
Even-Steven
If you guessed "comments on the OAS portion of Röltgen, K. et al."... you win a candy bar.

Note: This post uses a definition of “imprinting” that does not relate to “specificity” of antibody responses (the definition that turns out to be used in most “imprinting” studies and is now what I use on this site).

A whale of a study, published two weeks ago but highlighted by Robert Malone last night,1 uncovers persistent presence of mRNA and spike protein in the near-injection lymph nodes of mRNA vaccine recipients, physically distributed in a manner that suggests localization within Antigen Presenting Cells and thus recent / ongoing presence of vaccine payload in transfected cells… for up to 60 days after the second dose of either Moderna or Pfizer/BioNTech.
(Note: Those results are explored in “The 60 Day RNA Mystery.”)
The study also provides more evidence for circulating spike in the blood after injection, and tentative evidence that mRNA-injection-generated antibodies effectively camouflage spike generated by the 3rd (booster) dose.2
And, incredibly, the study presents this potentially future-of-half-of-humanity-determining revelation as a mere accompaniment to another self-declared validation of Original Antigenic Sin.
The paper may address both topics together, but I think it makes more sense to review them separately. And the OAS issue naturally deserves to be addressed first, because how can the future of half of humanity be more important than this journal’s private war on a once-obscure, now overhyped immunology trope? Anyway, to abridge the OAS Is Not Real triptych begun by the prior two posts would be aesthetically criminal.
However, before preceding, the reader is encouraged to consider reading the Röltgen, K. et al. study for themselves.3 It is well-designed and well-written (aside from the ramblings regarding OAS), and contains a wealth of comparative antibody kinetics findings which in reality overshadow the OAS headline. In fact I may devote a third post to the paper in the end, just to review the full spectrum of results.
In between OAS’s vintage obscurity and the current rage of attention spurred by the rushed rollout of the Covid vaccines, is several years of recent, bizarre obsession on the part of a distributed population of researchers. The theory, as I’ve taken pains to point out over and over, predates the last six decades of understanding of cellular and innate immunity. For present-day immunologists to obsess over the topic is akin to modern nuclear scientists staying up at night to fill their chalkboards with proofs for phlogiston.
Röltgen, K. et al., for example, seem positively hypnotized by the implications of imprinting as it would play out in an Alternate Reality where antibodies are the be-all-and-end-all of immunity:
As additional variants of SARS-CoV-2 appear over time, individuals will acquire distinct immunological histories depending on which vaccines they received and which viral variants infected them. The idea that “imprinting” by a prior antigen exposure can shape, either positively or negatively, the response to a subsequent variant is well established in studies of influenza viruses, and has been implicated in birth-year differences in susceptibility to particular avian influenza viruses (Gostic et al., 2016). […] While current booster vaccinations are still based on the Wuhan-Hu-1-like antigens, vaccine manufacturers are in the process of evaluating updated vaccines encoding sequences from one or more circulating variants. Initial results from 3rd dose boosting with Beta spike-encoding mRNA vaccines after prior 2-dose mRNA-1273 vaccination are consistent with our findings of significant imprinting of serological responses by the first antigen encountered (Choi et al., 2021; Chu et al., 2021), indicating that vaccine-derived imprinting affects subsequent antibody responses stimulated by vaccination as well as infection. The extent to which vaccine boosting or infection with different variants will effectively elicit antibody responses to new epitopes, or rather increase responses to the epitopes of antigens encountered previously, as in the “original antigenic sin” phenomenon described for influenza virus infection and vaccination (Arevalo et al., 2020; Zhang et al., 2019), will be an important topic of ongoing study. The degree of imprinting may depend on the particular variants and the order in which they are introduced to the individual’s immune system, and the number of exposures, such as the number of vaccine doses received.
