
Forever Spike
A grand tour of the theories for how the Covid-vaccinated could sabotage unvaccinated immunity.


As accords with the remarks offered in the conclusion to “Myo-Card Me a River,” I am reluctant to wade into the myriad theories that have been going around for how this experimental, failing vaccination campaign will potentially threaten the yet-unvaccinated.1 To even address the issue, necessarily resurrects the circuitry of the plague narrative which needs to die; it reopens the door to the obsessive, media-hyped Stop the Spread Insanity when even many of the most deluded of Covid vaccine supporters are fervently against ever opening that door again. But as this is likely a short-term status - at some point, their faith in the pseudo-vaccine will collapse - the unvaccinated have to be willing to face whatever threats the virus may throw, even if it kills us, or the only future available to the liberal West is the perpetual plague police state.
That said, I will offer some “takes” on the hottest controversies. On the docket:

The Escape Mutant Disaster!
As articulated by Geert vanden Bossche, this is undeniably the most brilliant, far-sighted, and widely recognized of the Vaccine Disaster Theories.3 Vanden Bossche’s central insight was that suddenly confronting the virus with the same, cookie-cutter anti-spike protein antibody challenge over and over would lead, where else, to the virus solving said challenge, well in advance of the virus being “extinguished” (which it can’t be, anyways). Vanden Bossche’s theory has set off a still-ongoing global “debate,” in which the Covid-vaccinated try hard as they can to rationalize away the fact that they, individually and collectively, are doing more to weaken the vaccines than the unvaccinated. Meanwhile the unvaccinated, try however hard they might, can not place more selection pressure on the virus in the direction of spike escape as the Covid-vaccinated - and on their own would take eons to rise a “perfect vaccine resistant strain” to prevalence according to random chance (although trillions of strains allegedly emerge every time a hummingbird blinks, only one becomes dominate during a given wave according to the pattern so far; and most cases occur inside of waves).
However, vanden Bossche’s theory has been rendered momentarily obsolete by the drop in infection efficacy, as remarked upon in “Boostermania.” And while the synchronous roll-out of boosters (as well as the coming wave of mandate-complying first timers) could place vaccine escape pressure back on the table this winter, the FDA is in the middle of staging a revolt on that very subject. The resurrection of the Escape Mutant Disaster thus appears to depend on some form of counter-attack from the elements of the administration that have been so aggressively teasing the booster rollout all month. For the moment, therefor, it is just one more known unknown.
Moreover, the harm represented to the unvaccinated in vanden Bossche’s theory, which he has elaborated upon in reply to the collapse in infection efficacy, is primarily the detrimental effect to the achievement of “herd immunity.” His entire point is that only natural immunity leads to that blessed, paradisiacal state.
As far as I can tell, vanden Bossche strictly employs the non-eradication meaning of herd immunity, but who can ever tell when this toxic, heavily weaponized term is bandied about. This leads to a disconnect between what his lay readers are interested in - namely, eradicating SARS-CoV-2 - and what he is interested in - achieving some vague condition of mathematically observable order, as far as I can discern.
If booster-escape-pressure in fact increases the pace of antigenic drift, the unvaccinated - recovered may be in for a symptomatic re-infection. The unvaccinated naive presumably would not have any more trouble with a vaccine-escape version as with a first-time encounter with the wild type. Both groups, as a population, might be more exposed than otherwise, but on an individual level this just amounts to a change in amount of risk, not degree of harm risked.
Edit, 9/27: For a discussion of the potential revival of the Escape Mutant Disaster theory in light of J.J. Couey’s compelling analysis of Nextstrain data, see “Saving Private mRNAyn.”
The Marek’s Effect Disaster!
This theory has been summarized in several different places, including by the blogger who goes by the handle “el gato malo,” who also originates the next theory in the list and operates the substack where a commenter inspired my own, final theory.5 Namely, it proposes that since a virus has to become “more contagious” to overcome the protection of a “leaky” vaccine, the immune systems of the unvaccinated become obsolete in the resulting vaccine - virus arms race.
Vaguely.
I’ve yet to see it clearly explained why “contagiousness” does not equal “deadliness” on one end of this theory, but does equal it on the other, for example. The theory posits, after all, that viruses always want to become more contagious, but not more deadly.
