


pHarmaccounting
ANOTHER study purports to support Covid vaccination during pregnancy while hiding half the data! No, really! Another one - I know! It just keeps happening!

A study from Scotland, cheerfully anagrammed “COPS,” claims to show a grave threat from infection with SARS-CoV-2 during pregnancy, and strong protection from the Covid vaccines. The findings are all likely to be misleading. The results don’t include information patients would want to know; the study manipulates its own results, and hides half of the raw data.

Nope, not taking the “education before editorializing” approach to this one:

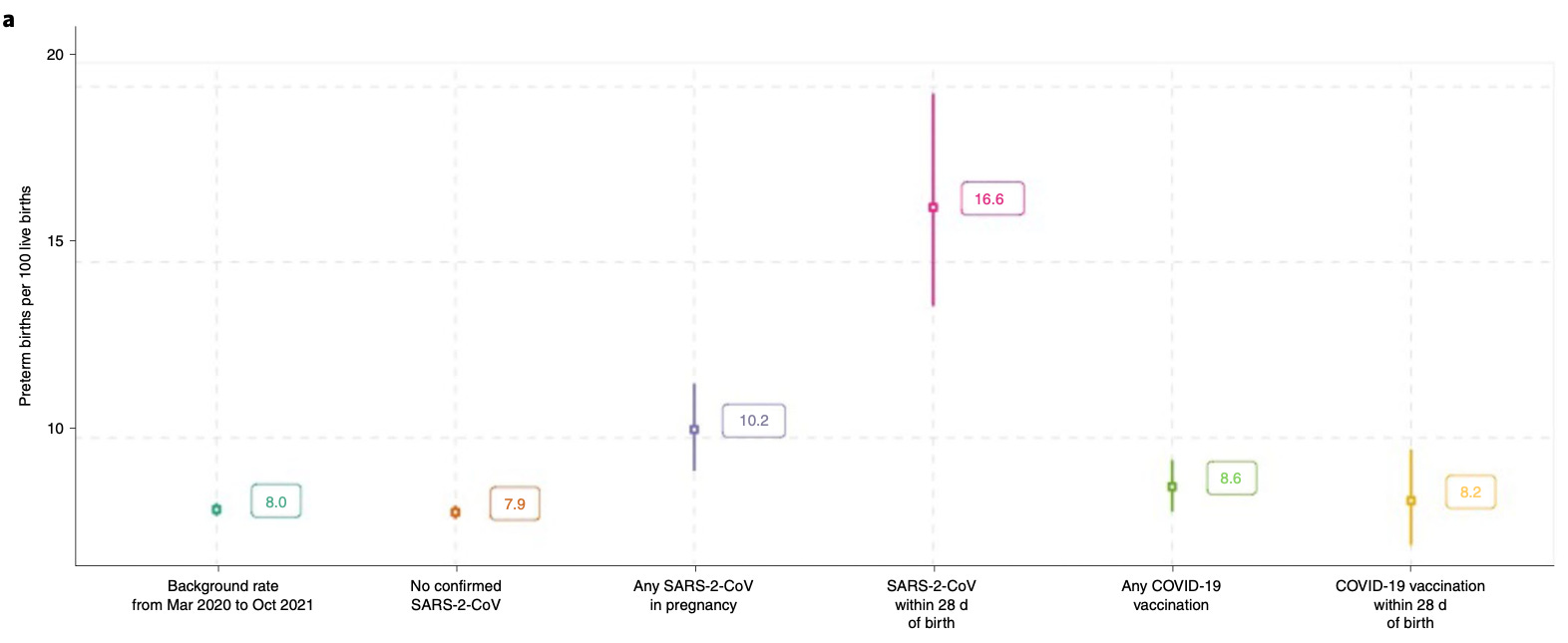
Researchers found that 17% of babies born within 28 days of their mother developing COVID-19 were delivered prematurely - more than three weeks before their due date - compared to the background rate of 8%.
