I have been spending the last 24 hours “off the grid,” for the most mundane of possible reasons: The Grid is having an outage where I am. (I don’t have cellular data here either.) In the first hours I was not inconvenienced, being immersed in the dynamics of codon / amino acid semantics, of which I am belatedly cramming an understanding so I can belatedly deliver my promised follow-up to “Mouse Party.” Occasionally, I would switch back to the still-open tabs for the Xie, Y. et al. paper and Chudov’s commentary on the paper, and jotting more notes down on the composition notebook page. Mid-afternoon, I was struck with the error in Chudov’s post - at which point my internet outage became incredibly inconvenient.
While I had no doubt that the Covid vaccine recipients in the paper experienced elevated rates of reported myocarditis (as well as likely subclinical, unreported, and possibly misreported myocarditis) after injection, since these reporting trends are already well-established in studies looking directly at the topic, I was skeptical that a study designed to observe post-infection outcomes could simultaneously demonstrate the impacts of the vaccine, unless in the raw numbers.
Chudov’s post didn’t seem to be working with the raw numbers, but rather the calculated odds ratios in the supplemental materials, so I decided to work through the paper and his post on my own, to see if I came up with any errors. It was early into my reading when I lost internet, so I had no way to visit the paper’s supplemental materials for myself, nor to view comments on Chudov’s post, once I spotted the error.
As I am composing this in advance of my emergency visit to the village internet cafe, I still have no way to check these things. For all I know, this has all already been spotted by a commenter, or maybe there has even been an update by now. Apologies if this post is the equivalent of a sailing ship that doesn’t know the war is over. Additional apologies in advance for going dark after publishing, so that I can not respond to any alerts about whatever mistakes I am making of my own. Further, I am opting to publish my comments here so that they can be accompanied by illustrations.
Now to quote Chudov. Annotations on the supplemental material charts are his, since I can’t get to the original source:
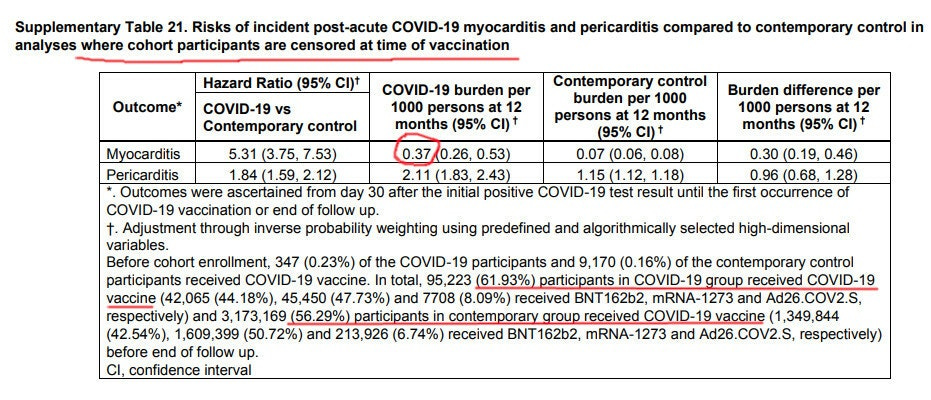
The VA study compares Control Group A from 2021 with Study Group (veterans who had Covid before Jan 15 2021). The first table (table 21) shows veterans myocarditis rates up UNTIL the time they get vaccinated (so no one is vaccinated in this table). Once vaccinated, they are instantly excluded (censored) from results in Table 21.
