


The 60 Day RNA Mystery, Pt 1
Covid vaccine mRNA and spike linger for up to 60 days after the 2nd dose.

The following is a brief walk-through of the germinal center findings by Röltgen, et al., and review of why the findings are alarming.
Part 2 will piece together the puzzle to discover the possible “non-alarming” explanation for those findings.
If you just want the highlights, head to Spoiler / Summary.

Though posted in January, it was last month that the paper by Röltgen, et al. made a splash. 1
We have previously examined the rather reassuring (though represented as otherwise) results pertaining to immune response after “breakthrough” infection,2 but the “splash” in question was generated by the far more alarming findings that in a sample of Covid vaccine recipients, both spike protein and Covid vaccine mRNA were still detectable in lymph nodes up to 60 days after the 2nd dose.
Supposedly, such a finding shouldn’t even be possible. In fact it isn’t very surprising.
The Pre-set-up: Germinal Centers and Antibody Response
When the immune system is busy creating what we classically define as a novel memory immunity response, with the long-lasting B Cells and the IgG and IgA antibodies and all that, the action mostly takes place in “Secondary Lymphoid Organs” (SLOs) - our lymph nodes, spleen, or myriad specialized accessory structures in the respiratory and gastrointestinal tracts.
In these, B Cells move into “follicles” (which would be better described as “nodes,” though that would be confusing, but that’s what they are - nodes of cells that resemble thumbprints in a tissue slide) where they compete over multiple generations to produce the most well-honed receptors for a target antigen which is attached for the entire time to a bunch of other cells called bla bla blas, and with another bunch of other cells called bla bla blas selecting the best designs for further enrichment (simplification). SLOs including lymph nodes have multiple of these follicles, but in lymph nodes they are more prevalent and highly-ordered when actively crafting a new B Cell response. Whatever the Secondary Lymphoid Organ, “germinal center” is the name for a follicle that is active in this manner.
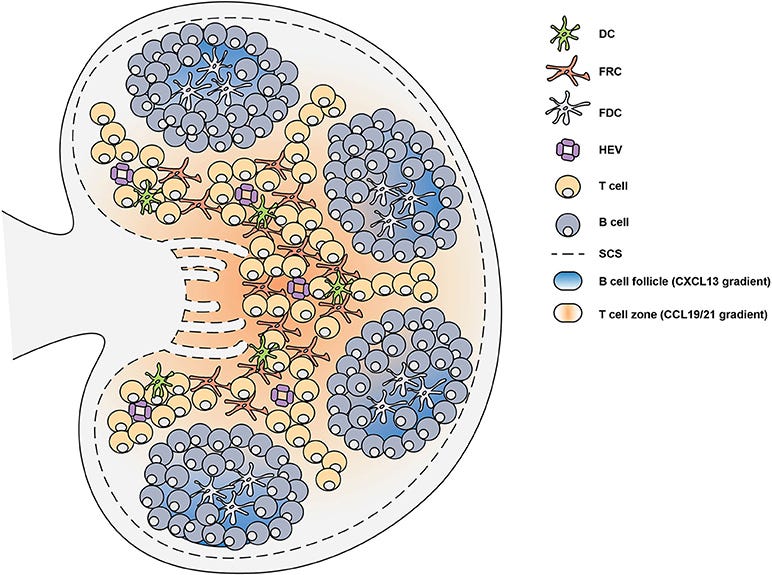
The long-lasting lineage of memory B Cells which later, throughout life, can expand (multiply) and express loads of previously-honed antibodies, all worked out their specific antibody design in a germinal center in one or the other of the Secondary Lymphoid Organs of your body.
Röltgen, et al. noticed that Pfizer / BioNTech Covid vaccine recipients (with no infection with SARS-CoV-2) made antibodies that bound really well to the Receptor Binding Domains of multiple variants, more-so than antibodies after very early natural infections, even though the spike proteins for those early infections should be… exactly the same as for the injections.
They thought this was interesting (it is). Why was the Pfizer Covid vaccine “front-loading” a cross-reactive immune response to what essentially ended up being “future” variant spike designs? We can leave this question aside for now, as they don’t really find an answer for it (a later essay may address the issue).3
All that matters is that they wanted to look for clues about the antibody responses after mRNA Covid vaccination, and antibody responses get their start in germinal centers, and so they looked in the germinal centers of people who had either been infected or recently Covid-vaccinated. Except that for the latter, “recent” wasn’t really very recent in every case.