Thus, vaguely, Marek’s Disease Virus is promoting higher levels of shedding, via dander, into the feathers of vaccinated chickens, so it can give other vaccinated chickens a higher dose; but is doing so without harming the nervous system, thanks to the vaccine’s protection. But, why wouldn’t it already be doing exactly this with unvaccinated chickens? If more “shedding” makes it more contagious, it should always try to maximize shedding, while pulling “less deadliness” out of the magic genetic box implied by the assertion that viruses “make themselves less deadly.”
Replying to this theory requires me to go out on the limb constructed by my first Immune Equilibrium argument - where, of course, I ventured to put a label on said magic genetic box. Marek’s Disease Virus, notably, is a herpesvirus, which are addressed in Tenet 3-1 (though, I need to do some cleanup here):6
If a respiratory or gut virus happens to take on core immune evasion traits, it must learn to turn off those traits immediately upon access to vital organs, before further replication kills off the host. Immune evasion is a binary in high-frequency-spread pathways - there is no evolutionary curve to “more contagious / less deadly.”
This is obviously a simplification - Marek’s Disease Virus uses a blend of respiratory and skin / touch-based pathways. But it represents the core point.
There is, as far as I can tell, a giant blind spot in epidemiology about the reality that many of the most common viruses aren’t being stopped by the immune system at all.
Herpesviruses included, these familiar “foes” possess sophisticated immune evasion traits. Therefor, the only reason they stop before killing their host is that they are stopping themselves, via triggering of lysogeny, in the same way as phages use signal/timer pathways to detect when to enter and exit lysogeny. All of this flies in the face of Germ Theory Dogma, but it is a fact which has been evident for decades: If viruses can figure out how to keep a colony of bacteria alive, they can figure out how to keep a human child alive - as does, for example, Chickenpox (itself a herpesvirus).
I therefor propose that Marek’s effect, in vaccinated chickens, is merely the result of a mis-calibration of the virus’s signal/timer pathways. Upon encountering an unvaccinated chicken, the chicken is dead before the virus hits the brakes.7
This does not apply to a respiratory coronavirus without significant cellular immunity-evading traits, like SARS-CoV-2.
(This argument has been significantly expanded here.)
The Superspreader Disaster!
More plausible, is the proposition that vaccination reduces the association between symptoms and “viral loads” in the nasal cavity, leading to more asymptomatic spread. This proposal is one element of the nuanced speculation offered by el gato malo in a recent post attempting to make sense of the (I view as totally poisoned) data for cases and outcomes in the US.9 By various means, including greater rates of asymptomatic spread, and higher infectious doses, el gato malo proposes that the Covid-vaccinated are both promoting more cases among the unvaccinated overall and more severe outcomes per (unvaccinated) case.
Personally, I find the idea of inferring anything about either the virus or the effect of the Covid-vaccinated based on US hospitalizations and deaths rates hazardous. If, say, the universe were to teleport into my mind the pure, perfect knowledge that US hospitals are not intentionally placing the moderately ill on ventilators to kill them for higher revenues, thereby committing mass murder, then I will embark on trying to make sense of the otherwise “mysterious” surge in deaths in the US this summer. Until then, one can’t know what one can’t see.
Nonetheless, a higher rate of asymptomatic spread among the Covid vaccinated is plausible, regardless of the supporting evidence (since the association between viral loads, as inferred by PCR cycle counts, and “contagiousness” is an assumption, not a demonstrated fact). Many of the most common symptoms for infection do not have to do with viral shedding into respiratory tract. “Cough” shares space with “fever” and “tiredness” in the top three on the WHO list. If the Covid vaccines, even after they lose infection efficacy, continue to effectively inhibit viral shedding into the bloodstream (but not the respiratory tract), they plausibly take two of the earliest symptoms off the table.
For the unvaccinated, the condition of “symptomatic” therefor plausibly becomes true at an earlier time frame of infection in many cases. (I haven’t looked at whether any of these viral load studies plot “cough” alone as a separate qualification for “symptomatic.”) This, however, may cease to be true for infections that occur even further away from the time of vaccination than we have currently been able to observe.
Moreover, I am - I should say, was - disinclined to grant that greater encounter with asymptomatic spread, however derived, can lead to a greater final case count among the unvaccinated. That final value ought to be determined by the overall “infection potency” of the population in question, not by the removal of a source of transient friction against infection. The fuel will burn out when it burns out, regardless of how much more closely the coals are gathered.