Baby deaths (stillbirths and deaths in the new born period), were also more common among women who had COVID-19 in the 28 days before delivery, compared to the background rates seen in the whole population during the pandemic.1
The Public Health Scotland presentation (emphasis added in above) is a forecast of how American health propaganda will be portraying the Stock, S. et al. “COVID-19 in Pregnancy in Scotland” (COPS) study’s results. Already, MedPage Today is quoting a coauthor’s press statement to conclude:
"Our analysis indicates ... that vaccination appears to be the safest and most effective way for pregnant women both to protect themselves and their babies from the complications of a SARS-CoV-2 infection," said Aziz Sheikh, MD, a co-author on the study, in a press briefing.2
No, it doesn’t.
Most of my study reviews take a light touch. I try to guide the reader through the study design, demonstrate how there were other conclusions available for the authors to draw, and often enough show where they made one or two choices to disguise these flaws. The COPS study defies this approach. It is a work of relentless mathematical manipulation, as if to wring every last penny of profit from their data set - more akin to a corporate tax filing than a bounced check, COPS subjects the truth to death-by-a-thousand-cuts, and yet follows all the rules to a T, so that any attack on the findings will seem desperate and confused. Worse, we are forced to audit the result using the metaphorical equivalent of a corporation’s annual report instead of their filing itself.
Really, I’d like to skip to the “Well, even if these findings were true” part - but here the flaws are too great; the findings are fabrications.
In sum, the COPS findings are the product of a cornucopia of flaws tiny and grand; and yet as even apparently related findings cannot be explained by the same flaws, it is only in the synthesis that the crime is complete.
So, let’s get to work.

Finding: 16.6% of births (101 of 610) within 28 days of infection were preterm.
Flaws:
“With, not from” false-positives.
The authors deliberately set the study window to start on the same date as a recommendation was issued to screen all maternity admissions for infection.3 Somewhere in the low-20%s of preterm births are medically induced - meaning they may be preceded by a prior visit, and thus a potential screening.4
There may have been something like 3,478 overall preterm births during the study window (the reported background rate of 6,381 extends beyond the study window, so the true study window background rate has to be estimated5). If ~750 of these (3,478 x .22) were medically induced and thus preceded by recommended screening for infection, they may have contributed heavily to the final count of 101 post-infection outcomes. (There is no diagnostic appraisal in any of the study results.)
Note that this may also apply to normal term births, since “infections” were scored up to the day of birth. On the other hand, it may be the case that medically-induced preterm births in particular were often preceded by multiple screening tests. There is no way to tell.
Cohort deception, pt 1 - Hidden vaccination status.
The authors do not report how many post-infection preterm births were Covid-vaccinated.
They have this data: There were 1,117 breakthrough infections during pregnancy during the study period. Covid-vaccination rates are reported for post-infection perinatal deaths but not for preterm births, the headline finding and the implicit subject of Sheikh’s claim regarding protection from injection. This is potentially uber-significant given the drop-off in infection efficacy in the UK before the autumn wave, and the screening/medical-induction issue mentioned above. As we will revisit in the next segment, the Covid-vaccinated could in fact be driving observed preterm outcomes after infection.
Regardless, without the data on whether Covid-vaccination protected against the (possibly false-positive) post-infection preterm outcome, there is no basis for Sheikh’s claim.
Cohort deception, pt 2 - The 1st-dosed.
For the purposes of hospitalization and critical care outcomes (below), the authors count recipients of the 1st dose of Covid vaccine as “unvaccinated” for 21 days. It is likely (though a bit unclear, from the text) that this also applies to the preterm outcome analysis. If so, 1st-dose + infection or screening-induced PCR+ preterm births could drive some of the 28 day results. There is no way to tell.
Cohort disparities.