The result is here:
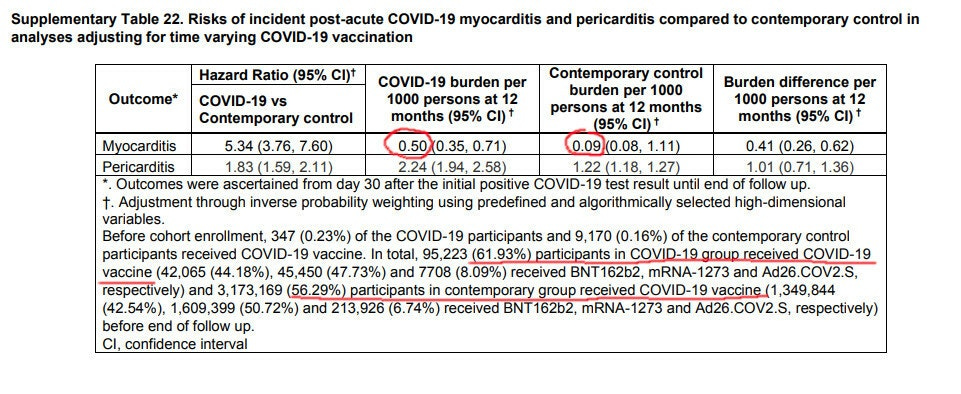
Here’s the same comparison of Covid-recovered vs Covid-naive veterans, however in this one they were included for the entire year, including many of them after they were vaccinated:
So, you can see that following up Covid-recovered veterans AFTER vaccination for the entire year, shows that vaccination INCREASED myocarditis burden from 0.37, to 0.50! That means that vaccinating 62% of the covid-recovered cohort (not even every member of it) INCREASED risk of myocarditis in the whole cohort, by 35%! (0.5/0.37 = 1.35)
Note again that only 62% of the covid-recovered cohort was vaccinated (and so 38% not vaccinated). But we can use algebra to calculate effect of vaccination, specifically on the vaccinated people.
This is where Chudov goes astray, since his reverse-calculation treats the outcomes for when Covid-vaccine recipients are censored after injection as though they represents outcomes for the never-vaccinated, and are thus able to be weighted as 38%. In fact, both the censored and uncensored outcomes still include the Covid-vaccinated. The latter includes them until the end of the study window and the former includes them only until they are injected. This compromises any attempt to reverse-calculate the impact of the vaccines. We can’t know the true rate of myocarditis among the never-vaccinated if it is not presented separately. And thus, we can’t know the rate of myocarditis amongst the Covid-vaccinated alone, especially if it’s unclear when just most of them were injected and censored.
And besides this, even if we knew the myocarditis rates for both unvaccinated and not, we could not decipher whether Covid-vaccination, itself, was elemental in an observed increase, or if this was a bias in who elected to get injected. We further can’t tell how this bias was handled by the papers’ noted “adjustments” for “high dimensional math nonsense.”
And so even if it is fair to assume the end result, given our current knowledge of the side-effects of the Covid-vaccines, these two tables do not comprise a secret document of “proof.” Obviously, they were not designed to. The authors are not attempting to look at this issue, and so do not bother to fabricate a valid control (though if the raw numbers are provided in the supplemental materials, the reader can attempt to reverse-construct a control). The study is examining the effect of infection; so naturally the only controls are the uninfected.
Onto my own analysis, further demonstration of the potential for these results to arise from bias in who received a Covid vaccine, and to the promised illustrations.
To understand why it matters so much what the authors’ are attempting to show, one must understand how utterly byzantine and reckless these types of study designs are. Here the authors take a large database likely crammed with built-in-biases, and add more bias by literally using the observed variable and outcomes to dictate when alleged subjects and “controls” are inserted or removed from the denominator, in the end so brutally mauling the data that the only way to validate the observed association between infection and cardiac outcomes is by seeing if the same brutal mauling magically produces the same association for “hypertrichosis, melanoma in situ, sickle cell trait, perforation of the tympanic membrane, malignant neoplasm of the tongue, B cell lymphoma and Hodgkin’s lymphoma.”
Imagine running a biological experiment in a lab that is so poorly-controlled that you have to assess and report how much of the output was also observed in the various drawers of your desk.
As the results for these negative controls are, again, hidden in the supplemental materials, I cannot offer the reader any assessment of the study’s headline findings. The effect of (PCR-proxied) infection on cardiac outcomes is much lower for the non-hospitalized, suggesting that only “serious” infection results in a substantial increase in observed cardiac events more than 30 days after PCR-positivity - or, that the observed increases are an artifact of the mere act of being hospitalized after PCR-positive test, despite the authors’ myriad attempts to rule out such a bias.
Such an artifact could arise from veterans with problems preceding diagnosis for cardiac issues being counted as hospitalized for infection due to coincidental PCR-positives, or that hospitalization, itself, causes these increases. Hospitals are depressing and stressful. And ICU-treatment is akin to physical trauma. Deciphering the role of the virus vs. the role of treatment for the virus is intrinsically difficult. After all, the “controls” are not also made to spend a week in a hospital, or be put on a ventilator, due to the withholding of inexpensive and effective therapeutics.
