A new study claims to find strong evidence of (higher than normal) cognitive decline in older Brits infected with SARS-CoV-2. And… the evidence is pretty strong.
The following essay reviews the study, but precedes said review with a meditation on how we should think about the risks of infection. Readers who simply want an overview of the study should scroll down to the section labeled “In the Bank.”
I do not purport to peddle fear, nor to sell the reader courage. You must dispense with the former and take up the latter on your own, or else be running around all the time with materialist talismans that crumble apart eventually.
In January, I teased an upcoming piece exploring my hunch that the wave of “Virus Trutherism” which was raging in Covid-vaccine-skeptical substack comment threads at the time was, in fact, a manifestation of germaphobia. Sadly, this would-be, life-changing masterpiece of psychological insight never materialized, in part because I’m not fully convinced by it myself, and in part because I also had a hunch that the Virus Trutherism fad would wane on its own, thanks to most of the Truthers coming down with “Omicron” (BA.1) before long.
But the basic idea of the hunch, was that the Truthers - those who would populate comment threads everywhere, in January and February, to insist that contagious disease is some kind of mass hallucination which they vaguely seem to imagine was invented in 1880 - were reactionary virus-fearers who had also (rightly) been skeptical of the experimental injections when they first rolled out.
They were “reactionary,” in that the choice to avoid the mass experiment had suddenly become less easy than the year prior, when the fraud of herd immunity implied that even the non-injected would be able to put the virus behind them, and when the evidence that the experimental injections prevent severe outcomes didn’t seem so strong.
What does someone who decided not to take the experimental injections, but didn’t expect the choice to be complicated, do upon finding out that it is, in fact, complicated?
Some deny that severe efficacy and Long Covid have any possibility of being true facts in the world, as opposed to just phantoms of anecdote and bias1 (“they won’t actually take our lives!”). Some peddle theories for how the injections will, in some way or other, inevitably “make the virus worse” for every recipient - theories which vary from plausible to embarrassingly sophomoric2 (“they may take our lives, but it turns out that they will take the lives of the people whose lives they don’t take even more!”). And some simply declare that there isn’t even such a thing as viruses3 (“they don’t even exist!”). Why, you can’t be “infected” (scoff! the absurdity!) by something that isn’t real! That certainly makes the decision simple.
In this, the simplifiers and extreme-takers and Virus Truthers are all just the mirror-image of those who refuse to acknowledge that the entire world taking an experimental medicine before the experiments are even done is crazy; both have been driven into their respective positions by fear of the virus, a lack of faith in their own immune systems and the human body’s capacity for healing, and a disbelief in the inevitability of death.
All of this, as I’ve said in my previous concern-trollings4 on the subject, weakens the anti-Covid-vaccine argument by not only skirting it, but shrinking away from it altogether.
Taking an experimental injection - especially one that forces the body to replicate the most pathogenic element of the virus, and was designed to promote dispersion and evade breakdown5 - is, well, pretty self-evidently a bad idea. And there’s reasons to at least imagine that the (widely suppressed) therapeutics which seem to prevent severe outcomes can also help prevent lingering symptoms (simply extrapolating from the fact that they seem to work on said symptoms after the fact), while it’s not at all clear that the injections can do the same,6 especially since they may replicate and thus exacerbate those symptoms to begin with. That said, to deny that some will die from the virus - to insist it is not a “grandma killer” - is to explicitly give in to the idea that if it is a grandma killer, we should all individually and collectively let our lives be defined by fear of it, which is a bunch of childish nonsense. Everybody dies. “Life” is what we do in the meanwhile.
There’s the argument. It’s messy, and nuanced, and it doesn’t meet the demand for “zero tradeoffs” that this giant global game of Who Is the Real Spiderman?! seems to cause people to adopt. But it’s still the argument.
The Fog of Research
So, what does this long-winded perspective on the personal aspect of the risks of the virus have to do with evaluating research on those risks?