But the last week has brought signs of a change of affairs. The Covid-vaccinated, once they leave the window of infection efficacy, appear to be experiencing negative infection efficacy, as measured in real time. This was first made directly visible in last week’s Public Health England update.10 It continues to be quite evident for the new “real time snapshot” posted by the agency yesterday.11 The Covid vaccinated are being PCR-confirmed infected more than the unvaccinated. Brits over 40 - who were Covid-vaccinated earlier than those under 40 - are testing positive at higher rates than the unvaccinated:
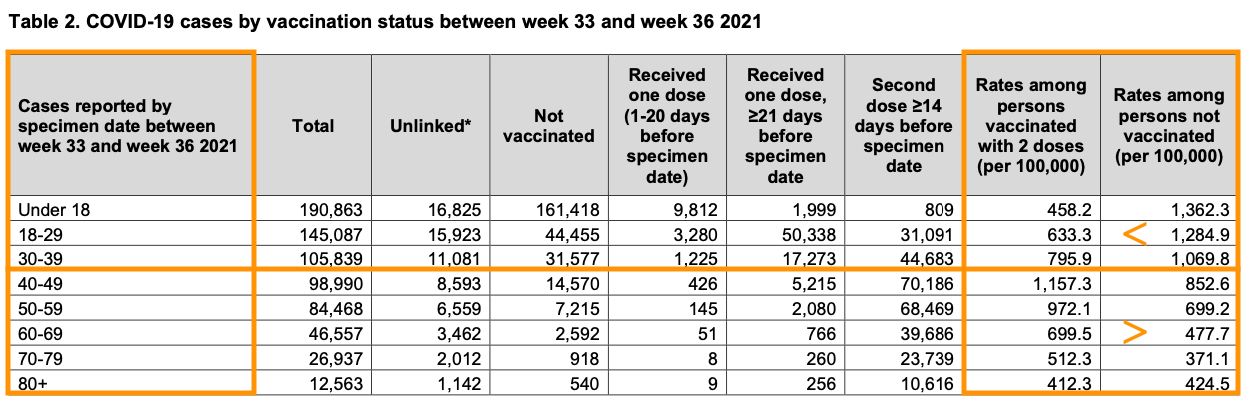
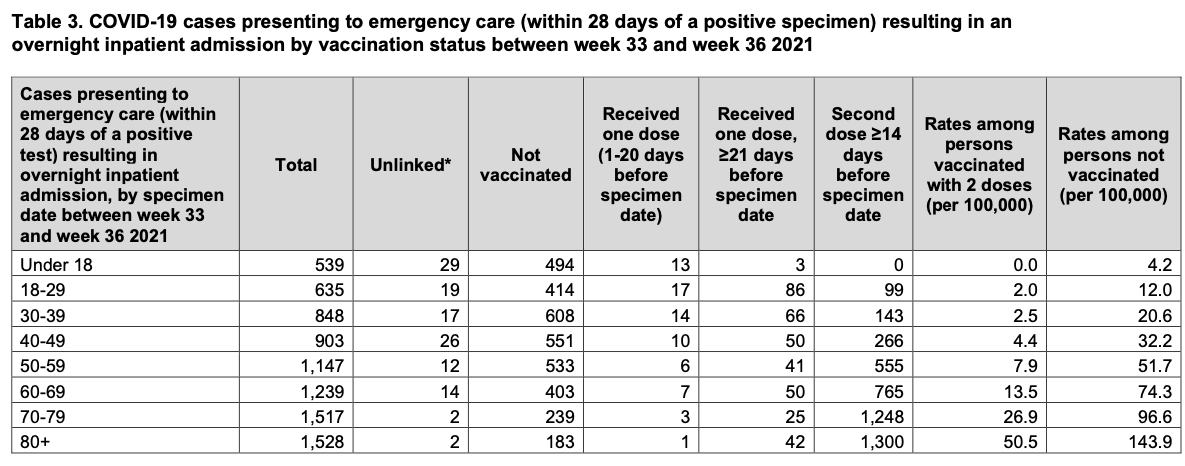
(Meanwhile, severe outcome efficacy remains quite robust.12)
At first I attributed this to mere timing. The Covid-vaccinated are simply catching up, on a per-capita level, with the unvaccinated who have been driving infection (and thereby gaining in overall immunity) all summer. As infection efficacy evaporates among the under-40s in the coming weeks, those cohorts will switch from “infection efficacy” to “falsely apparent negative infection efficacy” as well.
