio cases did increase year on year. As polio don William Hammon wrote in late 1952 (emphasis added):
The great severity of the disease in the Sioux City [Iowa] area [in 1952], as judged by the high proportion of bulbar cases, the extent of paralytic involvement, the high case fatality rate, and the phenomenal morbidity rate (greater than 400 per 100,000) in the wake of six consecutive previous epidemic years (see this issue, page 750) testifies to the great invasiveness or virulence of the strain or strains active in this areas1
In other words, polio researchers in the early 1950s were quite resigned to the fact that polio was increasing in general. They did not bluster and protest about any iron laws that, any day now, would spontaneously return annual polio case rates to zero.
But, why not?
Because no such iron laws exist.
Yearly trends in infectious diseases are not defined by iron mathematical laws. They are a complicated product of billions of discrete interactions between the pathogen, host, environment (climate, bystander organisms, etc.), and reporting trends.
As such, literally nothing can prohibit the ceaseless increase of any particular infectious disease, beyond such mundane, pragmatic principles as “there is a limit to everything,” and “nothing lasts forever.”
Should polio’s increase have reversed in 1954?
Or have gone on for another decade? What does comparison with other diseases say? Here are four others:

Two of these diseases undergo increases which reverse more quickly than polio — but due to specific interventions (DDT for typhus fever, and a broad campaign of dairy policies for brucellosis). Two others simply plow forward, increasing without end — no control efforts are available.
So to which category does polio belong? Given that, like typhus fever, the reversal in increasing cases took place exactly when a specific preventative was placed into use?
This question isn’t even serious.
Even supposing that “iron laws” demanded the reversal of the American polio increase of the 1950s, the coincidental timing is too much to swallow. Why didn’t the reversal happen in 1948, or 1950, or 1953? Just what was it that made the reversal “wait” for the Salk vaccine? (Answer: The fact that the Salk vaccine was needed to effect the reversal.)
The ceiling on increase
Theoretically, the ceiling on infectious disease incidence is the population itself (or however many are added to the population per year, when measuring yearly).
The above graph represents all respective disease notifications, firstly, as a percentage of their average in 1935-1944. Although polio climbs the highest in this way of looking at things (i.e. in percentage), it never comes close to the absolute increase in yearly cases for “scarlet fever / strep throat” (shown in the second graph). For some raw numbers:
The all-powerful importance of “other things” in yearly trends (and which “other thing” caused the polio increase)
Hence the absolute absurdity of suggesting that diseases should follow “Epidemic Curves™” in yearly trends. These same trends are only partly a manifestation of the same dynamics which drive the time-distribution of cases during discrete outbreaks (i.e., increased cases lead to depletion of susceptible people to have cases). Many diseases are in equilibrium — a similar number of new susceptible people are infected and “depleted” every year — but not all. Disequilibrium does not demand a return to any particular mean, because it may be driven not by the dynamics of discrete outbreaks, but by “other stuff.”
“Other stuff” includes increased population (due to migration or high birth rates in a given area) or vice-versa; increased reporting or vice-versa; increased host susceptibility or vice-versa; and increased virulence of the pathogen responsible for the disease. Only the last of these is not subject to human social influences; as such, yearly disease trends tend to be like yearly statistics for any other social measurement (such as crime, etc.). The screen-grab above depicts the very first years in which infectious hepatitis was a reportable disease; the dramatic increase in cases mostly reflects subsequent changes in medical awareness and reporting.
Back to polio
The point, with polio, is that there is no prima facie justification for supposing that the trend of increasing cases should have reversed naturally.
In fact quite the opposite: Polio’s increase was driven by all three of the non-pathogenic “other things” listed above — more people, more reporting, and higher rates of susceptibility2 — and potentially by pathogenic factors as well (increased prevalence of virulent strains in the 1950s).