Well, in acknowledging that the virus might look scary in the research, it’s also important to keep in mind that it will probably look scarier than it is. (In fact, this was foreseeable from the very start, which is why the game was always rigged in fear’s favor as soon as society bought into the fear to begin with.) Three of the reasons for this, which are all synergistic:
The fog of research
There’s almost no way to look at infection outcomes that doesn’t introduce distortion and selection bias. Early studies calculated infection outcomes using only the severely ill and hospitalized, because tests were not widespread; later studies calculated infection outcomes in settings where those who were going to seek health care anyway were also screened with PCR tests, because tests were widespread. And etc. It is hard to compare any two groups of humans, because the entire point of the comparison is that they are not the same. And modern research conventions like “adjusting” results and “matching” controls are akin to magic rituals on a good day, and an obvious opportunity for researchers to cook their own results on a bad day (like MMWR release day, if you’re the CDC). It is easy for scientific findings to be illusory.
But, this cuts both ways. Bias can also hide, or make unclear, a valid biological reality. So, a study that finds that Long Covid outcomes are associated with “believing” an infection occurred, and not so much a positive test, aren’t really saying anything about whether infection is causing Long Covid except that the question is hard to sort out.
It can both be true that the findings regarding Long Covid are an artifact of bias, and that mild infections really are messing up some people’s lives.
Publication bias, and the Replication Crisis in general
Related to above. These ailments were already ongoing in science before the virus; and both would ensure that studies that fail to find evidence for risk would not always counter-balance or overturn studies that seem to find risk, especially in the realm of mainstream media reporting.
Discounting the negative
Lots of things in life are risky; lots of commonplace infections would probably be associated with surprising long-term effects if science had enough money to look at them all. By suddenly focusing so intensely on this virus, before our understanding of “baseline viral risk” was anything near accurate, we collectively ensured that SARS-CoV-2 was scored against an absurd standard where viruses (and life) are expected not to carry any risk at all.
It is thus easy to create a super-virus just by looking too closely at a regular virus.7 This was knowable in advance, because it has happened before.8
There is no better proof of this perversion of our perspective than the argument that children and teens need to be made “safe” from the virus, even though that likely makes no difference (as in literally zero difference) to the overall risk of “experiencing a health downturn of some sort” in these groups. They will still face a gauntlet of viral (and internal) immune challenges, and their success in that gauntlet will largely be determined by the competence of their immune system. That’s literally how “gauntlets” work.
So if our subject today is long-term neurological outcomes after infection with SARS-CoV-2, with poorly-understood etiology, just what is our baseline? Perhaps the flu?
The most common extra-respiratory complication of influenza is the development of CNS disease. Influenza virus infections have been linked to a wide array of neurological diseases, beginning with the 1918 ‘Spanish flu’ pandemic, which was associated with an outbreak of encephalitis lethargica and subsequently post-encephalitis parkinsonism years later. Acute CNS diseases include febrile seizures, acute onset brain dysfunction, meningitis, encephalitis and encephalopathies. In addition, influenza viruses have been linked to the development of Guillan Barré syndrome, Kleine Levin syndrome and transfer myelitis. Besides acute CNS manifestations, influenza viruses have also been associated with neurodegenerative diseases. Interestingly some strains are more frequently associated with CNS disease than others. Recent examples are the 2009 H1N1 pandemic virus and HPAI H5N1 virus.[…]
The pathogenesis of influenza virus-induced CNS disease in humans is largely unknown. Influenza virus-associated CNS disease could be an indirect effect of the infection, due to systemic cytokines, a direct effect of virus entry into the CNS, or a combination of both9
With all these factors collaborating to favor “false-positives” in humanity’s effort to research the “super-virus” qualities of SARS-CoV-2, I have at times taken an antagonistic approach to the results - particularly when it comes to infection outcomes during pregnancy, where I don’t think there even are very many false-positives (as in, studies simply do not show higher risk), and yet the alleged risks of infection are regularly asserted anyway in order to promote the experimental injections. And those few studies that have suggested a risk in this realm are, I feel, all works of malpractice.10
But in other realms, I have tried to be more open. In last month’s terse visit to the VA cardiac outcomes study, I suggested that the results were largely an artifact of the bias toward hospitalized and ICU-treated cases, and without this bias might be similar for any other type of infection:11 In other words, that we were in the territory of the first and third bullets.