I no longer believe this to be the case.
It is not, however, the data in the UK and England that challenges such an ambivalent interpretation. Case rates are much higher this summer than last year: But like so much of the northeastern US, this could be attributed to the awkward timing of the (poorly measured) spring wave in 2020, which essentially made the summer a non-event.
There is no such explanation available to account for the southern US:



Again, I do not wish to make anything of the hospitalization and death rates for these regions, as so much depends on unknowable changes to standards of (mis-) treatment. The simple fact is that there a lot more apparent cases, and this can provisionally either be attributed to the virus or the pseudo-vaccines.
In fact, the same situation prevails in Israel, though triple-dosing has already thrown so much into question (additionally, Israel continues to have high positivity rates, indicating “gaps” in testing compared to the over-testing in the US):

Until recently, the appearance of a higher wave in 2021 could be provisionally attributed to a less locked-down society: The final shape of the wave in Israel, for example, would be higher, but the base less broad, resulting in the same overall volume. This possibility is out the window.
That leads us to… Forever Spike.
(For update notice on this segment, see footnotes.13)
For a more detailed, up-to-date version of the mechanism of “negative efficacy” described below, see “Neg.”

The Forever Spike Disaster!
Israel rolled out triple-dose boosters on July 31st, seemingly right before their official statistics would also have revealed a negative real-time efficacy. To revisit the capture previously examined for July (as well as the first three days of August, before any apparent change was made to categorization in light of triple-dosing):

The appearance of an intentional effort to make real-time infection efficacy invisible, just as it might have been expected to change for the worse, scarcely needs to be pointed out. Once again, per-100k rates for severe outcomes were still quite favorable in Israel throughout July. There was and still is very little explanation for Israel’s aggressive push of triple-dosing in August, beyond optics and obfuscation. At all events, it seems quite likely that the Covid-vaccinated in Israel are driving the continued growth of the summer 2021 wave, in some fashion that has been rendered very hard to make out thanks to the overnight recategorization of who is and is not “vaccinated.”
So, we sort-of have our trend. How to explain it?
Setting aside possible, magical changes to the virus itself, offering a Covid-vaccine immune response-based explanation for both negative infection efficacy (as observed in England) and higher overall case counts (as observed in the southern US), leads us full-circle to a prediction that has been forwarded by vanden Bossche for the last several months: The Covid vaccines are suppressing innate immunity.
What follows is my own version of the theory, as - once again - his version is so tied up into an ambiguous definition of “herd immunity,” that I haven’t read his recent posts very extensively.
Typically, observed outcomes to exposure to SARS-CoV-2 reveal a significant amount of “immune dark matter.” There are individuals who do not get infected despite exposure, and do not produce antibodies either (while many test-confirmed, asymptomatic infections result in the production of antibodies).
The most likely account for this dark matter is successful suppression of the virus within the respiratory tract via natural antibodies and toll-mediated immune responses, including Natural Killer Cells - this mode of natural immune protection both does not require memory immunity and, likely, does not lead to its generation. Additionally, as it appears that the virus is only detectable in the nasal cavity after a certain threshold of prior replication has been surpassed, detection of the virus in the nasal cavity corresponds to the full-on engagement of memory immunity.14
The mechanisms for “negative infection efficacy” that take this non-measurable, early suppression into account would almost certainly involve the interference of residual, post-Covid-vaccine antibodies in the upper respiratory tract. These antibodies, once they have faded below “sterilizing” levels, do not prevent egress into cells, but they do conceivably blunt the detection of the virus - or of the infected cells which are expressing viral proteins during replication - by the toll receptors of macrophages and Natural Killer Cells.
These innate immune cells, in fact, might take spike-binding IgA antibodies as an implicit “signal” that there are corresponding T Cells which should take over from here. In the wake of a normal encounter with a respiratory virus, some of the Killer T Cells which are programmed to recognize the virus later migrate into the respiratory epithelium, and remain there to guard against reinfection - these become “resident T Cells,” an under-studied element of memory immunity. Injection-based vaccination almost certainly does not lead to the same association of antibodies and tissue-resident T Cells. In this model, innate cellular immunity fails because it incorrectly defers to a non-existent memory cellular immunity.
