


The Vulgarity of Normal
Will logic and rhetoric end normalized mass child abuse, or is it far too late for that?



Vinay Prasad is confident that the “tide is turning.” Look at all the headlines (two of which are his own; two of which are the same screenshot, but resized and repositioned)! It certainly seems like some top-down effort to reverse the groupthink on forcing children to wear symbolic muzzles for hours on end to appease an angry Virus-God is underway.
Until you look closer.
Over in the Endless Ethical Posturing Olympics arena complex that is epidemiology / medical twitter, a pathetically low bar of common sense regarding “children and Covid” was only recently offered for credentialed fear-mongerers to competitively vault over; they obliged. MedPage Today, as always, provided the post-competition highlights:1

"We believe the data point to restoring full normalcy for children," said Balsitis, who confirmed the group feels this should happen by February 15. "We really mean the full normal."
Nearly 400 medical professionals have already co-signed in support of what the group calls its advocacy toolkit via its website, but their recommendations have also been met with swift criticism from peers.
"Proselytizing for a predetermined conclusion under the guise of objective, evidence-based analysis is not junk science, it's just junk," tweeted Mark Kline, MD, of Children's Hospital New Orleans, in response to the group. "With the health, well-being and lives of children at stake, we have every right to expect much more of our physicians." […]
Lakshmi Ganapathi, MBBS, a pediatric infectious disease physician at Boston Children's Hospital and Harvard Medical School, concurred, pointing out that many policy proposals are being shaped by opinions of the privileged.
"They really silence the realities of communities of color," she said. […]
A Twitter thread by Tyler Black, MD, a child and adolescent psychiatrist and suicidologist in Vancouver, noted that a line in the toolkit "about 'deaths from child suicide vastly outnumbering deaths from COVID and are increasing' is about as awful as it gets. I consider it ghoulish to wield child suicide statistics inaccurately to make advocacy points."
Rational dissent, meet histrionic, incoherent, echo-chambered meltdown.
Is the Urgency of Normal toolkit “proselytizing for a predetermined conclusion”? Perhaps, but how would such a subjective charge be litigated? What is the evidence that supports Kline’s assertion regarding the state of mind of the toolkit’s authors, many of whom are from the same background as himself (practicing pediatric medicine)?
To summarize the report, figures on the low hospitalization rates of children and Covid-vaccinated adults are presented; figures on child mental health trends are presented; a call is made to stop inflicting the latter (widespread) harms in the vain effort to mitigate the (rare) former. The report is intended as a resource for parents and communities who want to advocate for the end of the psychological torture of children. So just what does it mean to call this document “pre-determined,” as Kline asserts? Does Kline object to the toolkit’s intended dispersion of knowledge to non-academics, who he feels can’t conduct a true “evidence-based” analysis for themselves? Or to the report’s inclusion of pro-Covid-vaccine-efficacy statistics from the UK? Or to their mention of the Surgeon General’s “mental health advisory” (a report which itself eschews from condemning adults for the listed harms inflicted on children by lockdowns). What else should the authors have done?
Or does Kline mean, merely, that the toolkit was “pre-determined” because it set out to portray reality, and reality is favorable to the argument that Virus Mitigation is harmful to children?
In the MedPage Today follow-up interview, Kline “elaborates” his comments, asserting: “[Urgency of Normal is] not an evidence-based discussion of the pros and cons." But, it literally is that. The only “problem” we might imagine Kline to have with this approach, is that there is no evidence for the “pros” of insulating children from a might-as-well-be imaginary risk. Kline can thus only supply his own “pre-determined” maxims in counter-argument - as if there is some intuitive, socially-universal rationale that supports his mentally deranged notions of wrapping 10,000 children in metaphorical cellophane around-the-clock, until they are old enough to smoke or go to war, so that one “preventable” tragedy will be avoided:
"I think if we were to do as they are proposing, which is to basically do away with mitigation measures where the schools are concerned, and basically throw in the towel and just focus our efforts on a subset of children that are high risk ... that it's bound to lead to more cases of COVID ... more hospitalizations among children, and probably more deaths," Kline noted.