To suppose that all three (or four), let alone any one of these things coincidentally ceased to be a factor in 1955 exactly is an extraordinary claim requiring extraordinary proof. Which is to say, the Salk vaccine does not need to be defended against such fantastic imaginary scenarios — when it was used (in the US and elsewhere), polio was reduced. One does not suppose that when a door is closed, and the draft goes away, it’s just a silly coincidence, or a natural restoration driven by sacred mathematical laws.
(Only the “reclassification theory” deserves a special mention, because it supposes an intentional coincidence of timing — but, again, the evidence disproves the theory.)
Update 2: The wrongness of toxin theory on symptoms
The second update was made to “The Polio Toxin Theory, pt. 1.” In this post, I initially provided two key flaws with the toxin theory in terms of accounting for what was frequently observed in polio (cases and epidemics): Timing, and Immunity. Only when this blog was besieged by Polio Toxin Truthers did an obvious third key flaw occur to me: Symptoms. To keep the post as a whole from sprawling, the addition only outlines the problem briefly:
Symptoms
In short, polio was too specific a disease to have resulted from “poisoning.” There is no plausible explanation for how exposure to a toxin could result in such a “sniper-like” blow to the motor neurons, leaving higher-order functions spared.
As already quoted above, children stricken with polio were, immediately after the acute phase, frequently observed to be of sound mind and good cheer, and more physically hale than would be expected. (Of course, this extremely frequent observation, repeated over years and years, isn’t even mentioned in Turtles.)
This is inconsistent with neurological poisoning, when mental and emotional disturbances are often the first symptoms.
In the case of lead poisoning, for example:
Children who survive severe lead poisoning may be left with permanent intellectual disability and behavioural disorders. At lower levels of exposure that cause no obvious symptoms, lead is now known to produce a spectrum of injury across multiple body systems. In particular, lead can affect children’s brain development, resulting in reduced intelligence quotient (IQ), behavioural changes such as reduced attention span and increased antisocial behaviour, and reduced educational attainment. Lead exposure also causes anaemia, hypertension, renal impairment, immunotoxicity and toxicity to the reproductive organs. The neurological and behavioural effects of lead are believed to be irreversible.3
Supposing that polio paralysis results from a particularly high dose of whatever toxin, either in a single dose or by chronic exposure, it should not somehow be the case that the neurological functions usually harmed first are then harmed least.
This suffices to give the reader a picture of the toxin theory’s problem with symptoms. (Obviously one could go on, but a single problem is enough.)
Within the nervous system, expression of CD155 (the polio virus receptor) during embryogenesis is limited to the same anterior horn motor neurons destroyed in cases of polio paralysis4 — thus explaining the “sniper-like” accuracy of polio’s neural injury.
Update 3: Is it plausible that statistical manipulation could have “hidden” polio? (No): Another realistic look at the response to a post-Salk polio epidemic
This update was added to the footnotes of “The Polio ‘Reclassification’ Theory,” as I felt it would be useful to supplement the first example Salk-era epidemic (Detroit) with another (Chicago). It ended up providing a much fuller illustration of the government and media attitude of the era, demonstrating that there was still a certain “hunger” for polio epidemics (as something to drive attention and prestige), just as in recent years there was a great “hunger” for reported cases of infection with SARS-CoV-2.
I also added a quote to the top of the post from the CDC’s chief epidemiologist, AD Langmuir, which directly affirms my claim that polio would have been reported by hospitals, the media, etc. no matter what standards were put into place in terms of official statistics. Together, these two narratives should provide the reader a good “feel” for what was realistic in terms of “manipulating” polio out of existence (i.e., no such thing was realistic):
[I]f poliomyelitis were removed from the list of reportable diseases in all States, an informal reporting system would develop overnight. Newspapers, teachers, various business enterprises, hospitals, nurses organizations, and other agencies would collect, pool, and exchange information on the occurrence of the disease, not because these agencies have control measures which they could institute, but because poliomyelitis is a disease of both local and national interest, and that interest will be satisfied with or without an orderly reporting system.