Whatever the model, the end result is that nearly all of the “dark matter” category of encounter has been replaced by test-measurable immune responses, including symptomatic infections.
I have created a crude representation of this proposal below:15
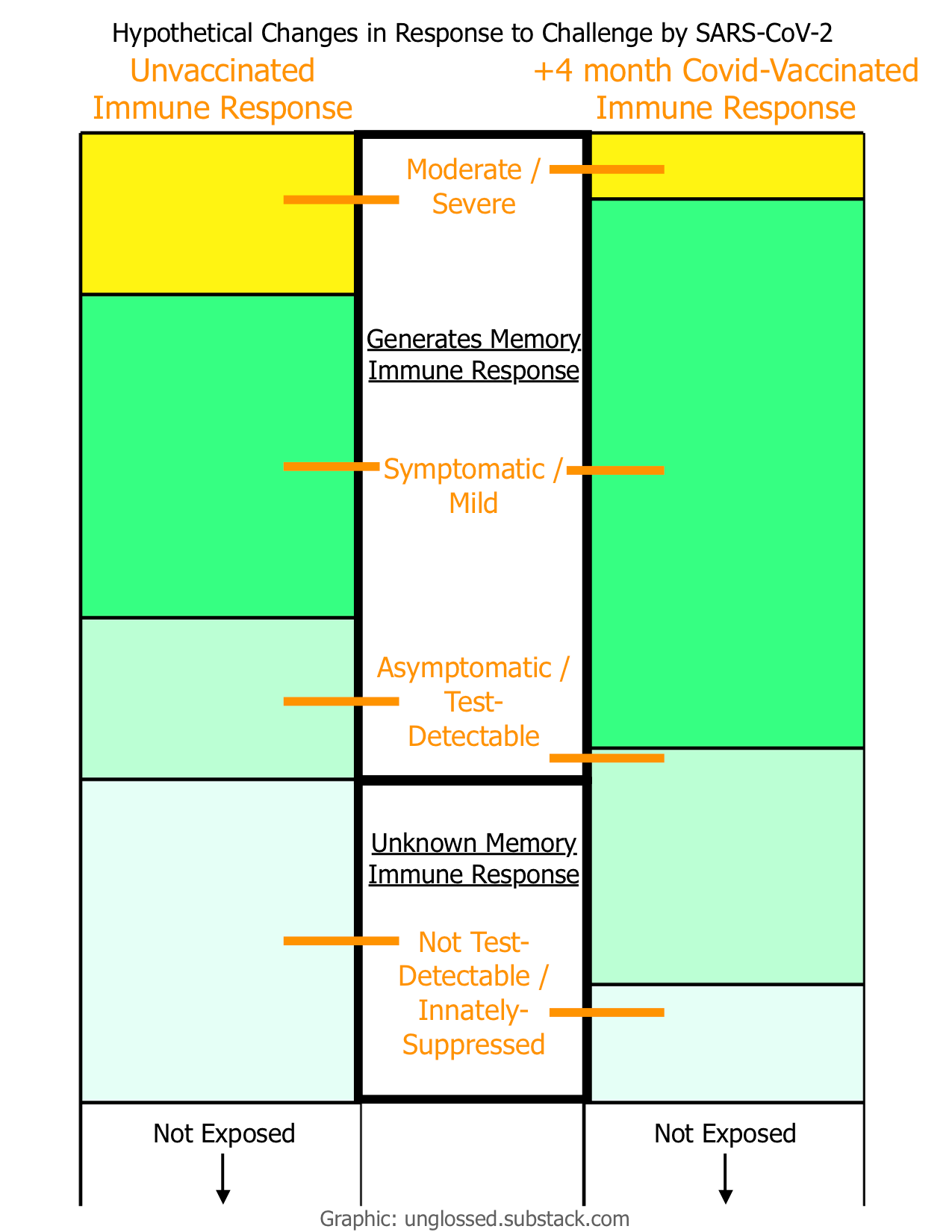
That such a phenomenon, if it were true, would explain a rise in cases is self-evident.
The question becomes, how does it affect the unvaccinated? Although the change to absolute number of all test-confirmed cases might be small, the number of non-severe cases more nearly doubles among the vaccinated in the crude representation above (and, I have likely under-represented the pool of innate suppression available to disable / convert). This could imply quite a bit more exposure for vaccinated and unvaccinated alike, leading to a cyclical effect. On the other hand, this change to immune response my wane over time; vaccine-induced antibodies may eventually “get out of the way” of the innate immune response, restoring the former status quo.