There’s lots of them. They could cut in any direction. Infections during pregnancy scored worse for socioeconomic vulnerability, but were younger, compared to Covid-vaccinations during pregnancy. However, there is no corresponding demographics data for infection + preterm births.6
Risk window and cutoff confusion.
This one is for the footnotes, as it is quite wobbly.7
Possible post-infection “normal term birth protection bias.”
This one is for the footnotes as well.8
Even if true:
The “preterm risk window” is primarily between weeks ~31 and 36, not for the entirety of pregnancy. Further, risk increases resulting “from being unvaccinated” should be interpreted as the infection risk increase multiplied by risk of infection during pregnancy or the preterm window (hint; it’s tiny). See next segment for overall and preterm-window risk increase calculations.
Finding: 10.2% of births (241 of 2,364) any time after infection were preterm.
Flaws:
Cutoff deception.
There were almost certainly more pending post-infection normal term births than preterm births at the October 31 cutoff, since the latter take longer to cross the “finish line.”9
The 28-day-window results, in fact, may over-correct for this, thanks to the evil that is math. The overall results cannot. There were 2,586 post-infection pregnancies still ongoing at the time of the cutoff. Additionally, the authors acknowledge a potential reporting lag of 3 months;10 if preterm births are reported more quickly than normal term births, this could further distort results. As we will see in Figure 5, below, these hazards potentially exaggerated post-Covid-vaccination preterm rates as well.
So why is the result - 10.2% - less dramatic than the 28-day-window value? Likely due to the screening/false-positive problem being more prevalent in the latter category (hence the reversed order of flaws).
“With, not from” false-positives.
As above. The overall post-infection outcomes still include all 101 of the 28-days-post infection outcomes, including all potential false positives due to screening on visits preceding medically induced preterm births.
Cohort disparities, and Cohort deception, 1 and 2.
As above. All of these still apply to the overall outcomes set.
To reiterate before the analysis below, the authors do not demonstrate or assert that Covid-vaccination removed the association between infection and preterm birth, whereas they did do so for other outcomes.11 In fact, with this data missing from the report, it’s possible that Covid-vaccination increases the association.
Even if true:
Risk increases resulting “from being unvaccinated” should be interpreted as the infection risk increase multiplied by risk of infection during pregnancy or the preterm window. Women deciding whether to get Covid-vaccinated, in the nonexistent world where the authors gave us data that showed “preterm protection” from the Covid vaccines, must calculate their risk reduction based on the likelihood that infection would occur to begin with.
There were 3,833 “infections” (“novel PCR-positives”) among 69,295 unvaccinated pregnant women (87,694 overall - 18,399 Covid-vaccinated) during the study window (December 1, 2020 to October 31, 2021). This window included two waves, with all completed or ongoing pregnancies overlapping with one or both, representing a robust proxy for normal pregnancy exposure risk (since we’re not looking at miscarriages anyway). Thus, observed risk of infection during (unvaccinated) pregnancy expressed as a risk multiplier is
3,833 / 69,295 = .0553
We can thus use the study’s Figure 5 to compare adjusted “added risk” associated with “being unvaccinated” vs Covid vaccination. Note that the cutoff bias does seem to have negatively impacted preterm rates for births after Covid-vaccination, due to a likely higher portion of ongoing pregnancies in that set:12

Finding: Miscarriage Risk?
Flaw:
There was no analysis of miscarriage outcomes for infection or Covid-vaccination. Why?13
Finding: Stillbirth and neonatal fatality rates post-infection, overall and 28-days-after
Flaws:
“With, not from” false-positives.
As above. There were 273 stillbirths and 179 neonatal deaths (deaths within 28 days of a live birth) in the background cohort (including infected and Covid-vaccinated), which comes out to an estimated study window background of 149 and 98.14 Could some of these - especially the 98 neonatal deaths - have been preceded by an admission leading to a screening PCR test (“infections” were counted up to the date of the end of pregnancy)? Obviously.
