


Tolerance (Maims and) Kills - Potential Examples
Some more examples and discussion of the Tolerance Kills theory.

Since July of 2022, brain fog, driving, listening, and focus all started to become very concerning and worse for me. I shared this in the Long Covid program, and a bunch of tests were run. November 2022, I was diagnosed with a Cognitive Brain Injury. A lot of my tests I fell in low percentiles. Short-term memory issues, listening, comprehending, spacing out, and focusing etc. I knew something was not right, I could feel it. Having it confirmed was nice, but also very terrifying.
[…] I am self limiting my driving because it has become very difficult and scary. I have ok days, not good days, and mainly bad days. From July 2022 to December 2022, my symptoms have gotten worse. For the most part, doctors don’t know if I will get better or when, no promises. All I can do is try, and I am willing to do anything. Except inject gold into my blood or take Ivermectin.1

Are the mRNA-Injected Unable to Limit SARS-CoV-2 Replication?
(Related: A 2024 study shows higher rates of Long Covid (per-infection) among Covid vaccinated children; see this post.)
In the wake of the Incredible New News About Tolerance based on the New News About the Brand New Tolerance Study, the proposal, first published by Igor Chudov, that tolerance leads to simmering or uncontrolled viral replication leading to “dying suddenly,” hasn’t really taken off. Here is Igor’s first post, in substack-cameo:

Although both of Igor’s posts (the second being from last week) have more engagement than I can generate, I want to try to amplify the theory by highlighting some recent possible real-life examples, followed by discussion of the biology.
First, the theory. Then two recent cardiac cases, followed by the Long Omicron example of “Squatchin Randy” quoted above. Finally, some more discussion. All of the case studies will, by necessity, be completely invasive of the privacy of the maimed and/or dead. There is no helping the blend between journalism and voyeurism that examining this topic leads to. (It’s like hard-working, normal people can’t unquestioningly take multiple experimental gene therapy injections and then suddenly die in private any more! What is the world coming to?!)
Tolerance Kills: The Theory
I previously described the theory as item three in my list for explanations for all the sudden cardiac deaths. As reports of post-infection complications continue to mount, I grow more inclined to move the theory to the number one spot on my list:
Tolerance-assisted viral cardiac destruction.
The last proposed mechanism [for sudden cardiac deaths] reflects the apparent correlation of sudden deaths with the recent BA.4/5 summer wave. It may be that IgG4-mediated tolerance of the spike protein results in long-term “smoldering” of the virus after infection. While these antibodies still neutralize the virus, they lead to T Cells ignoring infected cells, which ultimately may result in the virus eating away at the heart. This theory was in fact proposed by Igor Chudov early this summer [in the same post cameoed above]:
Tolerance ultimately makes deaths “from Covid” look like deaths “with Covid”. If a spike-tolerant boosted person dies from a heart attack that happens due to overexpression of the virus, it may seem unrelated. But it is NOT unrelated.
Igor’s remarks build off of my post reporting on IgG4 tolerance and some discussion in the comments. And, as always, credit for first proposing that the Covid vaccines will induce tolerance goes to Markael Luterra, who writes at Dendroica Project and his blog.
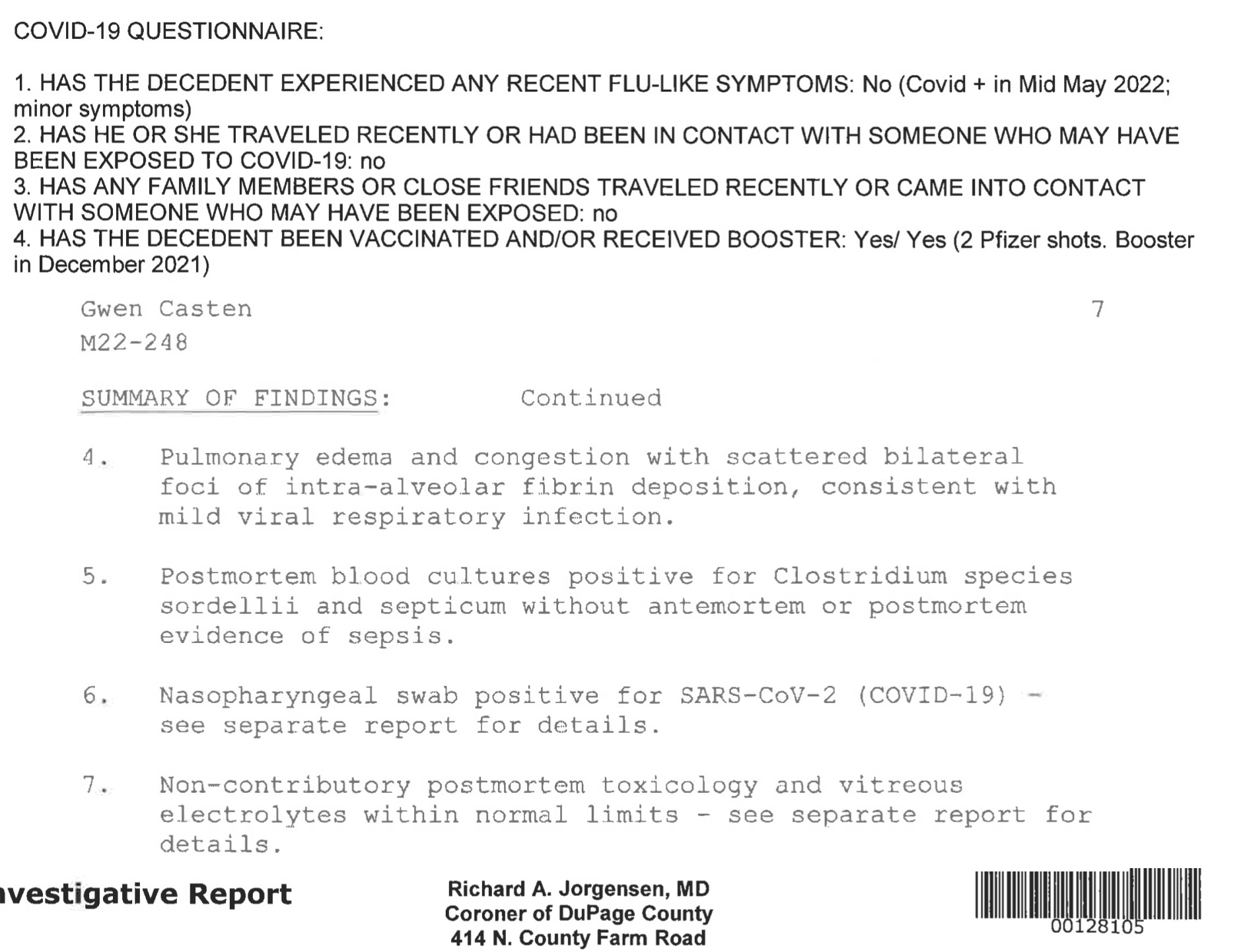
Previous notable potential-examples of infection-associated sudden cardiac death include Gwen Casten, daughter of Illinois representative Sean Casten:
This past June, our daughter, Gwen Casten, died of a sudden cardiac arrythmia [this is not a valid post-mortem diagnosis, but anyway]. In layman’s terms, she was fine, and then her heart stopped. […] She was fully vaccinated, and quarantined after occasional positive, asymptomatic COVID tests during the omicron wave.
—@teamcasten (instagram.com), October 7, 2022
And Julie Powell, who developed “Black Hairy Tongue” and then died out of the blue in late October, just over a month after “getting over” her infection with SARS-CoV-2:

Case Study 1: Post-symptomatic “breakthrough” infection myocarditis

In early August, Waddell and her husband were preparing to go on vacation and tested positive for COVID-19. She was vaccinated and boosted and felt surprised by how sick she felt.
“Body aches, fatigue, fever, your respiratory stuff, sinus congestion — I was sick for about 10 days before I started to feel better,” she says. “I did start to feel better. I was back to work. I was actually going to school and started.”
After returning to work and school, on Aug. 28, she took a walk, something she usually did for three to five miles a day. But when she was about a half mile from her house, she began to struggle. […]
Two days later, she was coughing and achy and asked her doctor for a chest X-ray, which came back normal. She called off work two days and went to her local urgent care clinic. She did not test positive for COVID-19 or flu. […]
But her symptoms intensified. She experienced body aches, cough, “overwhelmingly bad” fatigue and vomited. […]
That’s when Waddell went to the emergency room.
“My blood pressure and oxygen levels were really low,” she says. Pretty much immediately, they could tell something was wrong.”
“My lactic acid was high, which is a sign of sepsis, and they did a CT scan, and I had pneumonia pretty bad,” she says. “That is about the last thing I remember. I woke up 10 days later in Chicago.” […]
At this point, Waddell was diagnosed with myocarditis associated with her recent infection with SARS-CoV-2. Regarding the ambiguity here, more will be discussed below.
By the time Waddell reached her local hospital, doctors needed to act fast to support her. They implanted an Impella, a temporary device to help her heart pump blood. Patients in heart failure normally need help with the left side of the heart, where Waddell's device was placed. But her doctors noticed the right side of her heart also struggling, so they implanted another Impella made especially for that side. […]
“The amount of life support that she needed when she arrived at the University of Chicago was pretty much the most amount of life support that somebody can do,” Dr. Abdul Hafiz, structural heart disease specialist at SIU Medicine, tells TODAY.com. “Her heart and lungs were basically not working at the time.”
Waddell experiences a better-than-expected recovery after this point.
Case-study 2: Asymptomatic infection and cardiac failure
Case study 2 infers previous Covid-vaccination based on travel: Bali requires at least a primary course absent medical exemption.2