There was a reason for this.
The Set-up
Since there is currently no standard practice for examining intact germinal centers in living subjects for immunology research, the authors looked for core needle biopsy samples that had been coincidentally performed after receipt of an mRNA Covid Vaccine.4 They landed on biopsies which followed mammograms or related referrals at Stanford Medicine for seven recently Covid-vaccinated women, and which had taken place on the same side of the body as the injection.
These samples were core needle biopsies of “axillary” lymph nodes, located under the armpit, which are both the first place breast cancer cells are expected to be found if metastasis is underway, and where germinal centers resulting from an injection into the shoulder could be expected to appear. The authors were only interested in the latter.
Core needle biopsy results in a thin (1/16 inch) sliver of tissue which is typically longer than the lymph node being sampled, and includes nearby fat tissue. If positive for cancer, normal lymph structure is also replaced by cancer tissue. In cases where multiple samples of the same lymph node are taken, only one might target the area where follicles and germinal centers reside (cortex region); and typically only one lymph node will be sampled for staging (determining the current stage) of a breast cancer diagnosis.
So, this might all sound like the authors were searching for needles in a (tiny handful of a) haystack. However, since follicles multiply during active immune response, the chances of a positive hit were not bad.5 In fact, there were multiple intact and active germinal centers in many samples in which to look for Covid vaccine mRNA or for presence of the spike protein it encodes.
The problem was that there were so few haystacks.
Only about three of the donor samples were within the first three weeks after the 2nd dose of an mRNA Covid vaccine, and so the authors also included about four additional samples from other donors that were 37 to 60 days post 2nd-dose (it’s not clear which two samples were the same number of days post-dose).6
And that is what resulted in their alarming discovery: When they tested these not-so-recent biopsy samples for Covid-vaccine mRNA and spike, they were ostensibly looking at samples that shouldn’t still have Covid-vaccine mRNA or spike in them, per the guarantees offered by authorities promoting these injections left and right - and yet, they found Covid-vaccine mRNA and spike.
The infamous graph, with annotations:
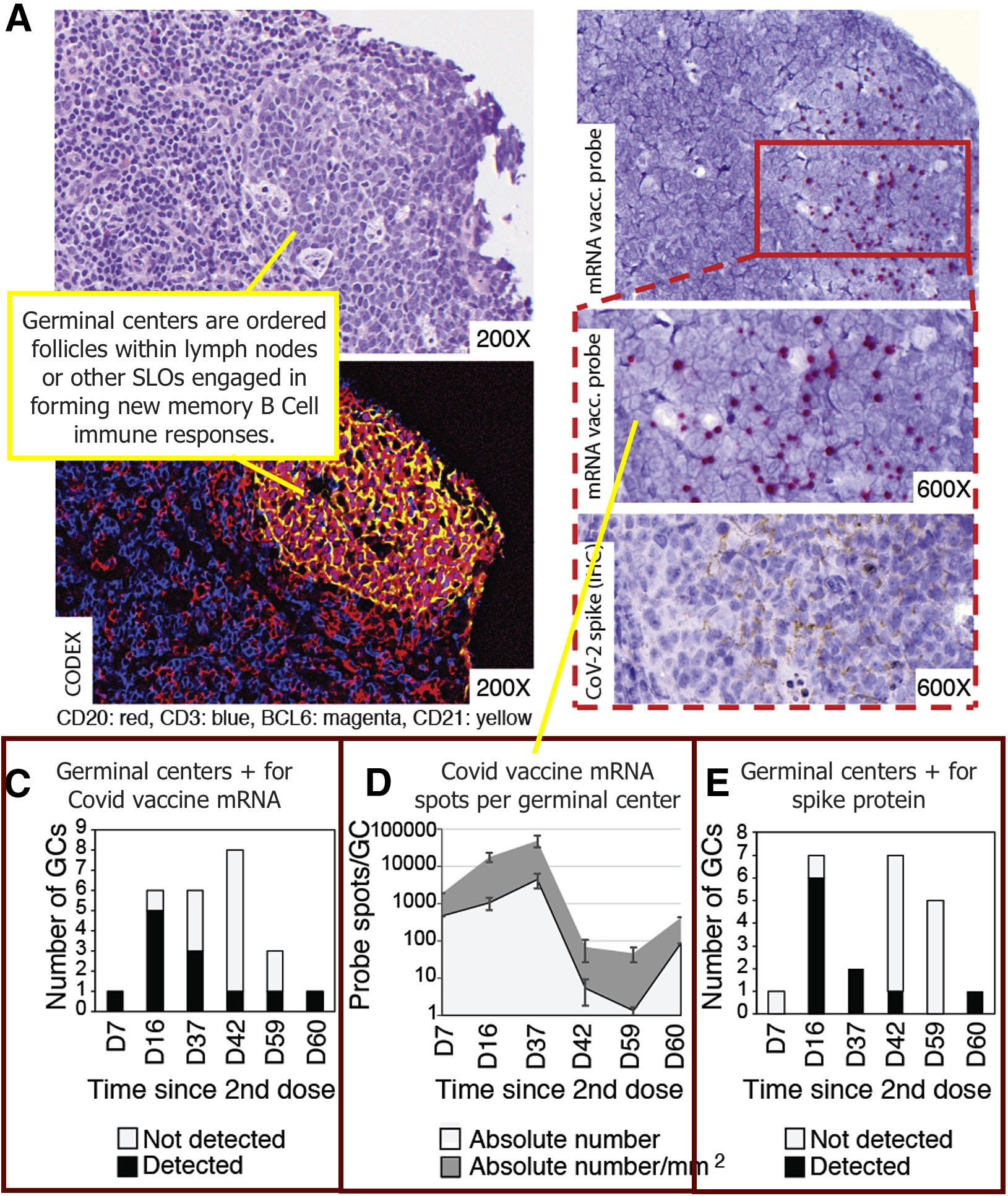