Ok. So what?
What does “more cases” or “more deaths” have to do with how adults should think about the risk to children? The answer, of course, is nothing. Kline’s unspoken argument is that thinking about this risk (or any risk, presumably) is, itself, an act of Child Murder. The “crime” of the Urgency of Normal is that it advocates thinking about the risk.
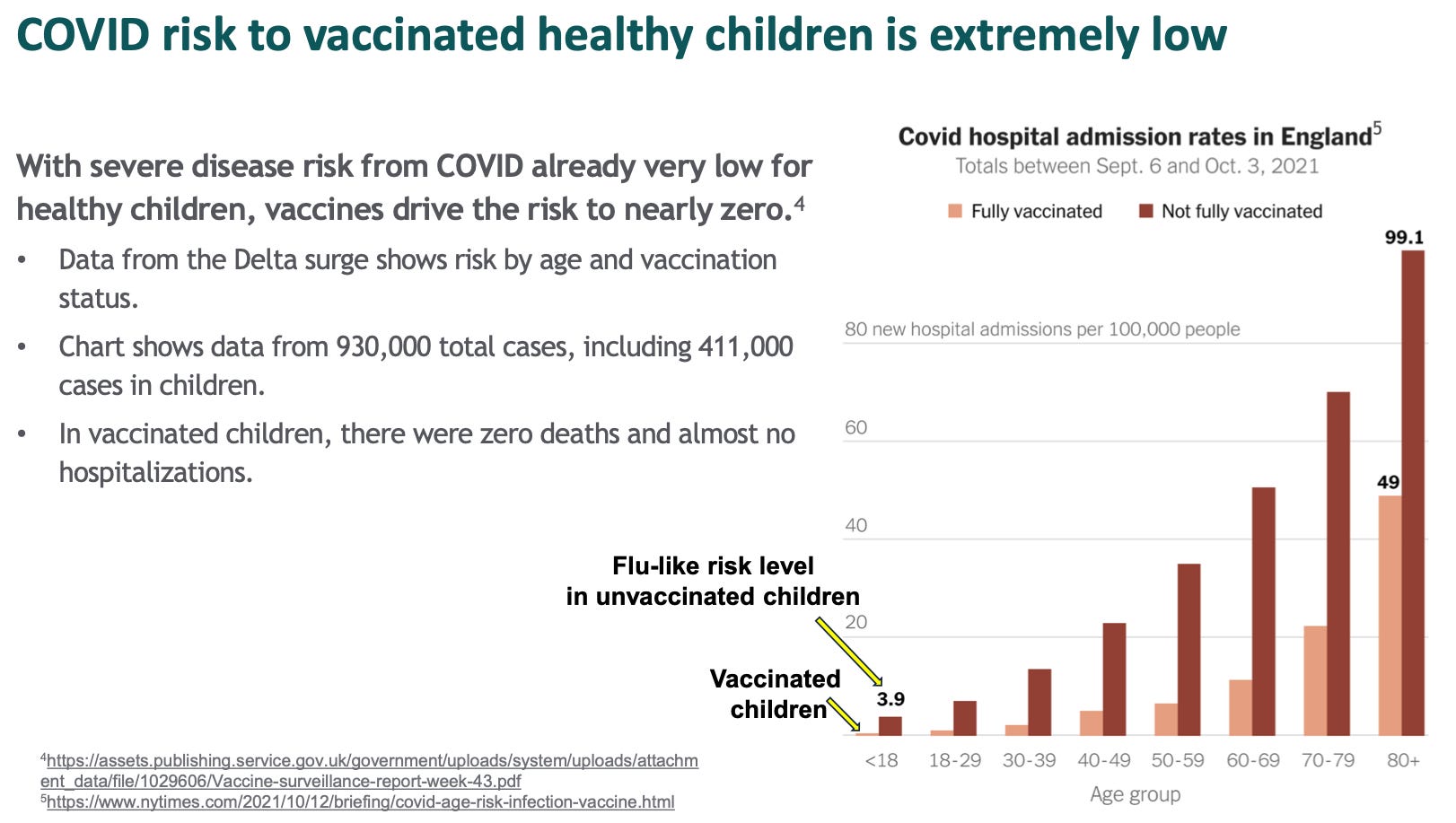
Painting the crime onto this act of rational assessment requires, of course, pure distortion on Kline’s part. Above, the toolkit clearly contextualizes the risk: It is “flu-like” in unvaccinated children; and null in Covid-vaccinated children (almost certainly due to short-term elimination of false-positive “with Covid” hospitalizations2). But in Kline’s hallucinogenic imagining, uncritically reported by MedPage Today (emphasis added):
Kline disputes the idea that there is no risk to children and that mitigation measures are all risk and no benefit, as suggested in the toolkit, in part because he's seen many children who have been hospitalized with COVID-19 in his own hospital.