The study by Douaud, et al. is not at all so easy to downplay.
So with the caveat that we should always be mindful of publication bias and “discounting the negative” - and one more reminder that these were infections without the support of therapeutics, and that it is still uncertain whether the Covid vaccines can prevent non-severe, long-term outcomes - let’s look at what seems to be a very well-done study that provides strong evidence that even mild infection with SARS-CoV-2 leads to increases in cognitive decline among (some of) the elderly.
In the Bank
As far as resolving the issues of selection bias built into most attempts to track infection outcomes, you can’t ask for better than “the most detailed, long-term prospective health research study in the world.”
51 was the minimum age for a Biobank participant during the infection-exposure window used by Douaud, et al.12 So nothing in this study should necessarily apply to the young.
401 participants were recorded as positive for infection with SARS-CoV-2 after a previous Biobank-scheduled brain-scan (we’ll just use “infected” to refer to the case subjects here, for simplicity). Most were either asymptomatic or mild infections; only 15 required hospitalization. Infections were, all in all, somewhat recent at the time of the second scan for most subjects - so we should be hesitant to accept some of the reporting that has described these results as implying anything about (un-) likelihood of eventual recovery:
For these 401 infected, changes in MRI readings in their next Biobank scan were compared with matched Biobank controls who did not have a reported infection (definition for “infected” in bold).13
UK Biobank offers a unique resource to elucidate these questions. With the data from this large, multi-modal brain imaging study, we use for the first time a longitudinal design whereby participants had been already scanned as part of UK Biobank before getting infected by SARS-CoV-2. They were then imaged again, on average 38 months later, after some had either medical and public health records for COVID-19, or had had two positive rapid antibody tests.
Those participants were then matched with controls who had undergone the same longitudinal imaging protocol but had tested negative to the rapid antibody test or had no medical record of COVID-19.
The infected had greater changes in several areas and associated regions, mostly in the same direction of natural aging. The difference in changes to regions associated with smell were the most stark.
We identified significant longitudinal effects when comparing the two groups, including: (i) greater reduction in grey matter thickness and tissue-contrast in the orbitofrontal cortex and parahippocampal gyrus,
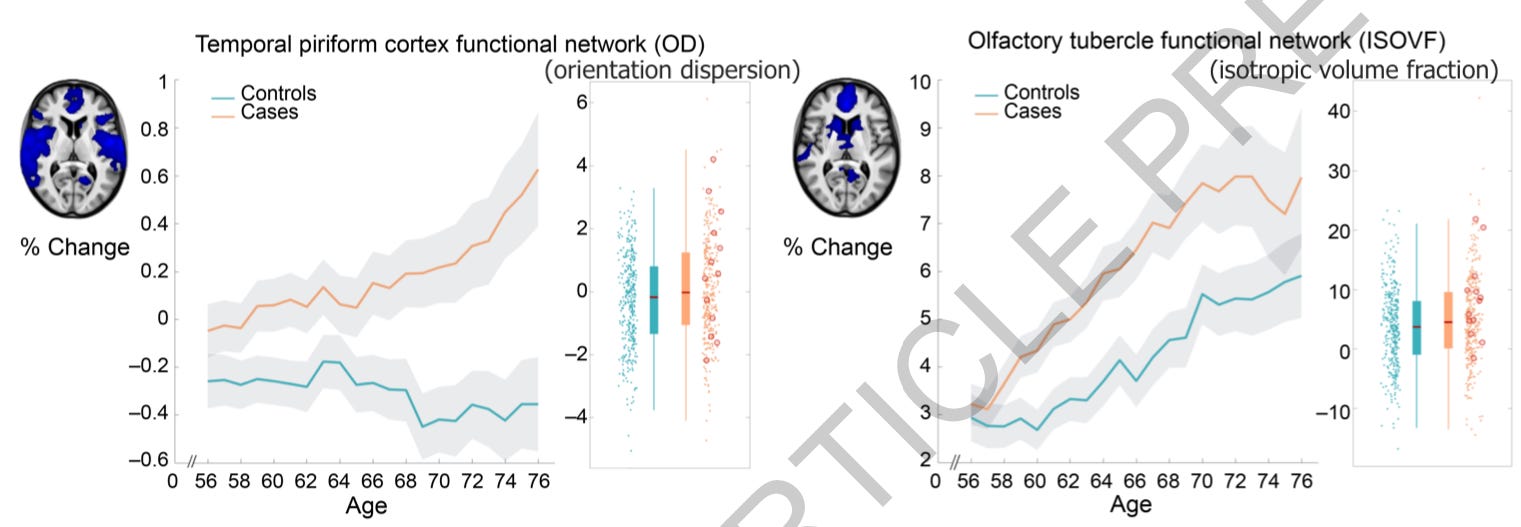
(ii) greater changes in markers of tissue damage in regions functionally-connected to the primary olfactory cortex,