(As with preterm outcomes, screening tests could also work in the other direction, due to PCR-testing at birth; the question is whether the rates of screening for healthy births vs complicated births is the same.)
Given that there were 10 total stillbirths and 4 neonatal deaths observed 28 days after “infection,” the “with-not-from” hazard could account for the entire signal. (Overall post-infection outcomes only add 1 stillbirth and 4 neonatal deaths, among 2,364 completed pregnancies.)
Cohort disparities, and Cohort deception pt. 2.
As above.
Uneven exposure risk.
Unlike with preterm births, the authors are able to report that none of the stillbirths or neonatal deaths associated with infection occurred following the 1,117 infections among the Covid-vaccinated. This may be due to the timing of the august wave. As Covid-vaccinated breakthrough infections likely did not occur before august, there was a smaller sample for 28-day risk and a cutoff bias for longer-term birth outcomes (including for post-infection live births that had not yet passed the 28-day risk window). This cutoff bias would have been less substantial for unvaccinated pregnant women, who were exposed in both the winter and late summer waves.
Finding: Stillbirth and neonatal fatality rates post-vaccination, overall and 28-days-after
Flaws:
Missing data.
The authors suddenly do not report discrete figures for stillbirth and neonatal death rates, when divulging outcomes after Covid-vaccination, whereas the values are given in plain text for outcomes after Covid infection. These must be reverse-calculated using given values for live births, completed pregnancies, and overall perinatal deaths (both stillbirths and neonatal deaths).
Yes, it’s that obvious there’s something to hide.
(Note beforehand that the definition for “vaccination,” for purposes of 28-day post-exposure windows, is a bit ambiguous in this part of the study analysis, as mentioned in Cohort Deception 1 and 2. Does it refer to any dose? Completing the second course? Bleh.)
Stillbirths, Covid-vaccinated overall
5,766 completed pregnancies - 5,752 live births = 14
Neonatal deaths, Covid-vaccinated, overall
25 perinatal fatalities - 14 stillbirths = 11
Neonatal deaths per 1,000 live births, Covid-vaccinated, overall
(11 / 5,752) x 1,000 = 1.9
Stillbirths, Covid-vaccinated 28-days
1,635 completed pregnancies - 1,632 live births = 3
Neonatal deaths, Covid-vaccinated, 28-days
7 perinatal fatalities - 3 stillbirths = 4
Neonatal deaths per 1,000 live births, Covid-vaccinated, 28-days
(4 / 1,632) x 1,000 = 2.45
Background rate, March 1, 2020 to October 31, 2021
(179 / 80,183) x 1,000= 2.32
Neonatal deaths per 1,000 live births, Covid-infected, overall
(8 / 2,364) x 1,000 = 3.38*
Neonatal deaths per 1,000 live births, Covid-infected, 28-days
(4 / 610) x 1,000 = 6.56*
*Scotland recommended screening-PCR-tests for all maternity admissions
That’s it: 2.45, higher than 2.32. The authors had the math to show a (likely under-sampled, inaccurate) association between Covid vaccination and neonatal deaths. But chose not to. In fact, they hid the raw numbers.
In the second part of Figure 5, stillbirths and neonatal deaths are lumped together, presenting the rosy picture that receipt of Covid-vaccines confers protection from both (among all completed pregnancies). The lower rate of stillbirths which drives these results is, again, a possible artifact of timing: Low sample size (with potentially twice as many incomplete pregnancies among the Covid vaccinated, as assumed in our miscarriage analysis, since the authors do not give a value15), “immortal time bias” (late-2nd and 3rd trimester Covid-vaccinations may boost the denominator for viable births), a reporting lag; or it may just reflect demographic differences among cohorts:

We could apply the same multiplier above to demonstrate the actual apparent risk increase for “being unvaccinated” (I may update this image in an update), but let’s wrap up.
Finding: Hospital admissions and critical care rates per “infection” lower for Covid-vaccinated
Flaws:
Cohort deception, pt 2 - The 1st-dosed.