Kline “disputes” a claim that Urgency of Normal never makes. The report does not claim “no risk,” but only “extremely low” risk.
But since Kline cannot actually dispute that the risk is extremely low, he must portray anything other than the outright catastrophization of “extremely low” as an unthinkable moral transgression. After all, he’s seen “many children […] in his own hospital.”
Well, of course he has. If you put all of some rare thing in one place, and then spend all your time in that place looking at the rare thing, you will see “many” of it. That doesn’t mean it’s not rare.
So it goes with Lakshmi Ganapathi, who asserts that Urgency of Normal “silences the realities of communities of color.” In the first place, no it doesn’t:

In the second place, Ganapathi leaves undefined what it would even mean for this allegation to be true. If the toolkit “silences” community-of-color-realities, does that mean that the “privileged” audience Ganapathi asserts the toolkit is tailored towards should stop using it? On the grounds that, what, it applies to them too much?
Obviously, if Urgency of Normal is unbalanced in treatment, Ganapathi is free to fashion her own toolkits for corresponding “silenced” realities. How she should accomplish this without violating taboos against victim-blaming parents for the obesity of their children would likely constitute an interesting feat of mental gymnastics in its own right. Presumably, at all events, the outcome of her toolkits would be to prescribe that “under-privileged” children wear masks all day and face endless restrictions on their social interaction (otherwise, why would she be complaining about Urgency of Normal’s supposedly white-centric conclusions?).
Great; write your “children of communities of color” toolkit, Ganapathi, advocating for physically muzzling and segregating such children on the basis of their corresponding “realities.” Perhaps you could name your document Separate, but Equal. “Silenced” communities could then decide for themselves which set of policies they prefer for their children.
Ganapathi, of course, would no doubt dismiss this interpretation of her insinuated critique of Urgency of Normal. For in the breath that follows her vaguely implying that the toolkit fails to take diversity of community into account, she faults it for advocating tailored risk management for specifically vulnerable children. This strategy of assigning extra precautions only where they might be needed, she describes as “placing the burden”:
Ganapathi further took issue with the group's recommendations placing the burden of protection on the vulnerable. "We do need to act collectively," she said. "That's a core public health principle."
Well, sure - in so far as “public health” is simply the philosophy that individual human biology resides in the sphere of implicit state interest, with no room left over for personal autonomy, “collective” action (as in restriction) is the only possibility. But in exactly what way are “Children of Nonvulnerable Privilege,” in Ganapathi’s imagining, supposed to help bear the “burden” vulnerable children face as a result of, sorry, their own lack of biological competence?