“Within the olfactory system, direct neuronal connections from and to the olfactory bulb encompass regions of the piriform cortex (the primary olfactory cortex), parahippocampal gyrus, entorhinal cortex and orbitofrontal areas.” (The functional networks were evaluated as MRI cannot reliably image the piriform cortex or olfactory bulbs.)
and (iii) greater reduction in global brain size.
Perhaps more importantly (because the impact of changes to specific brain structures cannot be easily quantified), the infected also had greater decrease in performance in cognitive tests.
However, these SARS-CoV-2 positive participants showed a worsening of executive function, taking a significantly greater time to complete trail A and particularly trail B of the Trail Making Test
All effects were still observable even when removing the 15 hospitalized subjects, but not their corresponding (usually less healthy) controls (the graphs above are based on the simple, all participants model).
There was no difference in the overall time between scans of both groups (in other words, it is not as if infection just resulted in the subjects delaying an appointment and actually having “gotten more older” than the controls14). And controls ended up being a bit older at first scan than the infected used to match them; though on the other hand the infected were somewhat lower-scoring on one cognitive test (not used for the analysis) at first scan than their matches.
Most of the infections occurred during the UK’s autumn, 2020 wave15 - again reinforcing that a “severe infection bias” was not at work here, nor any weird Covid-vaccine-rollout related bias.
The biggest limitation in the design was the loose definitions used to define infection. And yet, as the authors note, this should have only made it more difficult to observe a difference in brain changes, so that these results should be presumed as under-stating, if anything, the actual effect of infection.
However, it is worth noting that any potential misclassification of controls as positive cases (due to false positives in testing) and positive cases as controls (due to the absence of confirmed negative status and/or false negative tests) could only bias our results toward the null hypothesis of no difference between cases and controls.
The design is essentially flawless except for how few “positive controls”16 were available for a “respiratory infection benchmark,” as will be mentioned below. Beyond that, the authors were thorough in hunting for pre-existing phenotypes (as in patterns of brain structure) via statistical processing, to see if any such patterns could account for the effect. Although I am skeptical of the power of these types of magic statistical rituals to remove a confounder if there is one, it’s relevant that the authors put in the extra effort. None of the models based on the subtle patterns could account for the higher rate of brain changes. And, again, it is impressive that these findings should be associated with a positive PCR or (double) antigen test at all.