So the impression that donor immune responses are being tracked through time, here, is misleading. There were only seven different donors, who likely only contributed one or two samples from the same lymph node, and likely only on one given day-since-2nd-dose. It is not clear which day-since-2nd dose time-point has two different donors, since any sample can have any number of germinal centers. It’s also not clear why the total “Number of GCs” would be different for C and E on some days, unless there were some unclear results that the authors excluded for both the mRNA probe and spike stain tallies. I have not been able to find the relevant raw data to explain this discrepancy anywhere in the paper.7
So when examining the “roller-coaster” effect at the end, the fact that these were different samples from different donors, and that no sample might actually reflect overall prevalence of Covid vaccine product in a sampled (or nearby non-sampled, or distant) germinal centers, should be kept in mind. It’s a very messy signal. All that matters as far as the “mystery,” is that spike and mRNA are still being observed at all.
To finish with our overview of the set-up: The authors compared these samples with peribronchial lymph nodes for seven individuals who died during infection (which is centered in the respiratory tract, not the shoulder). Nothing was complicated or interesting about the collection of these samples, since they were retrieved from autopsies.
Both the Covid vaccine lymph nodes and the infection lymph nodes had controls. Three core needle biopsies of unvaccinated women served as controls for Covid-vaccinated samples; three autopsy-collected thoracic lymph nodes for pneumonia-associated deaths occurring before 2020 served as controls for the infection lymph nodes. None of the unvaccinated samples were positive for vaccine mRNA, and presumably not for spike protein or N protein (the text is unclear here8). And so the authors (presumably) do not seem to be showing us any false positives in the results.
Meanwhile, the Covid vaccine mRNA probes were tested on tissues collected during infection to validate specificity (no false positives from the virus), suggesting that the mRNA positives in germinal centers were not the result of infection.9 Additionally, the authors suggest that non-germinal center lymph zones effectively act as a negative control in all findings, which is reasonable. So, it seems safe to trust these findings do, indeed, indicate persistent Covid vaccine mRNA and spike.
(The observations for the natural SARS-CoV-2 infection germinal centers are interesting, but not relevant to the “mystery” of what is going on with the Covid-vaccinated.)
The authors conclude:
Histological analysis of draining [lymph nodes] shows […] higher quantities, and persistence of spike antigen accumulated in the [lymph node germinal centers] of mRNA vaccinees [compared to fatal natural infections] and detectable vaccine RNA in [vaccinee germinal centers] for up to 2 months post-second dose.