As the toolkit points out, perhaps a bit fancifully: “High-quality one-way masking is more effective at protecting the vulnerable than universal use of low-quality masks.” High-quality one-way masking isn’t really a practical solution for vulnerable children, either; but the larger point that universal masking of children makes no difference is well-supported by the review of the evidence in the toolkit’s “appendix.” It would arguably be more salient to assert that vulnerable children cannot opt-out of the human race; and neither can the human race opt out of its own biological shared fate. All children will be exposed to common respiratory pathogens eventually; attempting to perpetually “lock down” the lungs of children from the atmosphere itself is a demented, pseudo-scientific fantasy.
But again, the realities of what is possible do not matter; the moral “crime” is not that the report has made an incorrect assessment of the risks facing children - but that it has dared to make the assessment at all, thereby violating the groupthink’s ethical imperative that adults must not base decisions about childhood risk on reality. After all, to do so would result in acknowledging that not all children are the same: Itself an ethically impermissible thought.
Back to Prasad’s tangentially related video-post: He might be right that the pivot in groupthink - and a regression to the “old normal,” circa 2019 - is around the corner. I certainly would like to see such a thing. But if it does happen, it won’t be because the pillars sustaining the religion of mitigation have been weathered by changes to reality, or logical pleas from suddenly enlightened experts and opinion-writers.
In fact it is possible that the foundational mass hallucination of The Pandemic™ - that of a universally dangerous virus - cannot be dispelled by top-down reversals in expert messaging. If it could, after all, would the progressive corner of the Supreme Court still be ranting on record about how “750 million new cases yesterday, or close to that, is, uh, a lot;” would Whoopi Goldberg still react to an anodyne Bill Maher routine - which declared that continued performative Virus Fear is “bananas” - by wincing at the camera with visible strain to excrete the words, “That’s not really funny to people who have lost their kids to this vaccine3, or people who have lost family members, or dear friends.”
Goldberg’s feverish, scandalized revulsion persists despite over a month of concerted attempts by top American TV-experts to pivot from religion to realism; to set the dangers of the virus in context. Perhaps this effort is futile. Groupthink is by definition autonomous; it cannot be authored.4 And as much as Fauci and other talking heads have been given free reign to sermonize the public for the last two years, it never really mattered what they were saying.
The only real “message” was communicated via video footage of hospital corridors: Death is out there. And the task of making the message “real” was always undertaken by the audience: We, the consumers of the message, ourselves. It was a spasm of performative, irrational fear; a hard-core germaphobic mental illness made visible and contagious by the very thing still being debated today: The Mask.
And whatever Fauci’s role in the creation of the virus, however-much the mass hysteria played into his pre-existing plans for a “universal flu vaccine,” his elevation to High Priest of the Apocalypse was a function of his telling the camera whatever was compatible with the hallucination to begin with. In the same way that the TV News serves up an endless string of trial-of-the-centuries for the public to debate over, rendering the private into the societal, the Experts of the Virus are mere bit players in a story that is itself an emergent, collaborative art-project between the media and American culture at large.
So if the “reality” of the mass death hallucination was never actually the manifestation of the solemn reading of inflated “with, not from” figures - though those figures were easy talismans for missionaries of the religion to wield at nonbelievers - then of course a ninth-inning “official retraction” of that manipulative illusion is hopeless. Retract all you want, experts; the addled mind of the hallucinator is capable of filling in any blank. 750 million Americans were infected yesterday alone! For the media to turn the camera on the expert who now says “Death is not as out there as we said it was,” is merely to reinforce the central message once again: Death is still out there. That message only stops if the camera abandons the topic altogether; and that only occurs if the audience stops tuning in to see the message.
Meanwhile, any changes to the reality of the virus or its host that further divorce the hallucination from reality often only serve to strengthen it. Chief among these changes is the introduction of the so-called vaccines themselves.