Where the study falters, is in attempting to see how these results compare to other types of infections. There were only 11 cases of (non-SARS-CoV-2) associated pneumonia, and only 5 of influenza, among brain-scanned BioBank participants. Both cohorts showed different differences of change (vs control) than the SARS-CoV-2 differences (though there was overlap in the influenza group, in a pattern of changes in the brainstem), but with such a small set, it’s not clear if these results should carry too much weight as far as verifying that we are seeing a true signature for this virus.
On the other hand, the coherent signal for changes focused on areas of the brain connected to smell suggests an overlap with the signature symptom of mild infections with SARS-CoV-2, as the authors discuss in depth.
Individual Outcomes
Averages are not fate. As the authors note, “Our statistics also represent an average effect; not every infected participant will display brain longitudinal abnormalities.” It should also be kept in mind that there were more subjects and controls in the “younger” end of the age spread, so that the overall difference in change for all participants is not as great as it appears when changes are plotted by age.
Individuals are not averages. On the olfactory network plot, for example, there are plenty of orange dots that are below the average for the controls, including three hospitalized infected (circled).
Those individuals did not experience a greater than control average change, regardless of what the average was for infected participants - and ditto for every other plot.
Additionally, the scan 1 values buried in the Supplementary Materials show divergence between the infected and controls, usually starting at age 72. This could mean that the difference in measured changes at Scan 2 are, to some extent, exaggerated by some hidden selection bias for the older participants.
Mystery Mechanism
The final limitation, is that this study can tell us almost nothing about which aspects of infection were driving the observed outcomes. Aside from hospitalization and context of testing, almost nothing was known about what was different between infection experiences:
This is all they know about the “infected” group (some hospital data not shown, as it was too limited for any analysis).
Naturally it wouldn’t be very illuminating to compare the home-based and “diagnostic” vs each other, and so the only comparison available was between the hospitalized or not. And so, aside from the strong apparent centrality of changes to smell-related regions of the brain, this paper cannot offer any hints on how infection is bringing these changes about in the non-hospitalized group.
In the Supplementary Discussion, the authors write:
Whether our findings, which seem to delineate a clear limbic network of the primary and secondary olfactory and possibly gustatory cortex, reflect a corollary effect of the infection, an indirect brain-related pathophysiological process of SARS-CoV-2 through either anterograde degeneration or neuroinflammatory process, or a direct effect of the spread of the virus itself, remains to be elucidated.
The possible mechanisms proposed here are 1) Direct spread of the virus into the brain, 2) Anterograde degeneration, when neurons die off in a sort of domino-effect style, so that the virus is knocking out parts of the brain indirectly by damaging terminal neurons, 3) Inflammation, 4) A “corollary” effect, such as atrophy induced by shutting off smell.
Perhaps inflammation should be considered the most likely (or microclotting, not mentioned above, but which I will be discussing in an upcoming post), but the “corollary” effect is the most interesting suggestion. Essentially, the authors are proposing (cautiously, since they have no clinical data to back it up) that lack of olfactory stimulation, itself, could disrupt and dysregulate the brain in the fashion observed by this study.
From the main Discussion section:
Some of the most consistent abnormalities across hypothesis-driven and exploratory analyses and all group comparisons were revealed in the left parahippocampal gyrus (Table 4, Fig. 2, Supplementary Table 1) — a limbic region of the brain that plays a crucial, integrative role for the relative temporal order of events in episodic memory. Importantly, it is directly connected to the piriform cortex and entorhinal cortex, which are both part of the primary olfactory cortex . Similarly, the orbitofrontal cortex, which we also found altered in the SARS-CoV-2 positive group, is often referred to as the secondary olfactory cortex, as it possesses direct connections to both entorhinal and piriform cortex, as well as to the anterio olfactory nucleus. […]
The predominance observed in other studies of hyposmic and anosmic symptoms — whether caused directly by loss of olfactory neurons or by perturbation of supporting cells of the olfactory epithelium — could also, through repeated sensory deprivation, lead to loss of grey matter in these olfactory-related brain regions. Very focal reduction in grey matter in the orbitofrontal cortex and insula have been observed for instance in patients with severe olfactory dysfunction in a cross-sectional study of chronic rhinosinusitis .