Again, imprinting is real, but antibodies are only the tip of the iceberg that is the immune system to begin with. It boggles the mind that immunologists in the present day can fall into the trap of imagining that successful immune protection depends on their solving of the obsolete, endless contradictions implied by a 1960s-era understanding of biology. To deconstruct:
Q: Why does the immune system need antibody responses to new epitopes, post viral challenge?
Answer: Because otherwise there won’t be antibodies to the new epitopes!
Q: …So? Isn’t the virus just going to change again anyway? Isn’t this, presumably, why the immune system does not exclusively “store” the memory of viruses in antibodies? Why there’s T Cells, innate immune reprogramming, and who knows what else? What does generation of novel epitopes say about performance against future epitopes, especially with relation to the entirety of memory immune response?
Answer: But… but there aren’t antibodies to the new epitopes! Weren’t you listening!?
And, again, the “conundrum” of imprinting has an obvious relevance under the paradigm of influenza vaccination, or any hypothetical “Software Update” vaccination program: If the goal is for antibodies to new epitopes to predate encounter with those epitopes, which can only be accomplished by artificial intervention, then the desired ability to artificially stimulate production of homologous antibodies is indeed thwarted by “imprinting.” Eliciting bespoke antibodies with injected antigens is a one-time trick.
In nature, predating encounter of novel viral epitopes with production of antibodies is an obvious impossibility. So, obviously, the immune system has learned how to get by without doing so. There is no crisis here.
And yet OAS farcically presumes that the whole “imprinting” situation is some existential disfunction in urgent need of medical remedy. At least we can forgive the theory itself for being a product of the times; the modern researchers obsessed with OAS have no such excuse. And meanwhile the modern peddlers of Leaky Vaccine Disaster theories continue to farcically assure their audience that the researchers are finding evidence for this imaginary crisis all over the place.
The sentence that was excerpted from the wall of text above summarizes the entirety of the “evidence” that this paper contributes to the imaginary crisis of OAS:
We find that prior vaccination with Wuhan-Hu-1-like antigens followed by infection with Alpha or Delta variants gives rise to plasma antibody responses with apparent Wuhan-Hu-1-specific imprinting manifesting as relatively decreased responses to the variant virus epitopes, compared to unvaccinated patients infected with those variant viruses.
But to be fair, I should also report a quote from earlier in the paper, although it is redundant, as it provides even better fodder for the substack bloggers who will soon be reporting this new “smoking gun.” It’s the real “highlight-screenshot-bait” of the pdf:
To test whether prior exposure to one SARS-CoV-2 RBD variant causes imprinting of humoral immunity, we analyzed plasma from individuals vaccinated with Wuhan-Hu-1-like antigens and subsequently infected with Alpha or Delta variants (Figure 5A, lower panels). Despite breakthrough infection with Alpha or Delta viral variants, the vaccinated individuals showed patterns of IgG binding to viral variant RBDs similar to those of individuals exposed to only Wuhan-Hu-1.
See, they “tested” something! And “the vaccinated individuals showed patterns!” Testing! Patterns! A-ha! What more proof for OAS do you need!?