Prasad, for example, points out in his video-post that society already passed two “natural stopping rules” to masking children:
These are all articles that are making a similar case […] “What is the stopping rule?” There was a natural stopping rule. The natural stopping rule was, when all adults have been offered a vaccination, that’s a good stopping rule. Another stopping rule might be when the 5-11 year old vaccine was made available to parents and kids who so chose to pursue it. Now of course there are countries around the world who haven’t so chosen among healthy kids 5 to 11, such as Sweden. […] And now we find ourselves trapped. We find ourselves in a situation where there are no clear off-ramps. And the reason there are no clear off-ramps, of course, is when you don’t know under what circumstances an intervention works, you have difficulty knowing under what circumstances you can safely stop an intervention, and that’s the crux of the dilemma that all these articles talk about.
But what actually happens to the pro-mitigation argument, when the pseudo-vaccine is made available to children? Well, that only makes things more dire - as not all children are able to take the pseudo-vaccine. It would seem that American children are subject to homeopathic risk logic: The rarer the risk, the greater the “tragedy” of failing to prevent it. As Kline would put it:

Thus, every “concession” to the notion that it was ever reasonable to force American children to postpone their childhood in the name of safety - as though every day a child spends in stasis is not squandered forever, as though children could suddenly re-plug into a missing year of childhood somewhere else “down the line” - only renders a realistic assessment more “irresponsible.” And the Urgency of Normal is rife with such concessions.
It begins with the ingratiating invocation of the trope that Omicron has magically made it permissible to utter realities that were true all along, quoting Tom Frieden on twitter:
18 months ago irresponsible and wrong to say:
-Covid similar to flu
-Many people hospitalized/dying have positive tests, not sick from Covid
- Most important to protect the vulnerable
Omicron is different.
Now: That's basically correct.
Covid is adapting to us, we need to adapt.5
But it was never irresponsible to say these things. It was always a manifestation of mentally deranged, secular-religious psychosis to say otherwise. SARS-CoV-2 is literally similar to the flu; there is no qualitative description of either virus’s impact on human life that could not validly apply to the other, except in our disparate reaction to the two.
So just what do the authors hope to gain by endorsing, from the very start, the notion that this virus was ever more “urgent” than “normal” to begin with? How can “normal” truly be “urgent” now, if it was “irresponsible” and “wrong” 18 months ago? Rather, this introduction places the entire argument immediately in Prasad’s trap: The toolkit starts off by affirming an amorphous, undefined risk-calculus under which mitigation provided a “benefit” somewhere in the past, and then attempts to extricate the present from that calculus even though comparison with an undefined benefit is impossible.
Affirming the “protection” offered by the pseudo-vaccines (over and over, as the toolkit goes on to do) only repeats the error:
COVID poses very little threat of serious disease for students in highly vaccinated communities.
COVID is a flu-like risk for unvaccinated children. Extraordinary measures in schools are not justified.
Vaccinated children have almost no risk of severe disease. Omicron does not change this.
Teachers remain well protected by vaccination, with boosters important in older age groups.
But from the start, “COVID” also posed “very little threat of serious disease” for students in totally unvaccinated communities. If the “protection” of Covid-vaccination is elemental to the question of whether children should be subjected to mitigation routines, then something was implicitly unacceptable about the previous danger; that danger being the one reaffirmed by the toolkit’s wielding of the UK Omicron-wave hospitalization rates:

So, ~16 hospitalizations per 100,000 30 year-olds is (implicitly) unacceptable, but ~7 is fine? Why? What if the rate before the injections was 30, and after was 16? Would we still need to mask our children then, because 16 = bad? Just how does Covid-vaccine efficacy against severe disease actually change anything about the calculus for subjecting children to useless mitigation measures? The given outcome is still rare before or after the vaccines; the mitigation measures are still useless.
At what actual benchmark for Virus Danger, in other words, do the authors propose that “normal” becomes “urgent”? A number is never offered.
This gets to the crux of why Prasad’s “natural stopping points” were never fated to make any difference in masking children. The Covid vaccines never could have delivered society from a fear that was fundamentally irrational to begin with. Phobia only feeds on the rituals of protection that are designed to appease it. The Covid-vaccines were not an off-ramp from fear of the Virus. They were an off-ramp from confronting the irrationality of that fear; they were a bandage placed over the psychic wound of remembering what society had come to forget: Death is out there.