A more extensive study of congenital and acquired (post-infectious, chronic inflammation due to rhinosinusitis, or idiopathic) olfactory loss also demonstrated an association between grey matter volume and olfactory function in the orbitofrontal cortex . It also showed that duration of olfactory loss for those with acquired olfactory dysfunction, ranging from 0 to over 10 years, was related to more pronounced loss of grey matter in the gyrus rectus and orbitofrontal cortex […]
So, there is overlap and ambiguity. It is obviously possible that the virus or damage from inflammation is simply following a physical path, from the nose to whatever parts of the brain are downstream; but it is also possible that in making the olfactory center of the brain “go dark,” the regions which normally integrate smell into other cognitive processes atrophy in kind.
As potential support for this suggestion, they offer the following:
In turn, the duration to complete the alphanumeric trail B was associated post hoc (as in, after they decided to go and look for it) with the longitudinal changes in the cognitive part of the cerebellum, namely crus II, which is also specifically activated by olfactory tasks.
It is an interesting thought - that the results of this study could be largely driven by the impact of not being able to smell (though, again, the other mechanisms seem more likely17).
I have yet to offer a post drilling into the difficult question of whether severe efficacy is or isn’t a manifestation of “healthy user bias.” The all-cause mortality figures for ONS and Scotland, for example, strongly suggest such an effect at play in the UK, as death rates are apparently low in the days after every injection for adults (see “Midsummer Maladies”); but I think it may be too short-term to account for down-the-road infection outcomes. It rather seems like a paradoxical result of their push to Covid-vaccinate nearly everyone, so that the “on the deathbed” group sorts out of every just-dosed window, but overall the just-dosed are not actually above-average-health - but this requires supposing that the unvaccinated populations are over-estimated in all age groups as well (due to individuals who are not in the country being counted as “unvaccinated”).
Meanwhile, the low Covid-vaccination rate of the elderly in Honk Kong, where deaths attributed to BA.2 are currently very high, may finally put the matter to rest. At the moment I am not sure if the government and media claims that deaths skew toward the unvaccinated should be given too much credit, however.
“Concern trolling” refers to any attempt to represent criticism of a given party as being “for their own good.” In my view, the term subsumes two other terms, Respectability Politics and Credibility Fetishism (the latter, my own invention). When used in a way not also described by those two other terms, I don’t really have a problem with concern trolling, and so I only apply the term to myself here to signal self-awareness: “I know I am committing a rhetorical taboo.” As for the other two contexts, both of them are ridiculous since Respectability and Credibility are so easy to manufacture. Otherwise society wouldn’t believe in “safe and effective” vaccines to begin with, given their real history.
Severe efficacy is plausible as most severe outcomes and deaths follow widespread viremia (spread of the virus into the bloodstream), and likewise were effectively prevented by monoclonal antibody treatments, once those were finally embraced (leaving aside possible toxic effects from anti-spike antibodies themselves for now). But does suppression of viremia (by pre-existing anti-spike IgG memory immunity induced by the injections) do anything to prevent lingering symptoms? This depends on the threshold of infection needed to cause those symptoms - and it seems that that threshold is below “severe.”
In the case of my own (non-test-confirmed) bout with the virus, I chose to trust my own immune system. I ended up with two days of brain fog, but that was all. But my hunch is that therapeutics are effective at reducing lingering symptoms for those who might be at risk.
“Zero Polio,” which may or may not have contributed to escalating rates of paralysis (by, you know, driving adults to spray children with poison), resulted in part from widespread scientific refusal to accept near-universal asymptomatic infection. Instead, it was believed that most adults had antibodies (despite obviously never being paralyzed, since that was a rare occurrence) because the body just somehow made them out of thin air, as part of the aging process. (See Harrison, J. Hudson, N. (1940.) “Study of the Serum-Neutralization Test in Poliomyelitis.” J Bacteriol. 1940 Apr; 39(4): 405–427.) If humans want to see a super-virus, science will reveal a super-virus.
