Sorting out the “blame” for increased spike protein innovation. Plus: Forever Spike vindication, revisiting pregnancy risks from infection, and metal floaty bits.
While accrediting Geert vanden Bossche with promoting the theory that the Covid vaccines would disable the “dark matter” of innate immunity - individuals who, previously, could be exposed to SARS-CoV-2 without any test-measurable outcome, implying suppression of the virus by natural antibodies and Natural Killer Cells - I was careful to emphasize that I was voicing my version of his argument, and not purporting to speak for his.
This caveat has proven itself unnecessary. In yesterday’s dual interview with Robert Malone, vanden Bossche not only portrayed his innate immunity argument for himself, but affirmed that he interprets the current data from Israel and the UK to vindicate his argument. He goes further, to affirm that he expects that future case patterns will take the form of a constant plateau of semi-wave case levels - i.e., exactly what I characterized in my “Forever Spike” theory. My words:
And if the Covid-vaccinated are going to perpetually repeat this cycle via six or eight month boosters, I have a hard time seeing how the result does not land at “universal wave-like levels of exposure.” In other words, Forever Spike.
I expect yesterday’s interview will be taken down by Youtube in short order. I will update this post if a rumble or other version becomes available. In the meantime, the relevant discussion begins circa 27:45. (Edit, 09/27: Because I watched the video in a mixed up order, I mis-remembered the level of detail of vanden Bossche’s remarks at 27:45. For a much more thorough discussion of the disablement of innate immunity, see his remarks beginning at 1:30:00. Additionally, on second watch, it is a bit unclear in the linked portion when he is referring to the level of infection and the “pressure” on infection; so, I hereby partially restore my caveat as regards the Forever Spike topic.)
I continue to make no claim to understand what vanden Bossche means when he wades into discussions of “herd immunity,” however.
To highlight the ideas of another eccentric researcher who has been the target of censorship, I have recently been made aware of the brilliant work of J.J. Couey. Among all the credentialed Covid vaccine skeptics, Couey is the most sincerely faithful in natural immunity, vitriolic regarding our idiotic attempt to surpass it, and watchable in his willingness to get into the ring with our fraudulent expert overlords via picture-in-picture takedowns.
I have yet to go through his back catalog, but his most recent two videos are worth highlighting and discussing. On Tuesday, Couey debuted a theory that the SARS-CoV-2 spike protein was lab-designed to promote the creation of a Swiss army-knife anti-spike antibody against coronaviruses.
This design would have occurred in the context of vaccinology’s long-laboring, then still-fruitless obsession with using one virus as a vector to produce immunity to another one.3 But as opposed to using the coronavirus that would be SARS-CoV-2 as a self-spreading vector for another anti-viral vaccine, Couey suggests the designers intended SARS-CoV-2 to operate as a vector for itself. That this would somehow create lifelong sterilizing immunity is total scientific nonsense - which is why it is exactly the kind of thing vaccine researchers might try. The relevant description begins at 59:00 [link expired by twitch]; it is followed by a superb explanation of the futility of trying to control the virus’s spread.
While Couey’s description of the intention behind the spike protein’s design is excellent, I wasn’t initially convinced that the actual outcome - i.e., the virus - might have matched the intention. However, his stream yesterday provides a compelling case. It has also made me rethink my assurance that the Covid vaccines have not placed any significant escape pressure on the virus.