This gets us to the central backwardness of the current movement in favor of “realism”: Insofar as Omicron has revealed a growing schism in the media/expert elite mindset, it is a schism between those that still believe in the Covid vaccines, because they cannot mentally process the reality of universal mortality, and those who have accurately perceived that the Covid-vaccines were not a deliverance from death at all.
As an avatar of this psychic inversion, consider Freddie deBoer,6 who has been railing against continued Fear of Virus from within the crumbling fortress of mRNA-delivered protection against Virus Danger for most of the winter. In today’s outburst (emphasis added):7
Meanwhile the evidence that the vaccines8 keep you out of the hospital9 and alive10 grows and grows, and now it appears that “long Covid,” if real, is much less of a concern for the vaccinated [this links to an Israeli study based on survey responses, which found much less benefit for participants under 60 years old, i.e. deBoer’s age group11]. Get vaccinated, please.12
The purpose of these vaccines is to allow us to go about the work of being human beings.13 It would be a bizarre and sad not to take advantage of the blessings of medical science,14 obtained at great cost,15 by living as much as you can.16 Most people appear to be doing so. But there remains a very vocal contingent of people who do not want us to take advantage of the affordances of vaccines. These people are typically explicitly pro-vaccination but functionally anti-vaxx, as they insist that vaccines do not provide the kind of protection that could permit people to live anything akin to normal lives.
Just how is it that deBoer imagines himself any more reasonable than the “anti-vaxx” pro-vaxxers? His paean to the mRNA transfections is itself a confession of abject terror over the virus: Without the synthetically-delivered protection of these experimental injections, he would not be “allowed” to go about the work of being a human being. His ability to live would be directly curtailed. And anyone not taking these injections will, upon encounter with the virus, personally wind up in a hospital, suffering from Long Covid, and dead.
But thanks to the mRNA transfections, these universal, inescapable, inevitable outcomes will now only occur to, let’s say, 1/2 of the humans they would have otherwise. So gosh, with such “blessings of medical science” as these at hand, why can’t that “vocal contingent” let life get back to normal?!
For deBoer, the fig-leaf of the Covid vaccines is enough to seal his palpable, rabid terror of The Virus in a box labeled “Protected by Science.” This delusion achieved, he then wonders aloud at the fellow Pandemic Hallucinators who still lacerate themselves with the symbols and rituals of mitigation, who can’t take solace in the magic fig-leaf of protection that lets him imagine Death is Not Out There. But it is the vocal contingent, not he, who understands the fig-leaf for what it is.
The Covid vaccines have not banished death from the Earth, and never will do so. If anything, deBoer’s maniacal vaccine-utopianism broadcasts that he is psychologically further from accepting Covid Vaccine Failure, and moving on with life, than even the likes of Justice Breyer and Whoopi Goldberg. For him, it is not only relevant but essential that the evidence for severe efficacy keeps “growing and growing” (even though therapeutics could have the same impact), because he senses, intuitively, that the sand can drain from this bucket at any moment, casting him back into the apocalypse.
But really, just how is anyone supposed to take their advice for not living in fear from a grown man who resorted to injecting an experimental drug to protect himself against a virus that never seriously imperiled him to begin with? DeBoer’s blanket advocation of Covid-vaccination for the non-elderly merely broadcasts his internalized (and externally-projected), infantilized refusal to accept the possibility of death.
So where does that leave American children, particularly in the urban and coastal outposts of crazy? Will the “tide” really turn, at any moment, ushering in a sudden flood of rational risk assessment among their negligent adult caretakers? Or is the media/expert elite, and the TV-watching groupthink, further from being able to speak like adults about the issues than ever? Is “Omicron realism” going to snap American adults out of their trance of fear, when “Wuhan strain realism” couldn’t? Is the marginal protection of the Covid-vaccines going to render it socially permissible to downplay rare severe outcomes among the young, when the only “difference” the protection makes is that those outcomes are… well, still rare? Or does every resort to such arguments only feed the fear anew?