Again, for the purposes of hospitalization and critical care outcomes, the authors count recipients of the 1st dose of Covid vaccine as “unvaccinated” for 21 days (emphasis added):
To explore the impact of vaccination status on SARS-CoV-2 infection, women were grouped as follows: unvaccinated (no previous COVID-19 vaccination before the date of onset of COVID- 19 or with one dose of vaccination ≤21 d before the date of onset); partially vaccinated (one dose of vaccination >21 d before the date of onset of COVID-19 or two doses of vaccination with the second dose administered ≤14d before the date of onset); or fully vacci- nated (two doses of vaccination with the second dose >14 d before the date of onset of COVID-19).
I don’t usually make a big deal of “worry window” infections; but here it is incredibly conspicuous that the 1st-dosed were counted as unvaccinated rather than being excluded from analysis altogether. Thus, admissions for adverse events, per the policy in place during the study period, would have prompted a screening-PCR-test - all PCR-positives in the adverse-event 1st-dosed group would have driven recorded outcomes for the “unvaccinated”! It’s absurd.
“With, not from” false-positives.
As above, but worse than ever. For both the 1st-dosed and the authentically unvaccinated, who are lumped together as “unvaccinated,” admissions or critical care outcomes would have resulted in a screening test.
Here you might be thinking, but don’t the authors only record outcomes that follow a PCR positive as being infection-associated? Yes, for birth outcomes. No, for hospitalizations! In fact (emphasis added):
Hospital and critical care admission data.
[…] SARS-CoV-2 infection was defined as associated with a hospital admission if the woman was admitted to hospital ≤14 d after the date of onset of COVID-19 or if the date of onset occurred at any point during a hospital admission (as per Public Health Scotland standard definition). […]
SARS-CoV-2 infection was defined as associated with a critical care admission if the woman was admitted to critical care ≤21 d after the date of onset of COVID-19 or if the date of onset occurred at any point during a critical care admission
The authors deliberately included 100% of screening-caught and hospital-acquired infections during non-related admissions! Want to see the raw numbers for how many “infections” in fact preceded, not followed admission?
Tough cookies.
Note, again, that this false-positive hazard would apparently apply to the Covid-vaccinated once infection efficacy waned. So it might be a stretch to imagine that it drives too large a share of unvaccinated outcomes. After all, it is unlikely that there were zero actual hospitalizations for “Covid-19” among unvaccinated pregnant women. However, this study does not accord with previous research on the hazards.16
Where does that leave us? At face value, the infection outcomes observed among the Covid-vaccinated pregnant women suggest that for them, mild outcomes are the norm:
“Unvaccinated” (including 1st dose ≤21 days) infection outcomes
3,833 infections - 748 associated hospitalizations - 102 critical care
“Partially vaccinated” infection outcomes:
567 infections - 47 associated hospitalizations - 1 critical care
“Fully vaccinated” infection outcomes:
550 infections - 28 associated hospitalizations - 1 critical care
That all looks quite good. However, without excluding “with-not-from” cases, there’s no way to tell just how good. If anything, the authors have done the Covid vaccines a disservice on this front.
On the other hand, this could be an artifact of smaller exposure risk (no with-not-from false positives until infection efficacy drops, toward the end of the study window) and a higher rate of true false positives (PCR-positive in absence of infection) among (more recently) Covid-vaccinated.
Cohort disparities.
As above. Infections during pregnancy scored lower for socioeconomic markers. Did this drive associated hospitalizations, including among screening- and hospital-acquired PCR-positives? Or did the younger age among infected pregnant women make up for this? Who can say.
Finding: Anything in this study should inform decisions about pregnancy risks
Flaws:
A study that seeks to answer the question, “does Covid-vaccination improve outcomes in pregnancy,” should look at actual overall outcomes, not compare only the “infected” (including already-admitted) and injected.