But, if Covid-vaccinated individuals are going to continue exiting the “infection efficacy window” throughout the autumn, it seems that the unvaccinated are quite likely going to have more exposure overall.
And if the Covid-vaccinated are going to perpetually repeat this cycle via six or eight month boosters, I have a hard time seeing how the result does not land at “universal wave-like levels of exposure.” In other words, Forever Spike.
Should the FDA revolt fail, or should the resort to “booster fraud” merely expand in reply to the FDA’s act of “mRNA script censorship” so that triple-dosing is virtually ubiquitous, Forever Spike will likely result. But what will be the result of Forever Spike?
Regarding infection itself, my intuition is that the unvaccinated must quickly reach a resting point, where post-infection antibodies cross the same high thresholds observed in India, and the unvaccinated essentially do not partake into the “endless wave” whose dynamics among the perpetually dosing Covid-vaccinated, including rate of antibody escape, are impossible to fathom in advance.
But a comment by user “dendroica,” at the aforementioned “superspread” post by el gato malo, has me warbled.16 I mean worried:
The hypothesis is that genetic vaccines are inducing partial immune tolerance to spike protein, likely through a regulatory T-cell response. […]
Tolerance is the collective term for a variety of mechanisms used by the human immune system to prevent autoimmunity.
The comment is actually offering a novel theory about immune response among the Covid-vaccinated: Because the mRNA script creates a pattern-association between the spike protein and native cells, there is likely some degree of tolerance generated alongside the anti-viral response. This seems plausible. Could this lead to a novel form of infection enhancement - where the immune system, essentially, becomes “selectively immunocompromised” against SARS-CoV-2? Who can say?
But the idea this theory sparked in my head was: If all seasonality is removed, and exposure to SARS-CoV-2 becomes essentially a near-daily event all year round as I supposed above, will the immune system of the unvaccinated, at a certain point, incorrectly classify SARS-CoV-2 as “self” - or, just as bad, as a common allergen, leading to IgE sensitization? Especially - to really paint a picture of a potential Forever Spike hell - if the Covid-vaccinated, all this while, are somehow expressing the spike protein directly into the air (the evidence for which is strictly anecdotal at this point)?
Or, will “relief” arrive in the form of the simultaneous application of antibody escape pressure by those entering the boosted part of the cycle, leading to more rapid antigenic drift? That would potentially take the tolerance disaster scenario off the table. But would it mean that what should have become just another seasonal “common cold” for the unvaccinated, is experienced something more like an ubiquitous immune stressor, with a depleting effect on cellular immunity that could reduce overall immune competence (meanwhile, expect the rate of severe outcomes for “breakthrough” infections to dramatically increase when the virus does achieve “mRNA script escape”)?!17
Again - Who can say.
If the super-disaster of the last two centuries of medical interventions into the immune system has taught us one thing, it is that there is always a cost for replacing the patterns of nature with a lab-made simulacrum. If the farce of the Covid vaccine roll-out has taught us one more thing, it is that we, collectively and culturally, don’t even seem to care about that cost.18 Perhaps this will teach us how.

See “Myo-Card Me a River.”
See, broadly, https://www.geertvandenbossche.org.
(index link anchor)
See el gato malo. “leaky vaccines, super-spreads, and variant acceleration.” (2021, August 17.) bad cattitude.
See “Burned All My Notebooks.”
On the other hand, this has profound implications for Measles and other vaccines. Calibration of the dormancy timers of these viruses during infections in vaccinated children is only two generations in, compared to chickens where a generation passes in a flash. This could explain the rising case rates in the 80s, which led to the addition of a second dose to school entry mandates. See “Die Herd.” Since Measles does not seem to edit glycoproteins to a great extent, however, this is more plausibly another mucosal / humoral distinction-based vaccine immune-response deficiency. Nonetheless, a Marek’s effect for Measles which would affect unvaccinated children could already be underway.
(index link anchor)
See el gato malo. “the vaccinated superspread hypothesis.” (2021, September 16.) bad cattitude.