Even the authors of Urgency of Normal, in their repeated invocations of the protection offered by the Covid vaccines, seem to confess their own ultimate reliance on wishful thinking:
In adults over age 65, a booster dose restores protection against hospitalization to pre- Omicron levels (90%).
The enhanced protection appears durable, remaining at 90% for at least 10 weeks, the longest monitoring to date.
The UK has decided not to recommend additional boosters. Three doses does the job.
Double-dosing had “ten weeks confirmed protection” a year ago.17 So why didn’t that “do the job”?
And what, at last, of Covid-vaccine skeptical substack? Is this where American adults will develop the rhetorical tools to speak honestly about the virus? It seems unlikely. Here, our avatar of perpetual infantilization is Alex Berenson, who still persists in downplaying Long Covid altogether, and dismissing severe efficacy of the Covid vaccines outright:18
To Berenson, it cannot be acknowledged that the Covid vaccines reduce hospitalizations or death, because if they do, then no argument against them is morally sustainable. This is merely the mirror image of deBoer’s vaccine utopianism: Of course a marginal improvement in rare outcomes would imply that these injections offer deliverance from our self-inflicted fear; therefor, absolute vaccine-nihilism is the only recourse possible.
And nowhere in the entire arena of adult discourse, it would appear, is there anyone still willing to tackle the ghosts of 2020: If it is the elderly or “immunocompromised,” almost exclusively, who are at risk from this virus, then sorry, they need to take their lumps. It’s “irresponsible,” “wrong,” and frankly insane to suggest otherwise, and always has been! Life belongs to the living, and the future belongs to the young. And the young require a functioning, open society to support them.
Of course, even most elderly were never truly at risk; and the rest can be effectively protected by therapeutics - but at the point where society’s children must wait for adults to hash out the exact burden upon the elderly to begin with - to sort out just where the scales of death lean - the moral argument that “normal” childhood is not only “urgent,” but sacred, is already surrendered.
And that is the argument that needed to be made two years ago; and it is the argument that still needs to be made. If this virus kills more than the flu, well, so what? Does that mean it is actually “different” from the flu, or just that it is like flu, but more-so - as it was so allegedly “wrong” and “irresponsible” to say before Omicron? Is dying (being allowed to die) from the flu, or an equivalent virus, actually some moral crime to begin with - or isn’t it, in fact, the natural order of life?
And while Omicron-era adults fret over whether the moment is now, at last, ripe to violate these calcified taboos, children yet trudge through schools wearing cloth muzzles. The ghosts of spring, 2020 yet drive the plot; and yet we, the actors, seem less willing to speak their names than ever.
So, no - I do not think the “tide” is particularly close to turning. For even if the terror and endless obsession over SARS-CoV-2 fade - as they likely will do in the coming years - the injection has ensured that there will always be an asterisk next to society’s eventual “learning to live” with the virus.
Today’s children will either grow up in a region and culture that feels they should not be sacrificed for (mostly older) adults, just to make (mostly younger) adults feel some sort of moral purpose - or they will be psychologically abused for the rest of the decade, as well as subjected to the medical experimentation of the mRNA shots.
Healthy children, likewise, will either grow up where they are not spiritually crucified on the alter of “rare tragic childhood illness,” by being subjected to endless visual, verbal, and physical signals warning of a might-as-well-be-imaginary danger, or grow up to imagine themselves as biologically nonfunctional, sans medical intervention.
And the fall-out from those conditions, where they have obtained and will continue to obtain, will haunt human life for decades to come.
This is the world we are living in. The children spared from this disaster are those who live where “wrong” and “irresponsible” ways of thinking about the virus were embraced well over a year ago. Where the vulgar, mortal, non-utopian lifestyle of normal was reclaimed long before a shred of elite permission was issued to do so.