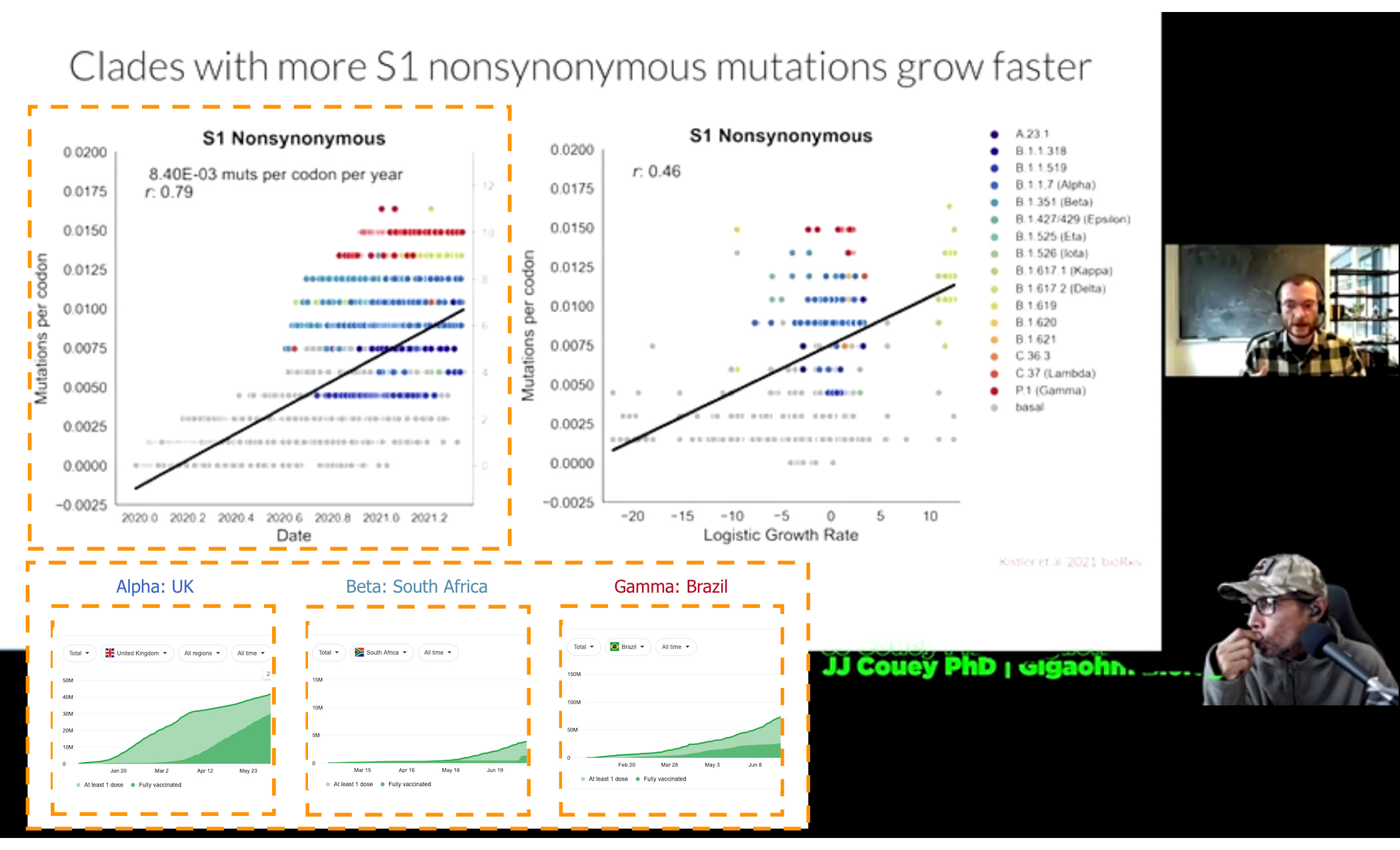
In this session, Couey wages a picture-in-picture battle with Trevor Bedford, the data torturer responsible for Nextstrain, who has just delivered a webcam thesis to explain the sudden increase in mutations of SARS-CoV-2 beginning last winter. The core content begins circa 12:00 (link expired). It is better watched than summarized, but in short, Bedford proposes that the reason SARS-CoV-2 began to mutate the spike protein much more aggressively beginning in October, is that it was confronted with a wave of naturally immune in the UK, Brazil, and South Africa - regions where spring and summer waves were significant. The most relevant graphic is the highlighted portion below (with Couey’s intense glare left in for flavor). I have added case rates for Brazil and South Africa, which show the wave pattern despite significant “under-testing;” and the hospitalization rate for the UK, as testing was not in place during the spring wave:
Click Image to Expand
So, Bedford’s thesis - that the critical change which promoted a diversion from the virus’s former stability, leading to a sudden pile-up of dots above the trend line, was natural immunity - has a glaring problem, before we even get to his unwillingness to say the word “vaccination” once throughout the entire video: If the first UK wave was in the spring, why didn’t the naturally immune begin to exert selection pressure on SARS-CoV-2 much faster than in South Africa or Brazil, which were not hit until the summer? And, for that matter, why did no “variant of concern” emerge in New York and the rest of New England, which also had spring waves? There is no answer, and Bedford’s thesis, barring the convergence of a million different invisible flapping butterfly wings, is nonsense.
But Couey loses me a bit, in his counter-attack. To Couey, it is self-evident that the sudden surge in spike mutation is an indictment of the Covid vaccines, which were undergoing trials in the UK already. This seems like a perilous argument, given how yet-to-arrive widespread adoption was for all three countries:
Additionally, neither of these theories seems like a good match for Delta’s emergence in India. And although Delta is in some respects less novel in the spike protein structure than the variants it has displaced, it has had no trouble thriving in regions with high vaccine uptake.
