
Glass House
A New York IVF study finds higher rates of pregnancy failure among Covid-vaccinated women.


It’s right there in the picture:1

In a comparison between 214 Covid-vaccinated patients and 733 unvaccinated controls, from February to September of 2021, the Covid-vaccinated had a lower rate of achieving clinical or ongoing pregnancies during frozen embryo transfer IVF. Rates of loss before (“Biochemical”) and after determination of clinical pregnancy were higher.
And yet what do the authors make of their own results? “Nothing to see here”:
The primary outcome of clinical pregnancy rate in the frozen-thawed embryo transfer cohort was similar between the vaccinated and unvaccinated groups (59.5% […] vs 63.7% […]). No significant differences were seen between vaccinated and unvaccinated patients in the secondary outcomes of pregnancy rate, ongoing pregnancy rate, biochemical loss rate, or clinical pregnancy loss rate (Table 2, Fig. 2).
The clinical pregnancy loss rate, in relative terms (and among confirmed clinical pregnancies only), is 50% higher. Is that not a significant difference?
What of the primary outcome? Isn’t the whole reason we have numbers so that we can tell when amounts are different? If I have $63.70, spend $4.20, and observe that only $59.50 remains, am I to think, What’s going on here? Why didn’t the amount of money in my wallet get any lower?
59.5 is less than 63.7!
The study compared outcomes from two different starting points. The first was Controlled Ovarian Hyperstimulation. Here, a small advantage was found in the “performance” of the Covid-vaccinated - but the endpoints are focused on egg collection, and do not include attempted pregnancies.
The second starting point was Frozen Embryo Transfers, in which the clinic attempts to establish pregnancy using previously collected and cryogenically preserved eggs. The advantage of comparing outcomes for this process - and excluding fresh transfers - is that with egg collection already complete, patient procedures for endometrial preparation are easily standardized and observed, all managed according to a set schedule.2 This, the authors feel, creates a more scientific backdrop for comparing the effect of an outside intervention (as in, Covid-vaccination) on success rates.
And yet, despite this sort-of controlled setting, the authors dismiss their own findings of an effect of the outside intervention. Lowered performance is observed not just in the primary outcome (clinical pregnancies), but every secondary outcome as well: All pregnancies, ongoing pregnancies, biochemical loss, and clinical loss (all terms referring to different stages of confirmed pregnancy):

From the authors’ own results, it is evident that the Covid vaccinated seem to “lose” via attrition: Serum hCG elevation rates (“pregnancy”) are (truly) nearly equal at the start. Patients are scheduled for transvaginal ultrasonography one week after hCG rise; this is the when “clinical pregnancy” is confirmed by the visualization of the intrauterine gestational sac. By this point, the Covid-vaccinated are already experiencing an apparent higher “failure” rate.
Weekly monitoring continues until discharge at week 8 or 9, with discharged patients contributing to the “ongoing pregnancy rate.” Once again, the Covid-vaccinated have a higher dropout rate before meeting this benchmark.
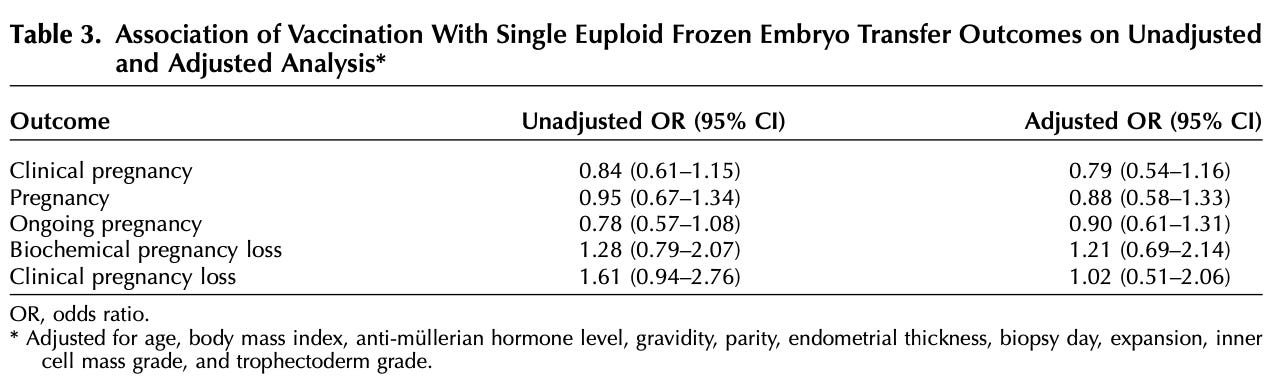
The authors attempt at length to “adjust” away their own findings, even though the unvaccinated cohort was already matched with the Covid-vaccinated cohort by age (the most important factor for determining IVF outcomes), BMI, anti-müllerian hormone, gravidity (prior pregnancies), parity (prior births of 24 weeks or later), and endometrial thickness:

The results obtained by “adjusting” these already well-matched cohorts are seemingly absurd, with some adjustments disfavoring the Covid-vaccinated, but the glaringly high odds ratio for Clinical Loss conveniently erased-away:
All that is seemingly achieved here is sowing confusion. The cohorts are broadly similar; the differences in raw rates, again, speak for themselves. Note that the historic Clinical Pregnancy rate at this facility is given as none other than 64% - almost exactly the rate observed for the unvaccinated during the study period (emphasis added):
For our primary outcome of clinical pregnancy rates among frozen- thawed embryo transfer cycles, a sample size of 171 single euploid frozen-thawed embryo transfers per group was required to detect an absolute difference of 15% in clinical pregnancy rates with 80% power and alpha of 0.05, based on 64% clinical pregnancy rates in our center.
So for the authors to dismiss an anomalously lower result - 59.5% - among the Covid-vaccinated is extra conspicuous. Once again, the authors designed their study around frozen embryo transfer to make head-to-head comparison of the Covid-vaccinated and the unvaccinated easier.
Yet perhaps the authors deemed the difference in outcomes not to meet their own statistical benchmarks. As above, per their calculations, 171 Frozen Embryo Transfer cycles would have been enough to “detect” a 15% change in a statistically satisfactory manner. Does this mean it was not enough to “detect” a smaller change? So what? They followed 214 cycles among Covid-vaccinated patients, and found a 4.2% change. Outcomes were even more stark when comparing “ongoing” pregnancies - those which were eventually referred to an obstetrician for follow-through - with a relative 11% fewer such outcomes ((53.6-47.5)/53.6) among the Covid-vaccinated. (Birth outcomes are not reported, as few pregnancies came to term during the observational window.)
Whether these results hold up to statistical benchmarks is not relevant. The authors set out to investigate potential negative impacts on fertility from Covid-vaccination; these results are a signal for a potential negative impacts on fertility. Perhaps the results were a fluke; perhaps an even broader study would reveal, thankfully, no negative impact on IVF fertility after Covid vaccination; but for now the correct interpretation is to cautiously sound the alarm, not throw water on any attempt for patients to think for themselves before potentially risking their ability to have children!
Patients vaccinated with the Pfizer or Moderna COVID-19 vaccine had similar responses to ovarian stimulation and similar pregnancy outcomes compared with unvaccinated patients. These findings provide reassurance that reproductive potential does not appear to be affected by COVID-19 mRNA vaccination in patients who undergo IVF.
Our data contribute to the ever-increasing evidence that COVID-19 vaccines do not negatively affect fertility or pregnancy.
There is no basis for this sanguine text. These results do not contribute support to the safety of these experimental gene products for women seeking to conceive; in fact, they constitute evidence in the other direction!
But there is nothing to really say about it, in the end. The authors have written what they have written. In throwing the stone at their own results, it is their own glass-house they have brought down. What IVF patient wants to hear that a 11% relative reduction in successful ongoing pregnancies looks like “no effect” to their reproductive potential, or constitutes a “similar” outcome?
If the authors are this careless, this indifferent, with their own patients’ pregnancies, they’ve done those patients a favor by putting this confession on paper.

Related: “Pharmaccounting” (Pregnancy outcomes after infection vs Covid-vaccination in Scotland)
Aharon, D. et al. “In Vitro Fertilization and Early Pregnancy Outcomes After Coronavirus Disease 2019 (COVID-19) Vaccination.” Obstetrics & Gynecology: January 25, 2022.
edit, February 7:
And now the paper is back online, with no apparent edits.
edit, February 4:
The paper has been removed from the lww.com site. The web archive snapshot is preserved at http://web.archive.org/web/20220126135121/https://journals.lww.com/greenjournal/Fulltext/9900/In_Vitro_Fertilization_and_Early_Pregnancy.378.aspx
The abstract is still online at https://pubmed.ncbi.nlm.nih.gov/35080199/, but only reports the adjusted OR figures for frozen embryo transfer.
(Aharon, D. et al.)
By evaluating only euploid frozen-thawed embryo transfers, our study excludes a number of confounding variables that may affect pregnancy and pregnancy loss rates. Our control group cycled during the same time period, using the same protocols and techniques. Both the study and control groups were subject to the same environmental exposures, including exposure to SARS-CoV-2 in the community. The inclusion of only the first cycle for each patient served to minimize potential bias from repeated frozen-thawed embryo transfer cycles, which would necessarily be due to failed transfer cycles during this short timeframe, and to remove partial crossover between the groups.
They have vanished the article.
As this continues more people are going to consider science to be little more than witchcraft and tea-leaf readings with lab coats thrown in. Writing that your own results aren't what they are showing themselves to be should disqualify anyone from even playing with a children's chemistry set.
And yes, hope you are feeling better as others have said.