So, before revealing Figure 5, let’s set our expectations. The most surefire tactic when presenting the “all over the place evidence” for OAS is to never set these expectations beforehand. We will not be participating in that error.
The authors are going to report binding against the Alpha and Delta Receptor Binding Domain as a ratio of binding against the vaccine-scripted Wuhan spike RBD. They are not going to show us whether the vaccinated-plus-infected underperformed the naive-infected in raw binding performance.
Biologically, what should we see?
The Covid-vaccinated have circulating B Cells that will be stimulated by the spike protein of the virus that is “breakthrough”-infecting them. These B Cells are going to multiply and mature, and kick out untold hordes of the same antibodies they were previously enriched for by the mRNA-transfection. This is prior memory replaying itself.
Novel immune memory will not involve or depend on these B Cells. Instead, Antigen Presenting Cells will break up the new Alpha- or Delta-spike protein and orchestrate the enrichment of a new B Cell lineage.4 After infection is cleared, collected plasma will presumably include both antibodies with high affinity for the (vaccine-mimicked) Wuhan spike protein and for the Alpha- or Delta-spike.
The non-Covid-vaccinated have no previously circulating B Cells for the Wuhan spike.
After infection is cleared, collected plasma will include antibodies with high affinity for the Alpha- or Delta-spike, but not for the Wuhan spike.
So the Covid-vaccinated group should be pretty even (the ratio of binding to Delta and Alpha spike vs Wuhan will be near 1); the second group should be lopsided. Biology therefor refutes the implied “test” that the authors have designed. The extent of “imprinting” on the vaccinated+infected cannot be revealed by comparison of the variant/Wuhan binding ratio with a donor set that has no high affinity antibodies for Wuhan. As an analogy, imagine measuring how ability to play Super Mario impedes ability to play basketball by showing “ratio of basketball skill to Super Mario skill” side by side for people who can do both vs people who have never played Super Mario. The skewed basketball-vs-Super Mario ratio of the “naive basketball infected” wouldn’t have any quantitative relevance, and finding out that Super Mario players are better at the video game than they are at basketball would not tell you if the Super Mario players are better or worse at basketball than the naive cohort.5
And with that, on to Figure 5. It turns out, “pretty even” in the Covid-vaccinated and skewed in the naive infected is exactly what we see:
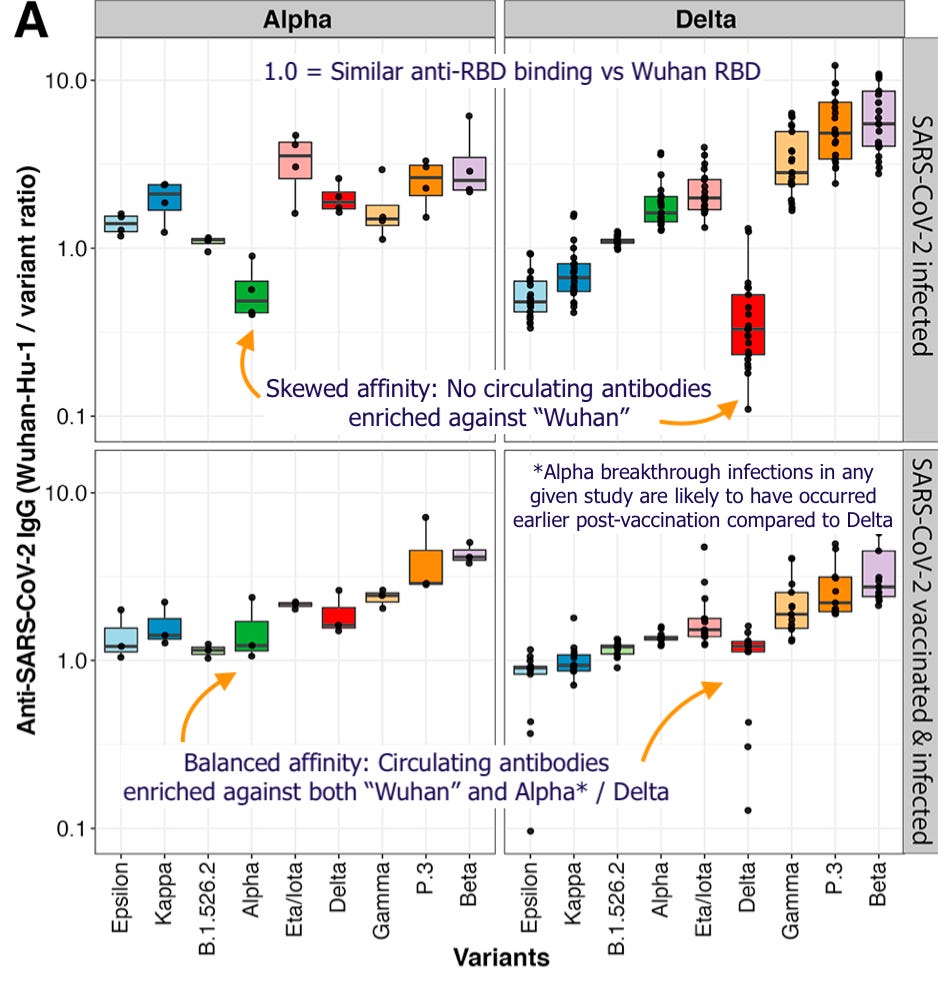
As with any “breakthrough” antibody kinetics study, pre-Delta (as in Alpha) infections are likely to have occurred earlier after Covid-vaccination, before vaccine-induced antibodies had dropped as much as they went onto do worldwide over the summer. These infections would on balance be milder, if not asymptomatic, and thus less likely to stimulate a high anti-Alpha response.
What’s more, the Delta-specificity of the Delta breakthrough response, compared to Alpha breakthroughs, is a robust demonstration that the immune system has created a tailored, novel immune response to the variant encountered, despite alleged “imprinting.” If all that were happening were the execution of the “imprinted” script, there would be no difference in Delta affinity between the two sets of breakthrough-infected. The influence of “imprinting” on breakthrough response is thus limited to an extent that is essentially impossible to quantify (absent raw binding results), but might as well be absolute.
An honest test of OAS would attempt to demonstrate that post-breakthrough plasma essentially doesn’t gain any affinity against the new variant at all - by comparing to samples from before breakthrough infection, rather than an irrelevant head-to-head with the naive infected.
All that these authors have found is that breakthrough leads to a pretty balanced, but still Wuhan-skewed anti-RBD affinity response; along with the obvious but unspoken side-result that 25% of breakthrough infections resulted in a strongly Delta-corrected response:

And perhaps comparison with the pre-breakthrough response, broadly favorable as it is, is where a more clever Leaky Vaccine Disaster proponent could attempt to rescue the results. As we will see below, the Covid vaccines seemingly induce high cross-affinity against the RBD of other variants in advance of infection. This drives down the baseline “Wuhan preference” for the Covid-vaccinated; the correcting effect reported above would obviously be more impressive if the Covid-vaccinated were 50% or higher skewed toward the Wuhan strain to begin with.
Röltgen, K. et al. are thus able to claim that their evidence of imprinting is somehow hiding in the “pattern” of the post-breakthrough RBD affinities.6
Despite breakthrough infection with Alpha or Delta viral variants, the vaccinated individuals showed patterns of IgG binding to viral variant RBDs similar to those of individuals exposed to only Wuhan-Hu-1.
Yes, “similar.” But also “different” - breakthrough infection induced a clearly observable change in “relative” affinities against Alpha and particularly Delta (it really would have been helpful if the authors had reported the raw values here).
7Reference to these patterns is required because the authors did not have available pre-infection samples for the breakthrough-infected. But as the reader can see, day 210 sera of their primary set of Covid-vaccinated subjects already has a close-to-balanced affinity for Alpha and Delta to begin with:

Raw binding results further demonstrate that the recently-Pfizer-injected have much higher cross-RBD affinity than the infected, or recipients of alternate brands:

The authors, notably, are at a bit of a loss to explain the magically enhanced cross-affinity elicited by the injections vs infection. (In fact, it’s partially in attempt to do so that they embark on the lymph node biopsies that lead to the more explosive findings.)
Meanwhile, we could speculate that the effect is a result of the injections’ forcing the immune system to focus on the spike protein exclusively, which results in higher average affinity for the receptor binding domain vs. infected patients, combined with potentially high variability in the translation of the Pfizer mRNA. In other words, the Pfizer-vaccinated are showing their immune system more spike, and more mutant “variants” of spike, than were encountered in Wuhan-era natural infections.
But it is the finding I just hinted at which sinks the author’s own conclusions regarding “imprinting.” Pfizer-vaccination not only induces enhanced cross-affinity for variant receptor binding domains, but higher RBD-affinity than non-severe natural infection to begin with:8
Stanford BNT162b2 vaccinee RBD and spike IgG concentrations were comparable to those of severely ill patients, and higher than those of mildly or moderately ill patients for anti- RBD antibodies at day 42.
As quoted earlier, the comparison being made in Figure 5 is in binding to the receptor binding domain, specifically, of the Wuhan and variant spikes. The naive infected obviously have no pre-existing antibodies with high affinity for the Wuhan spike, and so their affinity ratios do not elucidate anything. But for the vaccinated+infected, absent a severe course, novel anti-Alpha or anti-Delta antibodies are unlikely to have as high affinity for their respective RBDs as the vaccine-induced antibodies have against the Wuhan RBD.
The residual skew toward higher binding against the Wuhan RBD is thus not an artifact of “imprinting,” but of the aberrantly high RBD-affinity induced by injection vs. infection.
In other words, the Covid-vaccinated were probably just unnaturally good at Super Mario, not bad at basketball.9
Previously, in the OAS saga:
“Macaque Me an Offer I Can’t Refuse.” (OAS is “proven” via animal models where mRNA-vaccinated hamsters and macaques do better than unvaccinated controls vs Omicron.)
“Original Antigroundhogic Sin.” (OAS is “proven” via breakthrough blood samples taken too early for seroconversion, and an overhyped UKHSA comment.)
“Funeral for a Fact,” footnote 3. (OAS is “proven” because the boosters restore infection efficacy vs. Delta during the Omicron wave.)
“Darmok and the Spike Protein at Tanagra.” (OAS is “proven” when high pre-existing antibodies against coronaviruses… don’t correlate to severe outcomes in infection with SARS-CoV-2 in any way.)

See https://gettr.com/post/pt7fjg88a6
and Malone, Robert. “A Health Public Policy Nightmare.” (2022, February 8.) Who Is Robert Malone.
and Röltgen, K. et al. “Immune imprinting, breadth of variant recognition and germinal center response in human SARS-CoV-2 infection and vaccination.” Cell.
This may imply that spike-induced toxicity is reduced for doses that follow the first course - though spike-antibody complexes may still have unknown interactions with vasculature and other tissues; the antibodies themselves may have autoimmune harms; and the direct pathologies resulting from mRNA transfection may still be exacerbated by repeat dosing. Such as my theoretical cancer etiology. See “Liquid Cancer.” But I suppose I will be mentioning all of this again when I review the primary results.
See footnote 1, which also links to Malone’s review of the findings regarding the residual mRNA and spike protein detection.
For an overview of the symphony of events that is memory B Cell generation, see Akkaya, M. et al. “B cell memory: building two walls of protection against pathogens.” Nature Reviews Immunology volume 20, pages 229–238 (2020).
I initially wrote in this footnote that this “inversion” is visible in Figure 4 of the paper, which compares the non-infected Covid-vaccinated against the infected. Actually, Figure 4 does not contain the inversion. The Pfizer/BioNTech vaccine antibodies outperform natural infection antibodies against all variant RBDs (A), and also score “lower” in the “Wuhan RBD skew” view (B) - but this result implies positive variant affinity vs. post-infection in both views. I really dropped the ball on that one:

Note that the Mongolian samples were taken in a range of timepoints up-to the cutoffs, potentially explaining the lower affinity vs the Stanford values which were collected at Month 1 and 3 precisely. The authors supply this plausible speculation themselves; they are quite capable of thinking of non-OAS explanations for disparate immune responses when it occurs to them to try.
As far as I can tell, this incriminating pattern is meant to be visually demonstrated in Figure S5 A and mathematically demonstrated in Figure S5 B, via magic principal component analysis. However, the text does not make it completely clear whether “Vaccinee, CoV2+” represents breakthrough infections or individuals injected after infection (as in other figures). Make of it what you will:

(index link anchor)
It is with a bit of hesitation that I recycle the authors’ phrasing here. Rather than severe infections “generating more / higher-affinity antibodies,” it is more accurate to say that non-severe infections more frequently result in lower levels of antibodies. But non-severe infections still result in high antibodies the rest of the time.
This is even the result in Röltgen’s previous antibody kinetics study for natural infection with the “Wuhan” era virus (these measurements are the ones reused in the new study) - Röltgen, K. et al. (2020.) “Defining the features and duration of antibody responses to SARS-CoV-2 infection associated with disease severity and outcome.” Sci. Immunol.
However, since few outpatient subjects are included, the “high dots” in their group appear rare, even in Weeks 4 and onward after more seroconversion and enrichment against RBD has taken place:

In real life, non-severe infections would not be rare. Most infections are not severe, so even if only “one-fourth” of non-severe infections resulted in high antibody levels, most high-antibody-generators will be non-severe recovered.
There are thus limits to using antibody levels as a proxy for severity; as when Lin, C. et al. extrapolate from antibody generation to severe-outcomes even though actual infection outcomes were not more severe (see “Darmok.”)
Still, since the Covid-vaccinated subjects in this new study had very consistently high binding against the RBD, more incidences of lower binding should be expected in the context of natural infection, including for variant-tailored antibodies after “breakthrough” infection.
The authors’ admission that their Covid-vaccinated subjects had consistently higher binding than non-severe infected in fact implies that their exclusive use of “ratio view” in Figure 5 would deflate apparent binding post-breakthrough, compared to raw binding values. Of course, one cannot be sure if the same observations would hold up among the naive Alpha and Delta infected, given that the variants may have been more prone to severe infection than the Wuhan-era virus. Even so, this renders the absence of raw binding values in Figure 5 extra conspicuous.
Are the authors hiding that the breakthrough-infected had measurably better anti-Alpha and anti-Delta RBD binding than the naive Alpha- and Delta-infected, because that would contradict their headline conclusion, and once again directly refute OAS?
Hi Brian,
Spotted this as a question/answer in Rintrah's comments page yesterday:
'How about if you got vaccinated, and then get infected? Is the vaccine an obstacle to your immune response?
In that case you get to deal with original antigenic sin. Specifically it seems your body will struggle to develop an antibody response against the Nucleocapsid protein.'
There's been quite a lot about this inability of the vaccinated since the 'data' from a look at UK blood donors. Is there a struggle to deal with the nucleocapsid in the vaccinated and even if there is, how permanent and how important might it be do you think?
Hi, Brian!
I must confess that some of the points you made in this article baffled me on first read.
I understand that you don't think that any good evidence for OAS has been mounted, and I get that our immune systems are far more more complex and adaptive than OAS theorists would have us believe.
However, I am having trouble integrating your analysis into the bigger picture.
I was wondering if you would be so kind as to answer some very basic questions.
On a personal level, who do you think, if anyone, would be well served by getting Pfizer and Moderna mRNA vaccines?
If someone were to be forced to get one of the currently US approved vaccines for the first time, which one would you currently recommend?
Who do you think, if anyone, would be well served by getting Pfizer and Moderna mRNA boosters?
On a population level, what populations, if any, would you have recommended these mRNA vaccines to? Has the emergence Delta and then Omicron changed your analysis? If so, how?
What is your analysis of the trajectory of Marek's disease in chickens? How likely do you think mass vaccination with leaky vaccines during a pandemic could result in such a disaster among humans?
I realize that I may be asking you to bite off more than you would like to chew, but I truly value your perspective and would love any answers you could give me no matter how few or short.