


Followup Roundup: 22.2.5
Removed IVF Paper, Masked kids in the news, and mRNA-ed up macaques


IVF Vanishing Act
Edit, February 7: The paper has returned online, with no apparent alterations to the negative results. But the black-out was exciting while it lasted…
As noted by Paul Lutz in a comment sent yesterday, the Aharon, D. et al. IVF outcomes paper reviewed in “Glass House” has been pulled from online, so that it can complete some unspecified “transition” regarding “changed information”:
Perhaps these edits will prove to be mundane (note that another recent article, reporting cycle changes for Covid-vaccinated users of a fertility app, has also been yanked1).
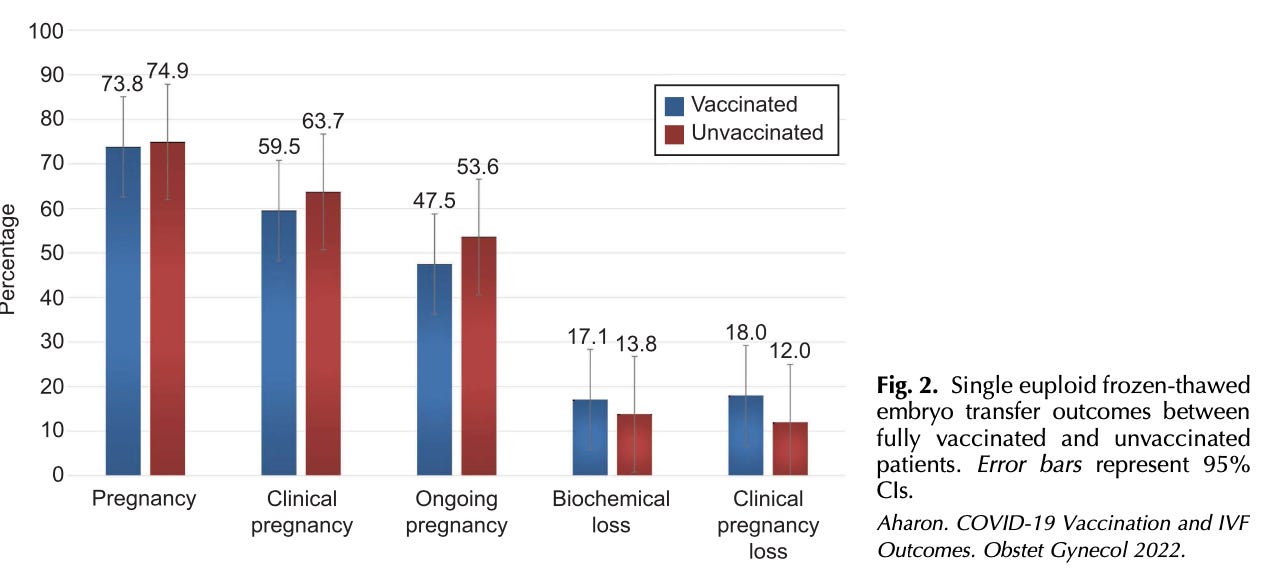
In the meantime, it is exciting to imagine that the lower success rate of frozen embryo transfers in the Covid-vaccinated is being literally erased from the document, memory-hole style. Oops, we made the vaccine look bad:

Virginia is for Maskers
A Virginia court has provided an unwelcome affirmation of my Black Pill take in “The Vulgarity of Normal,” suspending the Governor’s mask-optional executive order. The court decision isn’t really substantial in of itself, as it merely constitutes a rational reading of the Virginia constitution. As judge DiMatteo said during the hearing, “I’m not here to decide who is right and wrong on masking. This case is a question of who has authority.”3
In the case of Virginia, the constitution vaguely divides authority between a state Board appointed by the Governor and confirmed by the Legislature, the Legislature itself, and local division School Boards.4 Whatever wiggle room there is in this document for judicial interpretation, it doesn’t include executive orders. So the suspension of Youngkin’s order is natural.
Nonetheless, the decision highlights the resilience and energy of the teachers and school officials who still support masking children. Seven school boards were involved in the suit (Alexandria City, Arlington County, the City of Richmond, Fairfax County, Falls Church City, Hampton City and Prince William County); Loudoun County’s defiance of Youngkin’s order prompted a suit in the opposite direction from parents; and the Virginia ACLU filed a separate suit irrationally claiming that useless mask-wearing is a prerequisite for “federally mandated” education access for the disabled (no, access is access).5
An Arlington school board press release,6 gloating over the court victory, complains in self-victimizing fashion that Youngkin’s order was forcing them to break an incoherent law passed by the Virginia legislature last summer demanding school boards follow CDC Covid-mitigation-recommendations to “the maximum extent practicable” (which itself voids the delegation of authority to local boards in the Virginia constitution, implying that the CDC is a chartered entity of the government of Virginia until expiration of the bill in August of this year7).
Prior to today’s decision, Virginia school boards were placed in a legally untenable position8 — faced with an executive order in conflict with the state constitution and state law. That conflict has also put the health and safety of our students and staff at risk, as the Omicron variant continues to affect Virginia localities.9 We are confident that the court will soon come to the right decision to resolve this pressing matter.
And yet, the board then appears to strike a conciliatory tone, referring to a “not-too-distant future” revocation of the mask mandates. But how is such a revocation possible, if the the school district is determined to insist that last years’ law obliges them to follow CDC guidelines over local judgment? As if to give up the game, the release simultaneously recycles the typical trope of the Covid Self-Hostage-Taking Public Health Restriction, insisting that unnecessary mitigation measures are necessary to avoid unnecessary total closures (emphasis added):
We look forward to a day in the not-too-distant future when universal mask-wearing is no longer needed as part of our layered health mitigation strategies in order to keep our schools open for in-person learning, but that day is not yet here.
News flash: “That day” passed in March, 2020.
Macaque Me an Offer I Can’t Refuse
The unreal, mythical, fake thing that is called “OAS” remains a hot topic this weekend, thanks to two papers involving “boosting” in animal models. As both were brought up in the comments over at “Original Antigroundhogic Sin,” I will reprint my own replies below:

Of Mice and Hamsters
Study:
“Replicating RNA platform enables rapid response to the SARS-CoV-2 Omicron variant and elicits enhanced protection in naïve hamsters compared to ancestral vaccine” by Hawman, D. et al.11
My remarks:
First, it wouldn't require any new study to demonstrate that vaccination with a homologous antigen -let's use X' - to a previously vaccinated antigen - X - probably won't result in a lot of antibodies against X'. This is the relevance of OAS in terms of vaccination. It's extrapolating this problem to the real world where things fall apart. Immunology has moved beyond antibodies since 1960. We know that injected vaccination can't provide the mucosal immunity that results from real infection in the first place, so the idea that "can't keep updating antibodies against mutations" is a problem supposes that we shouldn't want vaccinated people to go out and get infected in real life and update their mucosal immune response that way. Why not? Don't we want them to have mucosal immunity at some point? The point of OAS is "how can we make endlessly updating vaccines" not "are endlessly updated vaccines necessary, given real-world immune response after 'infection boosting'." There is no evidence that suggests the answer to the second question is yes, so why are we asking the first question to begin with?
Does this study support any extension of the vaccination relevance of OAS into real life? No.
If we look at Figure 2B, where the grey bars are double A.1 vaxxed + Omicron boosted mice and the pink are double HA influenza vaxxed (control) + Omicron boosted mice, there's no "increase" in ELISA-measured binding against Omicron Receptor Binding Domain because A.1 already had higher anti-Omicron-RBD binding than the HA group ends up having.

Then the neutralization assay (C). Discard the bars, the dots are what matter. 2 of 5 HA influenza vaxxed + Omicron boosted don't pass this test either. This suggests the authors didn't calibrate the neutralization assay very well. A more sensitive assay might reveal more neutralizers in the A.1 vaxxed groups. Even so, neutralization assays are not real life.
Onto the hamsters, where there’s 1-dose A.1 vaxxed, 1-dose Omicron vaxxed, and controls. A.1 vaxxed are a bit outperformed by the Omicron vax, but overall still do much "better" than the controls in terms of where the authors are able to find viral antigen or RNA on day 4. Better is in scare quotes because Omicron did not cause lesions or weight loss on any hamsters, it was totally mild (while earlier experiments with "Wuhan-strains" produced lesions) and focused on upper respiratory tract. But the A.1 vaxxed hamsters, again, had only 1 of 6 viral antigen in lung detection vs 5 of 6 in controls and 4 of 6 epitheilial viral antigen vs 2 of 6 omicron vaxxed and 6 of 6 controls. A.1 vaxxed still benefited against Omicron.
Again as I mention in footnote 2, injected vaccines might still be a net negative via "more plausible mechanisms" but it's not clear-cut. If Wuhan-spike-mRNA-transfection had 0 adverse events, then you would have to weigh protection against viremia with "maybe more reinfections over the course of a lifetime" and you might come up with "better for some." If you believe that the immune system is smart and knows what it's doing, you can see why either outcome could be true: The immune system should only encounter the virus in natural context, to not be confused, or the immune system will self-correct after "natural boosting" post injection.

The Grapes of Macaqueth
Edit, March 9: This study’s non-confirmation of OAS has now been far more extensively appraised here:

Elsewhere, in the OAS saga:
“Even-Steven.” (OAS is “proven” via generation of a more balanced immune response against Alpha or Delta after breakthrough infection.)
“Original Antigroundhogic Sin.” (OAS is “proven” via breakthrough blood samples taken too early for seroconversion, and an overhyped UKHSA comment.)
“Funeral for a Fact,” footnote 3. (OAS is “proven” because the boosters restore infection efficacy vs. Delta during the Omicron wave.)
“Darmok and the Spike Protein at Tanagra.” (OAS is “proven” when high pre-existing antibodies against coronaviruses… don’t correlate to severe outcomes in infection with SARS-CoV-2 in any way.)
Archive of the original Gagne, M. et al. comments:
Study:
“mRNA-1273 or mRNA-Omicron boost in vaccinated macaques elicits comparable B cell expansion, neutralizing antibodies and protection against Omicron” by Gagne, M. et al.13
My remarks:
Not to be macabre with the macaques, but the study is way too limited. What’s the biology of mRNA transfection with an Omicron protein vs a Wuhan protein to begin with, not in the context of a booster? Changes to the spike amino acid recipe can affect cellular output in different hosts, based on a million different factors.
And does mRNA + spike production + immune response on macaques really say anything about the outcomes for humans? The authors are in la-la-land when they say macaques have been well established as correlates for protection. Nothing is a correlate for protection for Omicron.
Lastly, only eight test subjects? I look at the pre-boost antibody levels and those eight monkeys are already very skewed in antibody output. So did the high-pre-booster-antibody monkeys fall in the Wuhan booster or the Omicron booster set? If the former, that would throw out the results for which booster “induced” more neutralizing antibodies.