The Mystery
These lingering elements dramatically refute the promises that were made regarding the experimental products that no one waited to finish any experiments on before promising things about them.
As anti-vax-debunker extraordinaire, David “If you time-travelled me back to 1960, I would prescribe my own future mother Thalidomide” Gorski put it a year ago,10
In regular aqueous solution (in this case, water with some buffer and salt) RNA rapidly degrades at room temperature (or even in the refrigerator) and can degrade too quickly even at -20°C. The second, and more important, reason is that mRNA has a short half-life in cells, normally on the order of hours or even minutes. (I used to measure mRNA half-life for the gene I cloned back in the 1990s, and it was regulated by stimuli that dramatically shortened or lengthened its half-life in the cell from four hours to around an hour hour.11) Basically, the modification of the RNA in both vaccines is designed to make them more stable, but not infinitely stable, which is what Mikovits and Mercola are claiming. No biological molecule, modified or not, lasts forever,12 which is what the RNA would have to do to “turn your body into a viral protein factory, thus keeping antibody production activated on a continual basis with no ability to shut down”. Seriously, does Mercola know anything about molecular biology? Indeed, from Moderna, for example:
The delivered mRNA does not enter the cell nucleus or interact with the genome, is nonreplicating, and is expressed transiently. The estimated half-life for mRNA after injection is approximately 8 to 10 hours, before degradation by native RNases in the body, but the duration of effect also depends on the half-life of the expressed protein, which persists in the body for several days.[…]13
Basically, with a half-life of ten hours, the mRNA will be completely gone within a few days and the protein completely gone after, at most, a few weeks. The Pfizer mRNA vaccine is similar. Again, does Mercola understand anything about basic molecular biology? Apparently not, or he’s lying.
Or a really good fortune-teller.
Continued in Part 2…

The post-breakthrough-infection immune response findings were reviewed in “Even-Steven” (whereas the authors claim their findings showed OAS, their findings actually totally refute OAS - as expected, since OAS is not real).
They suggest that their observations of “slow delivery” of antigen are the explanation. The existing research support for this is ambivalent. I think it is more likely that either 1) injection results in over-involvement of the spleen in B Cell enrichment, with a resulting higher level of what might in normal infection be the “minority report” of B Cell response, resulting in higher humoral B Cell Receptor polyclonalism, or 2) the heavily modified mRNA in the injections results in poly-phenotypic spike expression (i.e., mutant spike) or more inconsistent Antigen Presenting Cell peptide selection. Again, this may be more extensively discussed in a later entry.
Lymph nodes, or the cells within them, cannot be put back into the body once removed. Lymph node biopsies are thus common in cancer care, but not conventionally used during immunology research. However, this is changing, as interest in the relationship between germinal center function over time and “goodness of antibodies” continues to grow, especially within HIV vaccine research.
However, most of the progress so far has been made with Fine Needle Aspiration - either in animal studies, or in one preliminary, “proof of concept” study on humans (Havenar-Daughton, C. et al. (2020.) “Normal human lymph node T follicular helper cells and germinal center B cells accessed via fine needle aspirations.” J Immunol Methods. 2020 Apr; 479: 112746.).
FNA essentially destroys the structure of Germinal Centers, essentially “liquifying” the sample so that cells are all mixed up, as in blood. However, examining the cellular soup for the specific markers that correspond to Follicular Helper T Cells allows researchers to infer germinal center activity.
Röltgen, et al. wanted to preserve structure (since structure was easily observable in the SARS-CoV-2 infected and pneumonia control autopsy samples), so FNA wasn’t the suitable choice per this design. Thus, they used core needle biopsies (even though fine needle biopsies may have been available for the same patients, depending on the procedures at Stanford Medicine). Had the authors been purely interested in “mRNA/spike in lymph nodes yes/no,” choosing FNA samples might have been the better choice (depending on the quality of available samples and whether the procedure is used at Stanford Medicine), allowing for a larger or less spread-out sample.
How much lymph node cortex tissue, and how many lymph nodes per patient, would also depend on the procedures used; however, as core needle biopsies usually take out a sample that is longer than the lymph node (and includes nearby fatty tissue), and doesn’t reward multiple runs through the cortex in cancer screening (as does FNA), there’s less variability in both method and result.