For the others, who have spent this era in the enclaves of crazy, there is no “undo” button for the most sweeping exercise in child abuse in history. And for many, if not most of these children, the “old normal,” urgent or not, is already a permanent psychological impossibility.

Henderson, Jennifer. “Doc Group Calling for Kids' Prompt Return to Normal Met With Swift Criticism.” (2022, January 28.) MedPage Today.
which reviews
Balsitas, S. et al. “Children, COVID, and the Urgency of Normal.” (pdf)
Whether Covid-vaccinated children will still fare well against the virus long-term is a still open question. Since childhood innate immunity was completely protective for almost all children, there is nowhere to go but “down” for almost all child recipients. Since current studies (see: “Scienceme Street”) have only looked at outcomes during the short window of “infection efficacy,” there is no data on how Covid-vaccinated children will fare when they experience their “breakthrough” infection, compared to the unvaccinated baseline.
Yes, she made that Freudian slip, and it went uncorrected.
That’s not to say that there isn’t an overarching, centrally planned narrative - aka, a conspiracy. Just that the conspiracy has had to adapt itself to and operated within the confines of the emergent mass psychosis. This renders the conspiracy not necessary to explain events; but also makes the conspiracy less implausible.
@DrTomFrieden (twitter)
DeBoer, before parlaying his volatile social media presence into a lucrative substack, wrote a few good essays, which I read at some point. I no longer remember what they were about; for me, my mental impression of the author was completely rewritten when he became “The guy who posted the Red Scare / Alex Jones photo.” It was via this bizarre episode that I became aware of deBoer’s vaccine-utopianist crusade against continued mitigation.
DeBoer, Freddie. “Covid as Liberal 9/11.” (2022, January 31.) freddiedeboer.substack.com.
(they’re not “vaccines”)
(not me; I was never at risk of going)
(again, not me)
An age-stratified analysis showed that the associations reported in the current study were largely confined to older age groups (above 60 years), a finding not consistent with a previous study reporting that the protective effect was confined to younger age groups
I cannot offer a personal take on the authors’ analysis of their own results, since they do not provide an age breakdown of infection rates (the study reports the age-breakdown for uninfected and infected respondents together by Covid-vaccination status, and then total infected by Covid-vaccination status - so there is no way to scrutinize the provided risk ratios for “long Covid” symptoms according to actual infection rates).
(again, not a “vaccine”)
(what?)
(what?)
(why do I need to “take advantage” of a medical crutch to do this?)
The disparity in severe outcomes between the double-dosed and the triple-dosed in the UK is partially an artifact of the aggressive push for boosting among the elderly, which introduced a short-term “healthy user bias” strongly disfavoring the double-dosed (as individuals who happened to already be in the hospital with an associated positive test for SARS-CoV-2 were forced to remain in the double-dosed cohort, while the rest were boosted)
Previously reviewed in “Truth Bombs (as a verb).”
The mass psychosis is the hardest obstacle to overcome. There is always an excuse to keep moving the goal post. But what if, but what if, but what if... That 30% of people have become incapable of accepting and managing risk in their lives and acknowledging their mortality in a healthy way. I feel encouraged each time I see someone have an awakening. Dr. John Campbell's obvious shock at the actual deaths from covid in England and Wales. Vinay's videos about the CDC Director's blatant lying. Two great examples that gave me hope. However, how do you get through to the, frankly, stupid people who can't understand enough to be awakened? How do you get through to those who have put their own survival above everything else- the mother putting her covid positive child in the trunk. The parents sending their 4 year old to school in an N95 with cloth mask over it. The parents who enrolled their children in clinical trials. These stories make things seem hopeless.
Kline MD says children's lives are at stake. All evidence says no, they're not. Which children is he worried about? If he has patients who are immunocompromised, they might have better risk with the vax. Most kids are safer without. Or do his fees rely on a steady stream of vax patients? Vax advocates all seem to need the business. They're not interested in anybody health, just our sickness. It's a very sick industry.