A young woman has died from complications related to contracting Covid on a holiday with her partner.
The 24-year-old woman from Aldinga in South Australia, Hayley Beadman, passed on Thursday, December 27 at an Adelaide hospital after going into a myocarditis-induced cardiac arrest. […]
Ms Beadman was rushed to Flinders Medical Centre in Adelaide's south when she couldn't control her breathing and was experiencing chest pains.
She went into cardiac arrest soon after reaching emergency, doctors diagnosing her with myocarditis due to a positive Covid test.
“We didn’t know we had Covid because we didn’t have any symptoms,” Mr Moore told The Advertiser.
Case-study 3: Mild “breakthrough” infection to Long Omicron
“Squatchin Randy” self-reports being a physically active, boosted 42 year-old before catching the virus immediately after leaving perpetual self-lockdown during Christmas, 2021.

The voyeurism-as-journalism meter runs high in the following review of Randy’s medium.com essay, as the writing makes his post-infection brain fog evident throughout. On the other hand, the reader is forewarned that the entire post may be a poorly-written, fictional “Covid is Not Over” parable (and many readers might still be of the opinion that all Long Covid anecdotes are crisis fictions designed to either siphon resources from the rest of society or promote the return of endless lockdowns):
My household was super cautious with covid. My wife, Val, and I didn’t really start going out again until the fall/winter of 2021. We both were still masking, had gotten the vaccine/boosters, and then Omnicron hit December 2021. […]
Well, my wife and I got Covid. We tested positive a day after our Christmas party, we woke up sick. Was it the party? Was it the promotion dinner? Who knows? But we had covid and we were sick. My wife, more so than I, I mainly just felt tired, fatigued, sore, and a minor cough, itchy throat. […]
February 2022 hit (I was keeping notes), and that is when I started noticing/feeling other weird things happening. Fatigue and weakness continued, but now I was always sore and short on breath. This is also when I began having very bad and strange GI issues. Usually having one, maybe two stool movements a day, it started to be 3, then 5, then up to 10. Went from solid to massive diarrhea, then blood, then lots of blood. I began to freak out by the end of February. I was not able to see a doctor until April 20th. In the meantime, all my symptoms of fatigue, overall body soreness, headaches, lack of sleep, dizziness, balance issues, and tinnitus all continued to progress, and I began to take notice. […]
May of 2022, my wife and I went to New York City, Boston, and the MLB Hall of Fame in Cooperstown, NY for a vacation, our first since before the pandemic. We took every precaution we could, and I still got Covid again less than 5 months later. This time, I got really sick, much sicker than in the winter.
Throughout the summer of 2022, my GI issues continued to get worse. All of my symptoms were progressing and getting worse. I started getting concerned and scared. I had to wait it out until my September doctor appointment. My GI issues got so bad that I was going to the bathroom 20+ times a day, pure diarrhea and blood. I would soil my pants many days, sometimes in public. It was all becoming too much and very embarrassing.
Now, a reminder. I was 42, turned 43 in August 2022. I am not old, I was at peak physical shape for myself. I could go long and hard at high elevation, could run, could do anything.
Randy reports being diagnosed with autoimmune colitis, followed by improvement from steroid treatments. The essay continues with details of treatment at the Scripps Long Covid center, none of which has yet helped with Randy’s cognitive and cardiac issues and general lack of energy and well-being:
Next week, I go to get my heart checked on, and a bunch of tests ran because something isn’t right, I don’t feel right. Most likely, POTS is suspected, I show all the signs and symptoms. My autonomic system is messed up.
Discussion
The IgG4 Panic has taken on a life of its own these last two weeks, with intense focus being assigned to “IgG4 Related Disease” and less discussion of the implications for infection and immunity to SARS-CoV-2.
My take on the biology hasn’t changed from my initial remarks in July. Especially, that this is less a story about “boosters” than of the recklessness and excess built into the basic design of the mRNA transfections.
i. mRNA Transfection: a Tolerance Machine
First, using host cells to produce a foreign antigen, absent associated molecular markers of viral infection, intrinsically risks tolerance: The immune system must associate spike protein with “self.”
ii. Antigen overkill from the start
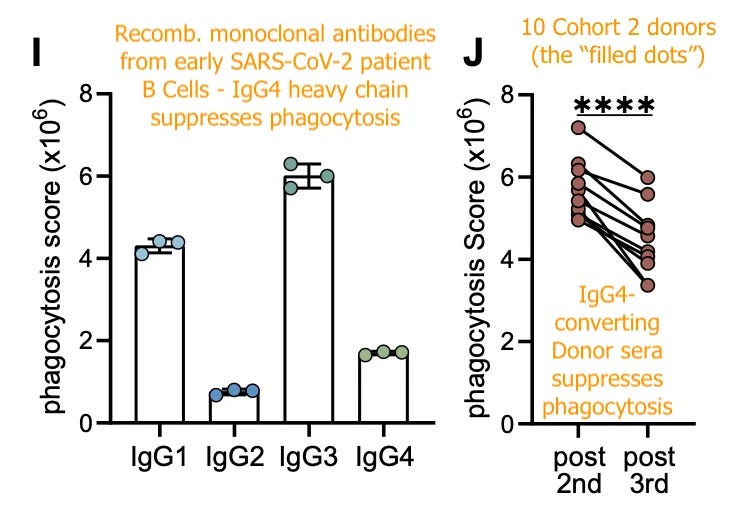
Second, the booster campaigns merely repeat, not invent, a critical error in how these injections are used, ie. as prophylactic against infection. In both cases the assumption is that antigen exposure must be so great as to generate temporary sterilizing immunity to a respiratory virus (by promoting the production of so much IgG that it somehow simulates mucosal immunity). Irrgang, et al. makes it clear that even two doses is total antigen overkill, and begins the march of anti-spike memory B Cells toward the IgG4 phenotype:

The 3rd dose only stimulates the IgG4-producing B Cells that have already emerged in the months following the 2nd dose. This is because tolerance results from sustained antigen exposure. Röltgen, et al. made it clear a year ago that spike protein lingers in germinal centers for months after injection. This may or may not be evidence of spike persisting elsewhere in the body; but it is certainly proof that the 2nd dose was probably never necessary for a vigorous immune response to begin with.

Long term retention of antigens in germinal centers, it turns out, may be a normal thing. The actual persistence of spike outside of germinal centers is still unclear; though Patterson, et al. found canonical and mutant spike protein in monocytes in individuals experiencing Long-Covid-like post-vaccine symptoms.3
Of the S1 positive post-vaccination patients, we sorted the CD16+ cells from six patients as previously performed for PASC patients9. Upon isolation of the protein, we demonstrated by LC-MS that these CD16+ cells from post-vaccination patients also contained S1 protein [the detachable “head” of the spike protein] months after vaccination (Fig 5A). Further analysis revealed that these S1 positive, CD16+ cells also contained peptide sequences of S2 [the stalk of the spike protein], and mutant S1 peptides (Fig 5B).
Ultimately, Irrgang, et al.’s results still speak for themselves in demonstrating that 2 doses of mRNA for spike is already overkill.
iii. Neutralization without clearance
The final point regarding the biology of post-mRNA tolerance is that IgG4 antibodies will still neutralize the virus, at least “on paper” — they will make it difficult for the virus to enter cells, and may tamp the direct, toxic and procoagulant properties of the virus.
The issue, as tentatively validated by Irrgang, et al.’s phagocytosis assay, is whether IgG4 suppresses cellular immune response to spike. After post-2nd-dose IgG4 conversion, in vitro antibody-mediated T Cell “cell eating” was suppressed in all mRNA-vaccinated donors.
iv. Tolerance Kills vs. A “Straw Breaking the Camel’s Back” Model
The reason for believing that IgG4 antibodies will limit damage (coagulation, etc.) from circulating virus and spike S1 subunits during infection is that otherwise, boosters ought to be far more destructive — which is to say, even better than tolerance-complicated infection at “breaking the camel’s back” with compounded spike damage.
After all, the whole reason for tolerance, potentially, is that the mRNA transfections deliver more spike than most infections. However, antibodies elicited by the first injection appear to be protective of dose-dependent harms.
Returning to Röltgen, et al., it was found that antibodies may mask circulating S1, explaining why post-vaccine spike showed up only transiently after the second dose:

Transfection-elicited antibodies may also, as said, prevent circulating virus and S1 subunits from injuring during infection. In general, this would be consistent with the observed severe efficacy that everyone in The Resistance wants to deny has been validated by mountains of research — the Covid-vaccinated do not experience the normal bouts of acute post-infection hypoxia and embolism associated with “Covid-19.”
But, they still seem to die from infection — as in the case of Casten, Powell, and others. Casten’s autopsy did not note any coagulation-related pathology;4 the conclusion of “sudden cardiac arrhythmia” was simply medical jargon for “she died” (arrhythmia can not be detected post-mortem; and ischemic damage from cardiac arrest will obscure the damage that leads to arrest, absent obvious markers like coronary artery plaque or inflammatory infiltrates).

Naturally, it may be more parsimonious to default to a theory that spike exposure from infection merely “breaks the camel’s back” and reveals preexisting cardiac damage from the injections. However, nothing seems intrinsically implausible about the possibility that lingering viral replication could be leading to cardiac destruction both with and without inflammation, due to tolerance of the spike protein mediated by IgG4.
v. A thousand ways to die: Personalized immune sabotage.

Whereas anti-spike IgG4 will dampen cell-mediated inflammatory response to spike, persistent cellular destruction from the virus itself may trigger an inflammatory response. This would only mirror the paradox observed during severe Covid-19, where immune “over-reaction,” if it occurs at all, is in fact only a delayed effect of immune suppression — the reaction is to the extensive tissue destruction the virus has been allowed to wreak.5 And in many or most cases such "over-reaction" may never come about, despite severe disease leading to death.6
Currently, the predominant paradigm is that an overexuberant immune response mediated by excessive proinflammatory cytokines drives excessive lung injury and a procoagulant state. Accordingly, death is assumed to be primarily due to inflammatory lung injury, disturbances in micro- and macrocirculation, and resultant respiratory failure or vascular coagulopathy. This concept of a cytokine storm–mediated death in COVID-19 patients has been popularized in both the lay press and many leading scientific publications […]
Paradoxically, a second and diametrically opposed theory for COVID-19–induced morbidity and mortality is an “immunologic collapse” of the host’s protective system. This collapse of host protective immunity manifests itself as a failure to control unrestrained viral replication and dissemination with direct host cytotoxicity. Support for this contrasting theory is based on the observed progressive and profound lymphopenia, often to levels seen in patients with AIDS.
Multiple recent studies show that unlike the cytokine storm, which is often considered episodic, lymphopenia is incessant in critically ill COVID-19 patients with and correlates with increased secondary infections and death. Postmortem studies of patients dying of COVID-19 have also described a devastating loss of immune cells in spleen and secondary lymphoid organs
IgG4-complicated persistent SARS-CoV-2 infection may be a less dramatic mirror of this paradox. As in cases where immunologically naive individuals mounted a suppressed immune response, leading to uncontrolled viral replication and organ injury, mRNA-vaccinated individuals levy a suppressed, but controlled response. The virus works slowly; inflammatory responses arise only in cases where viral replication-induced cell death activate innate immune inflammatory pathways (via DAMPS).
The immune system is rendered blind to the virus, but not to the damage it causes. However, given a slow enough course of viral replication (imperfectly suppressed by neutralizing anti-spike antibodies), it is plausible that a cardiac crisis would not be preceded by inflammation at all.
Not a bit of support for this theory, it should be pointed out, is found in the Augsburg autopsy series by Hirschbühl, et al.
Viral RNA is found in cardiac tissue for the “breakthrough”-infected listed as dying of “pneumonia” as often as for those dying of cardiac complications. However, as all patients in this series were elderly, these results may have nothing to say about the young who on a more rare basis have been dying suddenly post-infection:
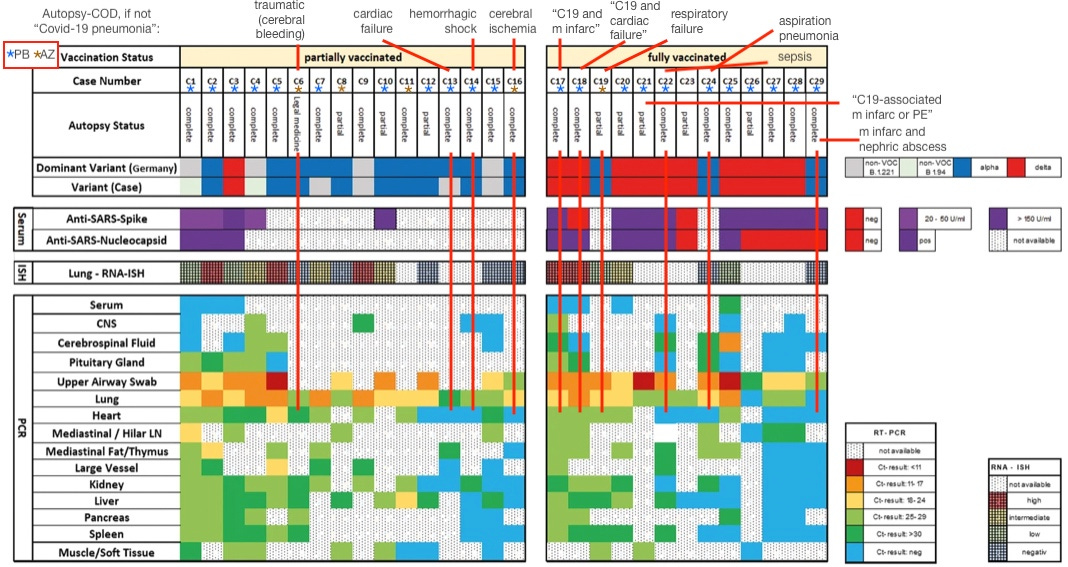
Additionally, in the “fully vaccinated” set, PCR-positivity was between 28 and 283 days after the second dose, which may have been too early for IgG4 conversion in most cases. IgG4 tolerance developing on a delay is obviously one element of why the trend of post-infection sudden deaths did not become apparent until after this summer, in the context of the Tolerance Kills theory.
As of now there is an absence of strong clinical evidence for a role for mRNA-induced tolerance in post-infection deaths, rather than evidence that such a role is absent.
Conclusion: Consistent with case studies
Overall, tolerance-complicated clandestine persistent infection could be involved in all three of the case studies highlighted in this post — the asymptomatic sudden myocarditis death; the heavily symptomatic nonfatal myocarditis; and the mild to severe reinfection that may have in fact been one endless chronic infection in the gastrointestinal tract, leading to severe post-acute symptoms and autoimmune complications.