Recipients and controls should be observed from exposure - “observing” outcomes by trawling the results after-the-fact substitutes the question “Are high-risk pregnancies more likely to be unvaccinated” for “Are unvaccinated pregnancies more high risk?” They may not have the same answer.
Finally, removing the risk of infection with SARS-CoV-2 does not remove the overall risk of being infected with “something,” and experiencing a related complication, during a given pregnancy. In fact, it might not make any difference to the overall risk at all; or the improvement may be very light.
Deciphering the actual “benefit” of the injection is the first step to considering whether it makes sense for pregnant or would-be pregnant women. (The second step is to weigh that benefit against the risks of the injection itself).
This study does not tell pregnant women what they need to know; only what the authors want them to think.
Finding: “Vaccination appears to be the safest and most effective way for pregnant women both to protect themselves and their babies from the complications of a SARS-CoV-2 infection.”
Flaw:
The author of this statement, Aziz Sheikh, participated in a study so staggeringly deceptive and manipulative, and frankly such a pain to decipher,17 that everyone involved should be driven from society by a mob armed with pitchforks.

See “Scottish study leads to calls for more pregnant women to get fully vaccinated.” Public Health Scotland.
which reviews today’s target:
Stock, S. et al. “SARS-CoV-2 infection and COVID-19 vaccination rates in pregnant women in Scotland.” Nature Medicine.
D'Ambrosio, Amanda. “COVID Vaccination in Pregnant Women Protective for Infants.” (2022, January 14.) MedPage Today.
(Stock, S. et al.)
Early in the pandemic, it is highly likely that there was under-ascertainment of cases of SARS-CoV-2 infection due to limited test availability and testing capacity (Fig. 4a). Restricting the COPS cohort to only data from 1 December 2020 onward (the date that routine SARS-CoV-2 testing was recommended for all admissions to maternity care and the COVID-19 vaccination program started in Scotland)
This is bunk. Uptake of Covid vaccines among pregnant women does not begin until June, 2021 anyway:

So the author’s rationalization for the December 1 start date is just that. Lack of testing in spring, 2020 is not a reason to exclude autumn 2020 wave outcomes, except that they might have had fewer false positives, taking away from the headline finding.
22% medically induced per preterm rate assumed from US studies and Norman, J. et al. (2009.) “The effect of changing patterns of obstetric care in Scotland (1980-2004) on rates of preterm birth and its neonatal consequences: perinatal database study.” - obviously, the real rate varies by year anyway.
By date, December 1 2020 to October 31 2021 is 11/20 of March 1 2020 to same = .55. By outcomes (91,183 study window pregnancies - 27,358 ongoing)/(144,548 background window pregnancies - 27,358 ongoing) = .545. Thus study window preterm births estimate is 6,381 background x .545 = 3,478.
The authors claim they will attempt to parse this data in a follow-up (once the ink on all the headlines is already dry):
A limitation of our study is that the data presented are descriptive and we have not adjusted for the potential confounding influence of demographics, obstet- ric or medical conditions. A fully adjusted analysis of all pregnancy outcomes (including early pregnancy outcomes) is planned
The question of how many preterm and normal term births occur 28 days after infection is also the question, “How many infections occur during or just before weeks 37 onward, vs how many that occur in the longer risk window for pre-term births, which are then followed by preterm birth?” It’s not clear that this question is enlightening to begin with. Isn’t it like comparing the odds of hitting the aircraft carrier vs the submarine, on any given guess? On the other hand, the infection still has to precede the preterm birth on the date that it actually happens, not just the entire window of possibility that it could have happened.
In fact, this hazard seems to poison results for post-Covid-vaccination results as well - we will visit this in Figure 5, in the next segment.