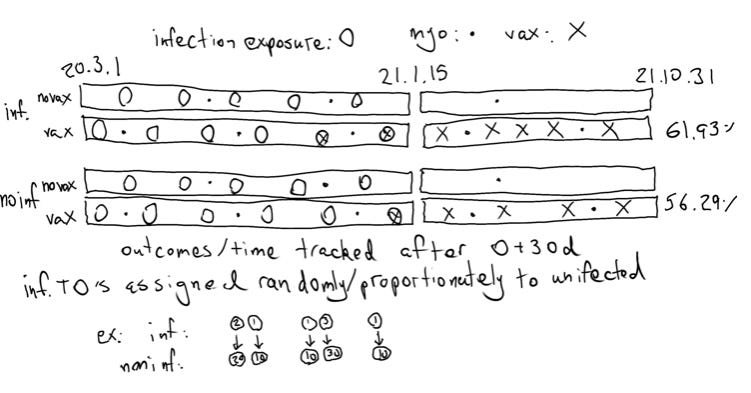
Randomly tapping the “controls” into the study ~37 at a time per every PCR positive further muddies the waters, even if it is likely to ensure that the controls enjoy the same immortal time bias as the infected. And censoring PCR-positive infected subjects and controls at the date of Covid-vaccination, as for table 21, further muddies the waters. It should be obvious at this point that these results are not safe to attack with basic algebra. To visualize the study design as it pertains to Covid-vaccination and myocarditis:
If you can make any sense of this without needing to spend an hour drawing things in your own composition notebook, congratulations: You are not me.
For the reader who neither can make sense of the illustration nor wishes to sort the mess out on their own time, all that is important is that subjects and controls are removed when they are injected, so they no longer contribute either to myocarditis outcomes nor to the tabulated person-years of exposure. This allows us to move into crude abstraction. The purpose of this crude abstraction is to demonstrate how easily a bias in who gets injected can create the appearance that the injection increases rates of myocarditis. We can run a simulation that creates exactly the results the study presents in Tables 21 and 22 if, in fact, veterans who receive the Covid vaccines were more at risk of myocarditis to begin with.
In this crude simulation, the never-injected are also at a lower risk of myocarditis to begin with, regardless of prior infection. However, the infected (both injected and never-injected) are at a higher risk than the uninfected. We see that the act of censoring the injected halfway through the study period can create the observed results for both groups. If “no infection, not censored” represents the true control, it turns out that the apparent elevation in myocarditis rates can appear even if the Covid vaccines do not increase incidence of myocarditis.
There is just one problem with this simulation (besides the fact that the results we are reproducing are adjusted for risk group anyway). The authors calculated the myocarditis rate two years prior to the study period. It was lower than our simulated “low risk” group:
This essentially refutes the simulation. But the purpose of the simulation was to show how fraught and unreliable this data is to begin with. Mission accomplished, in that case.
Chudov speculates that the higher rate of myocarditis for the uninfected is due to infections with SARS-CoV-2 that were not confirmed with a PCR+. Perhaps - but bear in mind that in most years, myocarditis is frequently a result of viral infection with something else. If SARS-CoV-2 is to some extent displacing this normal risk, it does not seem intuitive that after ruling out everyone who had a positive test for SARS-CoV-2, and who was Covid-vaccinated, the contemporary control rate shouldn’t in fact be lower.
And, once again, I have no doubt that the Covid vaccine recipients in this paper experienced elevated rates of reported myocarditis after injection, I am just skeptical of how well we can decipher this effect in the face of potential confounding bias.
In fact, the simulation that better explains the observed results assumes that the bias favors the injections, but that the injections are also causing increased rates. In other words, the reason the censored contemporary controls have a higher-than-2018 rate of myocarditis is because Covid vaccine recipients were older, or healthier, and at less risk to begin with. However, receipt of the injection turned them into the primary driver of myocarditis. And as in the previous simulation, the infected are also at a higher risk than the controls:
Here we have successfully simulated the results in Xie, Y. et al. I think this is likely to be what is actually occurring among the veterans in this study, though if it isn’t, blame the authors for foisting this statistically mangled garbage onto the world to begin with.






Imagine if this type of discussion were the type that dominated mainstream media. What a different and better world we would live in.
Good work! Clare Craig looked at it here as well
https://dailysceptic.org/2022/02/09/heart-problems-after-covid-are-much-worse-for-the-vaccinated-nature-study-shows-but-its-hidden-in-the-appendix/