Specifically, from Methods:
Axillary LN core biopsies and post-mortem peribronchial LN tissues
To analyze and compare GC architecture in response to COVID-19 vaccination […] we collected axillary LN core needle biopsies from BNT162b2 or mRNA-1273 vaccinees […] For the selection of vaccinee tissues, we performed a retrospective search of our pathology archives and medical records between January 2021 and June 2021 for female patients who received either mRNA-1273 or BNT162b2 vaccination and subsequently underwent an ipsilateral [same side as injection] axillary LN core needle biopsy due to mammographic findings and routine clinical care. Seven patients underwent biopsy one to eight weeks after vaccination with their second dose of mRNA vaccine. Three unvaccinated females undergoing axillary LN core biopsy for routine clinical care and mammographic findings served as controls.
For more on the methods, see Footnote 4.
As the Covid vaccines were rolled out, there was a wave of lymph node biopsies following Covid vaccination due to aberrant breast exam results resulting from swollen lymph nodes. These were most likely in healthcare workers, as the resulting recommendations to postpone exams was issued as early as January, before most states (and especially California) had expanded eligibility to the non-elderly. This may explain why so few truly “recent” lymph node biopsies ended up being available at Stanford Medicine.
SBI considerations for patients and providers scheduling screening exams:
If possible, and when it does not unduly delay care, consider scheduling screening exams prior to the first dose of a COVID-19 vaccination or 4-6 weeks following the second dose of a COVID-19 vaccination.
In “Even-Steven,” I called this study “well written” and recommended reading it directly. But the section regarding germinal centers is a nightmare of confusing and unclear syntax, with both redundant and missing information regarding the biopsies especially, which made today’s review quite difficult. My guess is that an outline for the results was composed before the methods had even been finalized; at least it reads exactly like that was what happened. Anyway, I take my complement back.
The link for the paper’s raw data is https://data.mendeley.com/datasets/j8r94pfrj6/1 - but nothing loads for me. This may be a server cache issue.
I am continuing to search for control results (aside from germinal center qualities in Figure 6). As mentioned in Footnote 7, this part of the paper is a mess.
From Method details:
For in situ hybridization, manual methods were used as previously described (Cloutier et al., 2021), using manufacturer-recommended protocols with the RNAScope 2.5 HD Assay-RED kit and probes from Advanced Cell Diagnostics (Newark, CA). Two SARS-CoV-2 vaccine probes were developed to target bases 101–1143 of the spike encoding sequence of the BNT162b2 vaccine or bases 101–1488 of the spike encoding sequence of the mRNA-1273 vaccine. Both probes recognized SARS-CoV-2 mRNA vaccine, thus only the SARS-CoV-2 vaccine probe recognizing bases 101–1488 of mRNA-1273 vaccine are presented. To assess the specificity of SARS-CoV-2 RNAScope vaccine probes, they were tested against SARS-CoV-2 infected placental tissue, in addition to staining for SARS-CoV-2 viral probe which targets bases 21631–23303 of the S-gene. SARS-CoV-2 RNAScope vaccine probes did not recognize SARS-CoV-2 virus. In addition, for each tissue tested there were internal negative control areas which did not react with SARS-CoV-2 vaccine probe.
There’s little reason to expect that a Covid-vaccine tailored mRNA probe would flag virus mRNA, since the former use such a substantially revised (“optimized”) choice of codons compared to the latter (so that if the virus spells a certain amino acid with a U, for example, this would be changed to a G or C as long as doing so still spells the same amino acid, etc.). But I do find the language about both probes being equal confusing, since Pfizer/BioNTech and Moderna each made difference sets of changes to the spelling.
Gorski, David. “The latest antivax false claim: mRNA vaccines against COVID-19 are not vaccines but “medical devices” or “gene therapy”.” (2021, February 8.) Science-Based Medicine.
Reassuring…
Does he literally not know what plastic is.
Thank you so much for this breakdown. 👍🏽💫 Definitely an important discovery, I wonder what people would say who thought mRNA would be broken down quickly in the muscle. I can't wait to read part two!
Well done. Even this old retired chiropractor can understand this.