A good write-up, which argues for why looking at the real-time value is more important than using a prematurely-derived “long term rate,” is at Jones, Will. “Vaccines Have NEGATIVE Effectiveness in the Over-40s, as Low as MINUS 38%, Shows New PHE Report.” (2021, September 10.) Daily Sceptic.
Here is chart from the same report for “real-time hospitalization rates.” For my discussion on “Covid vaccine immune response” which offers my theory for why severe outcome efficacy is durable, see “Boostermania!”:
October 29, 2021: This segment was edited to add a more nuanced proposal for the mechanism of residual antibody interference. The original version is below:
Thus, the simplest account for “negative infection efficacy” is that innate response is disabled by the interference of residual antibodies. These antibodies do not prevent egress into cells, but they do blunt the detection of the virus by the toll receptors of macrophages and Natural Killer Cells. The simple result is that nearly all of the “dark matter” category of encounter has been replaced by test-measurable immune responses, including symptomatic infections.
It also occurs to me that there could be an issue with the “back-up” innate immune response - the inflammatory signaling that recruits other macrophages etc. to the site of trouble - somehow being cross-wired with residual signaling pathways from the Covid-vaccines. These signals could lead to other parts of the body, so that recruited macrophages go to where spike was found before, instead of where it is now. However, I don’t think such a mechanism is as compatible with the “non-measurable immune suppression” that I am suggesting has been disabled.
As implied in the comparative swab-site study reviewed in “Travels to Maskladesh.”
This is not to be confused with the question of how the Covid vaccines might impact the other “innate” form of immunity to SARS-CoV-2, T Cell recognition based on prior exposure to coronaviruses. Implicitly, this prior recognition is measurable: The reason we can perceive it, is because IgG antibodies to the N protein and spike protein are found to rise before IgM antibodies during challenge with SARS-CoV-2 in some ostensibly “naive” individuals (otherwise, the mere identification of T Cells for coronaviruses would tell us nothing on its own). This memory-based “innate” immunity still results in test-measurable outcomes (whether by antibody assay or PCR test). It therefor does not belong in the “dark matter” of exposure without infection or test-measurable memory immunity generation.
Further, Covid-vaccination does not appear to have made any negative impact on measurable, memory-based immunity so far, as most recently suggested by the bombshell reinfection study by Gazit, S. et al. “Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections.” medrxiv.org.
An impairment to memory-based, post-infection natural immunity may reveal itself in the long term; additionally, Covid vaccines may turn out to have detrimental effects on memory-based immunity to other viruses (as already suggested by the association of shingles with Covid vaccination, though there are other possible mechanisms for this anomaly). But in accounting for the larger summer wave in 2021, erosion of infection-based memory immunity does not seem to be a plausible culprit; there simply aren’t enough apparent reinfections. Therefor, the disabling of innate, “dark matter” suppression of the virus by natural antibodies and Natural Killer Cells is the more likely explanation.
(el gato malo. “the vaccinated superspread hypothesis.”) (Comments.)
Regarding a hypothetical scenario where vaccine-altered rates of antigenic drift / shift could raise the danger of antibody-dependent enhancement, I believe this will almost certainly be a concern for the vaccinated (based on many of the previous failures with coronavirus vaccines), but that the (infected, recovered) unvaccinated will not face the same danger. As observed with Dengue Virus, direct introduction to an antigen in the blood seems to be critical to priming the IgE-mediated antibody dependent enhancement threat posed by coronavirus vaccines.
Observe, in particular, that while coronavirus vaccines have failed in trials for years, signs have been emerging all around of the unraveling of the benefits of traditional vaccines on a societal scale - hinting at an ongoing and worsening plague of unintended consequences. So what could possibly make the medical establishment think that a vaccine of the type that routinely fails in limited trials would not have even worse societal consequences?
Actually, nothing. It seems all the more plausible that the intention - one which even physicians not directly involved in the expert apparatus that directed this effort seem to intuit as desirable, based on the outputs of “science journalism” - was to unleash the worst type of vaccine possible into society, before the plague of unintended consequences for traditional vaccines could no longer be widely suppressed.
Thanks for sharing these, and I'm pleasantly surprised to see my hypothesis incorporated into your thinking. My thought is that if the genetic vaccines truly are inducing negative efficacy via immune tolerance, the consequences for the vaccinated will become disastrously obvious at some point and the responsible vaccines will disappear from use in a giant scandal - and perhaps will be replaced by Novavax-type or even inactivated-virus vaccines. Tolerance will presumably fade eventually, so I don't think it will truly be a "forever spike" situation inducing tolerance in unvaccinated people.