AD Langmuir, 19525
Chicago example:
A more realistic picture of how health authorities would have responded to polio epidemics, had not the Salk vaccine reduced the incidence of the same, is given in the account of the 1956 Chicago epidemic.
In this case, the authors use the 35 per 100,000 incidence threshold to (retroactively) conclude that the epidemic was magically an “outbreak.” This linguistic tic — which I haven’t encountered in any other papers — has no relevance for the real-time response at the beginning of the epidemic.
What the reader will note instead are two meta-considerations that guide the response: There is an ongoing taboo regarding injection provocation; it isn’t explicitly mentioned in these quotes, but is the reason for the statewide requirement of special permission to keep using the Salk vaccine after an observed rise in cases, as well as for the collection of vaccination history of polio cases. This is appropriate; one can only say that the concern that Salk vaccines would, if poorly timed, increase paralytic polio during outbreaks should have been more explicitly acknowledged to the public, who obviously would have demanded that injections stop. The second consideration is that the authors — Chicago’s public health vicars — obviously see this outbreak as a chance to peacock their epidemiologic feathers. This is important for understanding how aggressive laboratory confirmation couldn’t possibly reduce polio epidemics — public health officials would have only sought to use it to reify and validate their own alarmist policies, just as testing served to do for SARS-CoV-2.
Bundesen, HN. Graning, HM. Goldberg, EL. Bauer, FC. “Preliminary report and observations on the 1956 poliomyelitis outbreak in Chicago; with an evaluation of the large-scale use of Salk vaccine, particularly in the face of a sharply rising incidence.” J Am Med Assoc. 1957 Apr 27;163(17):1604-19. doi: 10.1001/jama.1957.82970520003013.
Overview
This is a report on Chicago’s 1956 poliomyelitis [epidemic], in which 1,111 cases of poliomyelitis (835, or 75.2% confirmed paralytic cases and 276, or 24.8% confirmed nonparalytic cases), including 36 deaths, were reported in Chicago residents in the city of Chicago. […]
Launching the response — no lab confirmation, no incidence threshold. Just “some cases happened.”
However, with the reporting of 13 more cases during the week ending June 28, we became aware of a sudden increase in the number of reported cases in Chicago. This awareness was based on a comparison of the 13 [mentioned cases] with the 2 cases reported in the comparable period of 1955.
Because of this we were desirous of vigorously intensifying our inoculation program. However, to continue our inoculation program, it was necessary that permission be obtained from the Illinois Department of Public Health, because of a directive dated May 25, 1956, which stated, “Inoculations with poliomyelitis vaccine can be continued into the summer until there is an increased prevalence of the disease. . . . Specific recommendations will be made for local areas with high incidence if indicated.” Hence, the Chicago Board of Health on July 2, 1956, transmitted to the Illinois Department of Public Health complete information as to the sudden increased prevalence of poliomyelitis cases in Chicago at that time with a request that a recommendation be provide permitting our continuation of poliomyelitis inoculations.
While awaiting this recommendation, one of us (H. N. B.), cognizant of the possible urgency of the situation, began to mobilize the total facilities under his direction [etc….]
Real-time case response: No reference to lab confirmation
The major problems facing the Chicago Board of Health were as follows: […]
To mobilize the personnel of the Chicago Board of Health at once into a well-integrated team, personnel being placed on a seven-day week, emergency basis, with all vacation and other leaves being canceled.