Further, how does cutting off the study while pregnancies are still ongoing affect those results? (This creates a clear bias for the all-post-infection results, as discussed in the subsequent segment; but it may run in the opposite direction for 28-day window results). Does the longer risk window for preterm births mean that more pending 28-day-window preterm births get censored by the cutoff (relative to normal term births), or fewer, or no change? It’s impossible to appraise this, given the study design. The authors also report that data latency may extend up to 3 months before the cutoff (see footnote 10) - if births are not reported as quickly as preterm births, this could further distort the results.
Again going back to the question of how looking at 28-day outcomes may “create” the preterm association to begin with.
37% of “novel PCR positives” (i.e. “infections”) during pregnancy were during the second trimester (1,850 of 4,950 overall, including among Covid-vaccinated). Subsequent PCR positives are censored for 90 days after. False positives due to screening during admission during the second trimester may have censored some post-infection normal term births, contributing to the low denominator of 610, while subsequent preterm births would still score in the post-28 day window.
Alternately, the bias may work in the other direction. 24% of all post-infection normal term births (509 of 2,123) occur in the 28-day window and 31.5% (1,557 of 4,950) of infections are during the third trimester overall. Thus, normal term birth seem to be over-represented in the 28 day window (since it theoretically corresponds to ~1/3 of 31.5%).
There’s no real way to know.
Hilariously, this is the mirror-image of the error made in criticism of the “Preliminary Findings” paper, which derived an 82% “miscarriage rate” by incorrectly excluding ongoing pregnancies from the denominator. See, again, “The ‘Preliminary Findings’ Paper.”
(Stock, S. et al.)
A caveat is that due to source data latency, the most recent 3 months’ pregnancy data may be less complete (there may be some under-ascertainment of the most recent pregnancies and end of pregnancy outcomes).
It’s quite conspicuous, actually - especially with the relevant paragraphs re-ordered (1,3,2):
[Paragraph 1] Of the SARS-CoV-2 infections in pregnancy that occurred in unvaccinated women, 19.5% (748 out of 3,833; 95% CI 18.3−20.8) were associated with hospital admission, compared to 8.3% (47 out of 567; 95% CI 6.2−10.9) of those in partially vaccinated women and 5.1% (28 out of 550; 95% CI 3.5−7.4) of those in fully vaccinated women. A total of 2.7% (102 out of 3,833; 95% CI 2.2−3.2) of the SARS-CoV-2 infections in pregnancy that occurred in unvaccinated women were associated with a critical care admission, compared to 0.2% (1 out of 567; 95% CI 0.01−1.1) of those in partially vaccinated women and 0.2% (1 out of 550 cases; 95% CI 0.01−1.2) of those in fully vaccinated women. This means that while 77.4% (3,833 out of 4,950; 95% CI 76.2−78.6) of SARS-CoV-2 infections in pregnancy occurred in unvaccinated women, 90.9% (748 out of 823; 95% CI 88.7−92.7) of infections associated with hospital admission and 98.1% (102 out of 104; 95% CI 92.5−99.7) of infections associated with critical care admission, were in unvaccinated women (Fig. 4d). To date, there has been one maternal death following SARS-CoV-2 infection in pregnancy in Scotland. [Summary: the Covid-vaccinated + PCR+ did better in hospital admission and critical care outcomes]
[Paragraph 3] Of the 2,364 total [post-infection] births, 11 were stillbirths (deaths in utero ≥ 24 weeks gestation) and eight live births resulted in neonatal deaths (death within 28d of birth), giving an extended perinatal mortal- ity rate of 8.0 per 1,000 births following SARS-CoV-2 infection at any point in pregnancy (19 out of 2,364; 95% CI 5.0−12.8). Ten of the stillbirths and four neonatal deaths occurred in babies born within 28d of the onset of maternal infection, giving an extended perinatal mortality rate of 22.6 per 1,000 births (14 out of 620, 95% 12.9−38.5) in this population. All perinatal deaths following SARS-CoV-2 infection in pregnancy occurred in women who were unvaccinated at the time of SARS-CoV-2 infection. We do not have access to detailed clinical records to assess whether COVID-19 directly or indirectly contributed to the preterm births and deaths seen following maternal infection. [Summary: the Covid-vaccinated + PCR+ avoided 100% of apparent perinatal death outcomes]