If the superspreader hypothesis is real, the vaxxed/unvaxxed illness/death differential should disappear once a majority of unvaxxed have natural immunity. At that point (probably sometime in the next few months in the US) we will see whether the differential reverses which would indicate tolerance/immune suppression, original antigenic sin, antibody-dependent enhancement, or some other issue specific to the vaccines.
I won't be 100% convinced of negative-efficacy data until I see a chart that separates unvaccinated-naive from unvaccinated-prior-immunity people. It seems like people with prior immunity would self-select into the unvaccinated group, and given that we know natural immunity is superior that alone could lead to lower infection levels in that group.
I like your graphic - that is about what I would expect from immune tolerance. I'm also interested in understanding the degree to which induced tolerance might be protective against severe illness due to immune dysfunction/overreaction - in which case it might appear superficially as a feature rather than a bug.
I've never been convinced by the Marek's disaster scenario. For one, it is much more of an exception than a rule - much as was true of smallpox in terms of being eradicable through vaccination. For another, there are many important factors that are true of Marek's in chickens that are not true of SARS-CoV2 in humans. Below is a response I recently posted to another forum on this issue.
-------------
Although I'm certainly not an expert on the level of Geert Vanden Bossche, I find the Marek's scenario unlikely for several reasons.
1. Natural immunity is superior to vaccine immunity, and we are rapidly reaching a point at which a majority of unvaccinated people have natural immunity. This is in contrast to the situation in chickens, in which the entire population turns over on average several times per year and so there is a constant influx of disease-naive birds and natural immunity plays a smaller role.
2. The concern is that a vaccine that reduces symptoms without blocking infection could select for more virulent strains that are capable of causing symptoms in vaccinated people - but that then are deadly to unvaccinated people. This is more likely if symptoms are required for spread - e.g. a virus that spreads through lesions or pustules. In the case of covid, which spreads through breathing and talking, suppression of symptoms may actually increase transmission as asymptomatic people are more likely to be out and about. So there should not be much selection for more virulent strains among vaccinated people.
3. The selective pressure for respiratory viruses to become endemic through increased transmissibility and decreased virulence over time is very strong, and while vaccination may interfere with this trajectory in harmful ways I would not expect it to destroy it entirely. Natural immunity against coronaviruses and influenza viruses is also "leaky" and of limited duration, and so leaky vaccination is not so much a special case as an inferior version of natural immunity. I would be much more concerned about a Marek's scenario if we had a leaky vaccine against Ebola, polio, or smallpox - diseases with a naturally high virulence and for which natural immunity is typically sterilizing (non-leaky) and lifelong.
4. We have been vaccinating with leaky flu vaccines for years without creating new lethal strains, and SARS-CoV2 is much more similar to influenza than to the carcinogenic herpes virus that causes Marek's in chickens.
5. Vaccine efficacy is rapidly waning to the point at which they are not merely "leaky" but might better be called "ineffective against everything except severe illness." In this circumstance there should be little if any selective pressure for increased virulence among vaccinated people. The primary selective pressure will be for evasion of vaccine-induced neutralizing antibodies, and these antibody-escape mutants should not in general cause more severe illness in unvaccinated people. (Although if leaky vaccines increase the total amount of virus in circulation, they will increase the overall mutation rate, which could lead to new strains emerging more frequently and potentially causing more frequent reinfection among both vaccinated and unvaccinated people. This is a problem but not on the level of Marek's.)
6. The Marek's scenario unfolded relatively slowly. It was not so much that the vaccines selected *for* hotter (more virulent) strains but rather that they failed to select *against* them. Because the vaccines suppressed symptoms, strains that would have been eliminated in unvaccinated populations because they killed birds too quickly were allowed to evolve and persist if they also increased transmissibility even slightly. Thus Marek's disease gradually became more deadly to unvaccinated birds over several decades of widespread leaky vaccination. So even if widespread leaky vaccination against influenza or SARS-Cov2 does have the effect of increasing virulence, I would expect this to occur over a years-to-decades timescale - whereas many of the other crisis scenarios we have been discussing could easily unfold over the next few months.
Many thanks for such an informative post. I was wondering how the four hypotheses would affect different age groups.