Here the study design gets a bit complicated, as there was a lot of variety in time between scans.
To keep the time between scans similar for the controls, controls had to be matched to the infected by age on the one hand but also have a time-between-scan value that contributed to the desired overall curve, leading to compromise on the former. Hence why the authors are a bit self-critical about the disparity in ages. However, it seems like here once again they have disfavored the control group, by assigning “long-inter-scan” controls to the older end of the spectrum (where between-scan declines are greater by default). For this, however, I am just making inferences based on the changes in squishiness in the scan 1 and 2 histograms:
Controls did not all go the same length of time between scans as their matched subjects. However, it seems like the authors’s sorting “aged” the control group more overall, again favoring the null hypothesis.
ICU delirium is an long accepted phenomenon sometimes lasting for months after discharge. As an RN I can testify to the atrocity of locking someone into a room and depriving them of the company of anyone who might care about them (except of course random 'space suited' staff who were overwhelmed with just the donning of equipment before even going into the room). These people often didn't even see a smile, so the previous post wondering about how being locked down might much more negatively impact the sick...even those who were home and sick is worth a study or two. I was 69 when I had covid in oct'20. I completely lost my smell for one week while I also experienced severe headache, body pain, exhaustion and general misery. When I recovered, my sense of smell came back quickly. My 48yo daughter had very mild symptoms but her sense of smell is still impaired. I want you to know that I enjoy your stack. It is like being back in college, though in a class way too advanced for me. Even though you slammed a stack I really like, (I read about twenty) I really appreciate different points of view so that my opinions aren't so deeply entrenched that I can't learn. I would like you to address the similarities and differences between antibiotic resistance and vaccine resistance at some point if you have time. I find it odd that I never see this issue discussed by the scientists who insist that the unvaccinated are responsible for the mutations in this virus. Would they also say that those who never use antibiotics are responsible for mutations in bacteria and fungus? I am pretty sure that it is overuse of antibiotics as in earaches, colds and of course the pervasive use in agriculture that is driving the antibiotic/antifungal resistance that kills over one million people a year. I would like to know if I am mistaken. Thanks for a really great read.




















I’m just wondering how anyone was able to notice declined brain function in a Brit. ;)
ICU delirium is an long accepted phenomenon sometimes lasting for months after discharge. As an RN I can testify to the atrocity of locking someone into a room and depriving them of the company of anyone who might care about them (except of course random 'space suited' staff who were overwhelmed with just the donning of equipment before even going into the room). These people often didn't even see a smile, so the previous post wondering about how being locked down might much more negatively impact the sick...even those who were home and sick is worth a study or two. I was 69 when I had covid in oct'20. I completely lost my smell for one week while I also experienced severe headache, body pain, exhaustion and general misery. When I recovered, my sense of smell came back quickly. My 48yo daughter had very mild symptoms but her sense of smell is still impaired. I want you to know that I enjoy your stack. It is like being back in college, though in a class way too advanced for me. Even though you slammed a stack I really like, (I read about twenty) I really appreciate different points of view so that my opinions aren't so deeply entrenched that I can't learn. I would like you to address the similarities and differences between antibiotic resistance and vaccine resistance at some point if you have time. I find it odd that I never see this issue discussed by the scientists who insist that the unvaccinated are responsible for the mutations in this virus. Would they also say that those who never use antibiotics are responsible for mutations in bacteria and fungus? I am pretty sure that it is overuse of antibiotics as in earaches, colds and of course the pervasive use in agriculture that is driving the antibiotic/antifungal resistance that kills over one million people a year. I would like to know if I am mistaken. Thanks for a really great read.