[Paragraph 2] A total of 2,364 babies have been born to women who had SARS-CoV-2 infection in pregnancy between 1 December 2020 and 31 October 2021. Of these, 2,353 were live births, of which 241 were preterm births (<37 weeks gestation; preterm birth rate 10.2%; 95% CI 9.1−11.6). Overall, 610 of the live births and 101 of the preterm births occurred within 28 d of the date of onset of the mother’s SARS-CoV-2 infection, giving a preterm birth rate among babies born within 28 d of SARS-CoV-2 infection of 16.6% (95% CI 13.7−19.8). [Summary: contribution of Covid-vaccinated to post-infection preterm outcomes not provided]
Covid-vaccination was also associated with an increased risk of preterm birth. This could be an overall risk or a two-factor risk (as in, Covid-vaccination + infection); the latter case indicating that Covid-vaccination either does not reduce the association between infection and preterm outcomes altogether, does not reduce it at all, or potentially increases it. Since the authors hide the data for how many post-infection preterm births were Covid-vaccinated, there is no way to know:
As discussed in footnote 13.
I attempted a rough guess of miscarriage rates following Covid-vaccination in the 1st 20 weeks:
18,309 overall Covid-vaccinated pregnant women - 5,766 completed births (with duplications for non-singleton pregnancies) = 12,543 pending ongoing
27,358 given overall ongoing pregnancies / 91,183 study window pregnancies = 30% study-window background ongoing rate. However, we’ll double that, since uptake of Covid vaccines among pregnant women doesn’t really start until June.
18,309 x .6 = 10,985 expected ongoing Covid-vaccinated pregnancies
12,543 - 10,985 = 1,558 est. terminated Covid-vaccinated pregnancies
13,933 / 34,413 = 40.5% gross (March 2020 onward) background non-induced termination rate (there were 20,480 apparent abortions in this timespan, representing 14% of pregnancies; obviously the difference in rate between the Covid-vaccinated and overall is unknowable since it depends on the same real number we are estimating).
1,558 x .405 = 631 est. non-induced terminated Covid-vaccinated pregnancies
((9,905 “1st trimester vaccinations” (any dose) x .8 arbitrary 2nd dose correction factor) + (9,317 “2nd trimester vaccinations” (any dose) x .6 arbitrary 2nd dose correction factor x 8/16 2nd trimester miscarriage exposure window)) = 10,719 est. first 20 week Covid-vaccinated
631 / 10,719 = 5.9% est. early loss rate
Notes: The actual rate of induced terminations for Covid-vaccinated women, which is not provided, can make a big difference. Were doctors in Scotland recommending Covid-vaccination before abortion, for example - or would Covid-vaccination during pregnancy indicate less likelihood of abortion, as might be more intuitive?
1,558 x .8 = 1,264 alt. est. non-induced terminated Covid-vaccinated pregnancies
1,264 / 10,719 = 11.8% alt. est. early loss rate
Nonetheless, the 5.9% result seems plausible, given “immortal time bias” (Covid vaccinations during pregnancy cannot rationally follow a miscarriage). In other words, it’s not as good as it looks, but it doesn’t seem bad, either.
Same math as in footnote 5.
Footnote 13.
See my “pregnancy risks snippet” in “Saving Private mRNAyn.”
Look at this mess!
Thanks for taking the time to pick this apart. It is deeply frustrating that someone, somewhere, apparently has access to maternity outcome data from the second half of 2021, but these numbers don't seem to have been made public, anywhere. I want to see that data! Particularly for August thru December!
The future of Scotland, killed by a clotting neurotoxin. I blame the TNI primarily. News would be reaching more people if the TNI could be broken.