And what would the results be of a non-boosted Omicron challenge? Oops, the study has no non-boosted macaques to work with, sorry. Geez, why couldn’t they just let these poor 8 monkeys go about their lives instead of pretending there was anything left to gain from infecting and sacrificing them without a large enough population to control for anything?

All that aside, in so far as the study suggests anything it’s that prior sensitization to the “wuhan spike” doesn’t impede immune response against Omicron in any meaningful way during actual infection.


That defunct url is here: https://journals.lww.com/greenjournal/Fulltext/9900/Association_Between_Menstrual_Cycle_Length_and.357.aspx
The web archive, again, has the original in snapshot:

The paper’s findings also remain summarized (and downplayed) in the recent editorial by Victoria Male, “Menstruation and covid-19 vaccination.” BMJ 2022; 376:
Most affected were the 358 individuals who received both doses of the vaccine in the same cycle, experiencing a 2.32 day (98.75% CI 1.59 to 3.04) delay to their next period. Among this group, 10.6% experienced a change in cycle length of more than 8 days, which is considered clinically significant, compared with 4.3% in the unvaccinated cohort (P<0.001). In all groups, cycle lengths returned to normal by two cycles after vaccination.
NBC Washington Staff. “School Boards Granted Temporary Ruling Against Virginia Governor's Mask Order.” (2022, February 4.) nbcwashington.com.
Natanson, Hannah. Weiner, Rachel. Jouvenal, Justin. “Judge temporarily halts Youngkin order making masks optional in Va. schools after lawsuit from school boards.” (2022, February 4.) The Washington Post.
(Oh, boo hoo.)
(Do imagine yourself circa-2019 reading this line. Just what is happening in this fictional Future Virginia; is it an invasion of brain-eating alien child-swappers?)
(index link anchor)
(index link anchor)
It's been evident for decades that public school teachers are, by and large, overpaid mediocrities who fail at rates no other profession would allow. What wasn't as clear until Recent Events was how fanatically selfish, money-grubbing and lazy they are, and the very last thing they care about is "the children." The entire system should be abolished. There is no saving it.
The spike proteins from the cmRNA vaccines are coded with Pseudouridine, an isomer of Uridine. These proteins will be isomeric as well, since Uracil is replaced 100% with Pseudouridine. Thus, the antibodies will have a different chirality/configuration than "normal" abs, i.e., they will be isomeric. That is, they have nothing to do with spike proteins from Sars-Cov-2, which are coded with Uracil. The latest experiments point out to this scenario: ICU cases of Covid-19 are caused by two lethal abs, REGN10987 and B38. Since the immune system is sabotaged to create numerous isomeric abs, there will be fewer binding/neutralizing abs, including the two lethal abs mentioned above. But now, the vaccinated people have a huge quantity of isomeric binding abs in their organisms, which are awaiting an activation (since these isomeric abs are misfolded abs, they can also be neurotoxic; they also include the lethal isomeric version of REGN10987 and B38). So, we have two pandemics running in parallel: a Uracil coded Sars-Cov-2, which by now has become Mers-Cov-2 (Omicron uses the DPP4 celullar receptor, same as Mers-Cov, both having a huge R0: Omicron has R0 of 10, while Mers had R0 of between 7 and 19 in South Korea), and a Pseudouridine coded Sars-Cov-2, which is part of the cmRNA vaccines. cmRNA = chemically modified RNA, or modRNA. Had the vaccines been coded with Uracil, full fledged mRNA, all of the vaccinees would have found themselves in ICUs right away, since then a huge number of lethal abs (REGN10987 and B38) would have been fabricated by the immune system. Since there are trillions of spike proteins (coded with Pseudouridine) being produced, obviously there won't be a matching number of isomeric abs: it is now known that such spike proteins remain in the body for up to 15 months, and so do the binding isomeric abs. Spike proteins = T-bacilli of Wilhelm Reich = prions. Dextrorotatory prions = misfolded prions. What could activate the Pseudoridine coded spike proteins (prions) and the isomeric abs to a full dextrorotatory prion state? A thermal shock (volcanic eruptions on an unprecedented scale), or scalar biological weapons being used.
Omicron = Omega (practically same letters). Omicron paves the way for the Pi variant: a Pseudouridine isomeric version of Sars-Cov-2.