Additionally, Couey argues that the (post-infection) naturally immune do not place any pressure on the spike protein specifically. Rather, T Cell immunity heavily favors other viral assembly proteins that would be prevalent on the membranes of cells infected with SARS-CoV-2, presenting a broad spectrum of escape pressure that is too difficult for the virus to escape. This may be true, but such protection would seem irrelevant to the consideration of cellular entry, which is enhanced by one thing above all else - mucosal antibodies against the spike protein. It’s difficult to see how T Cell immunity influences escape pressure on the virus (see Edit, below, for more discussion).
Couey, however, cements his argument in his analysis of Bedford’s own presentation. The fact that the current rate of mutation of the spike protein has exceeded the flu, and the suggestion that just a handful of healthcare workers could drive enough gain-of-function pressure on the spike to accelerate mutation by several months, are thought-provoking.
I have given the question of whether the naturally (post-infection) immune place pressure on the spike protein additional thought. As I, of course, have advocated a grand unifying immunity theory which posits, in part, that antibody-based immunity is meant to wane to allow for asymptomatic (but spread-capable) or mildly symptomatic re-infection after a cellular immunity resting period, both to avoid placing immune-escape pressure on the virus and to keep memory immunity up-to-date as the virus is edited by the “herd” at large, the intuitive answer is no. Natural, post-infection immunity is a binary between “sterilizing” and “inviting,” there is no uncanny valley of gain-of-function like semi-protection.
However, I still think the current evidence is that the Covid vaccines are almost the same. The only change is that the “sterilizing” state - which, of course, evaporates after four months - appears to be much more inconsistent.5
This leaves me even more “thought-provoked” by Couey’s proposal that early trial recipients turned into walking gain-of-function labs. Regarding my dismissal of the Escape Mutant Disaster theory, the bullets are indeed whizzing. Yet even if the bailey is swarmed, I still have the motte: India.
Where I still differ with Couey is in his insistence that T Cell immunity is the key distinction between natural and synthetic immunity. T Cell immunity, I argue, does not prevent (asymptomatic or mild) reinfection after antibody fade-out for a simple reason: It is not robust enough to survive a high viral load challenge, such as might be encountered during a winter wave. The central tenet of the first Immune Equilibrium argument, after all, is an axiom: The immune system cannot be competent at discouraging immune escape, unless it is competent at allowing for future spread. This implies a baseline permissiveness to T Cell immunity. It prevents small flares, but not a concentrated attack. It is a buffer, not a wall.
For the Covid-vaccinated, again, the issue is that the would-be temporary wall - mucosal immunity - is improperly built, as a natural result of the futility of trying to immunize for a respiratory virus by placing an antigen into the shoulder and bloodstream. So it is both “leaky” in the early stages (implying the Escape Mutant theory is back on the table) and disruptive to innate immunity in the later stages (to round back to the Forever Spike theory). The Covid-vaccinated do not have a functioning “buffer” against small flares, whether innate or memory-based.
Compared to deficiencies in mucosal immunity, deficiencies in T Cell immunity are not likely to be instrumental from the perspective of evolutionary pressure on the virus.
I have also recently become aware of a certain Rhonda Patrick, a “vaccine misinformation debunker” who seems more knowledgeable and formidable than the average for the type. But, continuing the theme of this post, Patrick’s output is entirely in video / audio form - including a lengthy Joe Rogan interview.7
If any subscribers are aware of a site where some of Patrick’s arguments are already converted to text, I would appreciate the link. TYIA.