To aid in the coordination of the activities and the integration of the facilities of medical groups […]
To insure the immediate hospitalization of persons with suspected or confirmed acute cases of poliomyelitis as they were reported and to arrange for the later hospital care of the persons with acute cases in private hospitals after the acute stage had passed. (In this outbreak, 70% of all persons reported as having poliomyelitis were hospitalized in the Chicago Municipal Contagious Disease Hospital and 19% in the Cook County Hospital, 11% either were hospitalized in private institutions (7%) or their cases were not diagnosed and reported until after the acute stage was well over (4%).) […]
To evaluate at once the outstanding demographic characteristics of this outbreak, which were its presence predominantly in (a) children living in densely populated, lower socioeconomic areas, (b) the nonwhite population […]
Two weeks into the response: mobilizing lab verification post-hoc with “special provisions” — but no retroactive reduction of the cases already counted and hospitalized, nor of future cases
On July 16, 1956, representatives from the Public Health Service, Department of Health, Education, and Welfare; the Illinois Department of Public Health; and others met in Chicago to develop procedures jointly for obtaining as accurate and complete epidemiologic information as possible concerning every reported case of poliomyelitis in 1956. The data to be collected included the exact date of onset, paralytic status, history of previous tonsillectomy, clinical course, and the ultimate outcome of each case. Arrangements were also made for obtaining complete information as to any history of poliomyelitis vaccination, dates and site of vaccine inoculation, the site of first paralysis, if any, and its degree. Special provisions were also made for collecting and examining all necessary laboratory specimens from the patients. The Illinois Department of Public Health laboratory performed all of the routine diagnostic blood and stool cultures on these specimens submitted by the board of health.
Returning to the overview, we confirm that this post-hoc lab verification campaign made no difference to final case counts:
Of the 1,111 cases, virology reports have been received on 651. Of these 651 cases, a poliomyelitis virus has been successfully isolated from 412 [63.3%]
There is no way to imagine that implementing a just-in-time lab confirmation program (totally off the books) could, in future years, have made it so that 800 people became paralyzed routinely in the summer but no government or media response followed — especially if 2/3 of them would come back positive for polio virus anyway.
The only way to prevent observation of polio epidemics is to prevent occurrence of polio epidemics. The reclassification theory is idiotic.
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Hammon, WM. et al. (1954.) “Evaluation of Red Cross gamma globulin as a prophylactic agent for poliomyelitis. 5. Reanalysis of results based on laboratory-confirmed cases.” J Am Med Assoc. 1954 Sep 4;156(1):21-7doi: 10.1001/jama.1954.02950010023009.
This is indisputable given that while overall cases were increasing during the Baby Boom, the representation of adults among yearly cases was increasing as well.
Gromeier, M. Solecki, D. Patel, DD. Wimmer, E. (2000.) “Expression of the Human Poliovirus Receptor/CD155 Gene during Development of the Central Nervous System: Implications for the Pathogenesis of Poliomyelitis.” Virology. 2000 Aug 1;273(2):248-57.
Langmuir, AD. (1952.) “Usefulness of communicable disease reports.” Public Health Rep (1896). 1952 Dec; 67(12): 1249–1257.
In which, the chief epidemiologist of the CDC “confesses” that merely ignoring polio is not possible.
The probability of developing paralytic disease is oddly small that it seems there should be an explanation for vast communities with existing antibodies that did not suffer disease outbreaks. The provocation poliomyelitis theory is still interesting. I wonder if there is any merit to the possibility that disease development could be linked to toxins/viruses/etc. that are chronically demyelinating and/or inflammatory but not necessarily to an extent of presenting other acutely recognizable degeneration. It seems key that polio can pass the BBB and attack the anterior horn. How does it get there? The body first needs a red carpet to be able to roll one out.
There are certainly other mimics (AFP, Guillain-Barré, etc) where demyelination is a paramount mechanism to symptoms, as well as other enteroviruses that have similar presentation. Guillain-Barré handshakes with pneumoniae; perhaps there is a similar synergy/comorbidity for polio. There have been some polio comorbidity studies, but all seem rather shotgun spray (ie laundry list of generally poor health markers), or they focus on sequelae.
Your work is always thought-provoking and interesting. Thank you.
Great summary, looking forward to Explaining polio, pt 3!