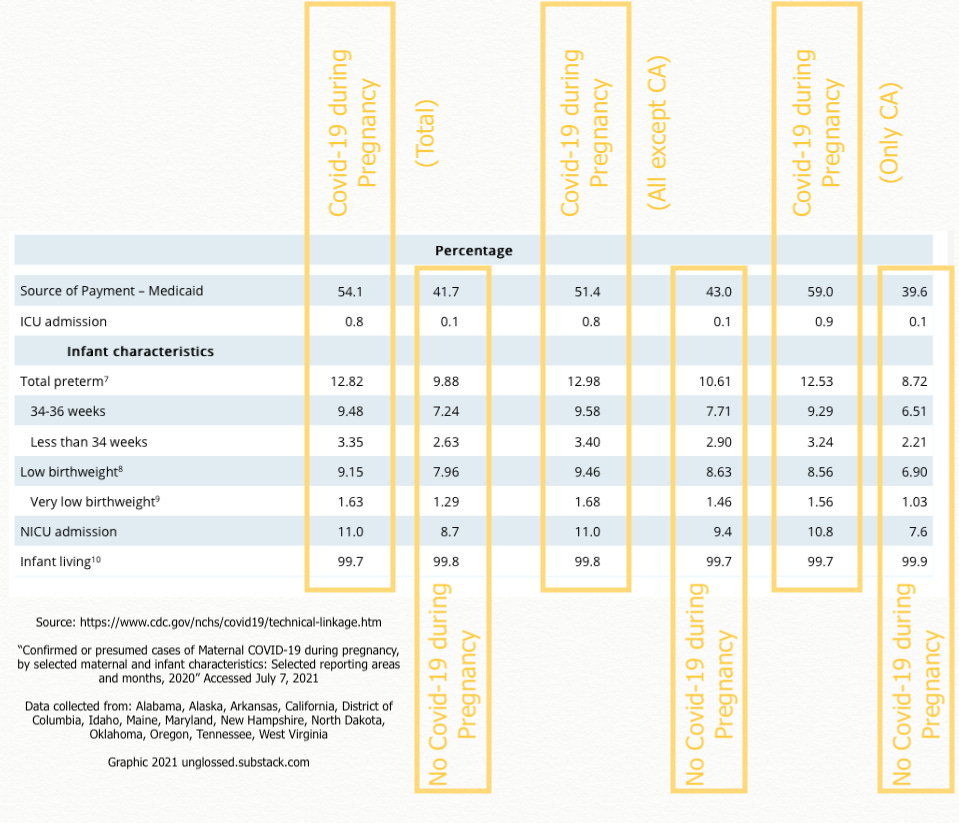
As my previous attempts to address the risk / benefit proposal for pregnant women who might be considering the Covid vaccine are split between two separate posts, I thought I would take the opportunity to present the current, streamlined version of the text-snippet which I use when addressing comments on the subject elsewhere. Readers familiar with my older posts may find the following redundant. With the addition of the previously-posted mark-up the CDC’s table:
If it helps, here's the CDC's compiled data indicating the minimal, almost statistically nonexistent impact on outcomes from infection with SARS-CoV-2 during pregnancy in 2020:
See table III, ICU admission and Infant Characteristics at the bottom. Note that higher medicaid percentage for "Yes Covid-19" cohort indicating an income disparity.
Very little increase in negative outcomes associated with infection; and it may all be a reflection of lower income anyway.
This is as should be expected - there is no way to avoid the risk of viral challenge of some kind during pregnancy. That doesn't mean it is safe to get sick - it means that getting sick with one thing is the same as getting sick with something else. Targeting SARS-CoV-2 likely does nothing to make pregnancy safer in terms of general risk of viral complication.
Regarding Covid vaccination, the data on "normal (first 20 weeks) miscarriage risk window" is ok so far, the data on "aberrant post-20-weeks maladies" is not in (https://www.researchsquare.com/article/rs-798175/v1).
But perhaps anecdotes speak louder than statistics, when it comes to a subject this sensitive. And since the news has been weaponizing outlier cases of infection during pregnancy, a look at counter-anecdotes is appropriate:
5. Metallic contaminant theories go semi-mainstream!
Rumors of metallic contaminants in the Covid vaccines - as well as graphene oxide - have spent the last several months the sole province of HighWire video comment rants and the perpetually provocative, but often-vindicated Stew Peters.
As of four days ago, these concerns have escalated to the realm of rebellious European lawyers, doctors, and researchers involved in or associated with Corona Ausschuss, who arranged a presentation highlighting nearly a hundred alarming autopsy slides and light microscope video footage. Take it for what you will.
Promised ADE post to arrive soon. Thanks for subscribing to Unglossed!
Perhaps the only successful achievement of this dream is the smallpox vaccine, which itself is the reason why the word at the center of the largest controversy in human history essentially means “cow-ine,” even though it actually appears more related to horsepox than to cowpox, as I so habitually take to the footnotes to point out.
Rhonda doesn't seem to write much. She is fairly prolific in videos and has a lot of good insights, including at her own site at foundmyfitness. Maybe we can talk her into starting a substack.






Lab leak or natural mutation?
Rhonda doesn't seem to write much. She is fairly prolific in videos and has a lot of good insights, including at her own site at foundmyfitness. Maybe we can talk her into starting a substack.