“Squatchin Randy.” “20 Miles to 900 Feet: My Long Covid Story.” (2022, December 18.) medium.com
See https://kemlu.go.id/losangeles/en/news/11727/update-indonesia-travel-restrictions, which appears to offer an official statement; or the privately-managed example below which reports the same info:

Patterson, BK. et al. “SARS-CoV-2 S1 Protein Persistence in SARS-CoV-2 Negative Post-Vaccination Individuals with Long COVID/ PASC-Like Symptoms.” researchsquare.com
See Hockett, Jessica. “Autopsy Report for Unexpected Death of U.S. Congressman’s Daughter.” (2022, October 18.)
Sinha, P. Matthay, MA. Calfee, CS. (2020.) “Is a "Cytokine Storm" Relevant to COVID-19?” JAMA Intern Med. 2020 Sep 1;180(9):1152-1154.
Remy, KE. et al. (2020.) “Severe immunosuppression and not a cytokine storm characterizes COVID-19 infections.” JCI Insight. 2020 Sep 3; 5(17): e140329.
Squatchin Randy didn't get "long covid" after he got covid. He got it after getting vaccinated and boosted and THEN getting Omicron. Which is exactly what those studies show - that getting vaccinated, boosted, and then a breakthrough infection converts everything to IgG4. And he's so brainwashed he won't even connect it to the vaccines - and neither will his doctors, the so-called "experts" on Long Covid...so much so that he won't try ivermectin, an incredibly safe drug! Sooo infuriating to read! I feel bad for the guy but damn...brainwashed!
Tolerance is incorrect to describe IgG4 mediated disease state. With IgG4, the body attacks the pathogen using eosinophils. It is a milder attack to avoid immunopathology. It is normally used against parasites. Here, a failed vaccine is provoking an anti-parasite immune attack against a virus.
Severe COVID itself is due to vaccine induced immune misfiring, specifically traditional vaccines programmed the immune system to perceive SARS-CoV-2 as a parasite. Allergy is basically anti-parasite immune response against non-parasite antigens.
COVID-19 severity is a result of tetanus, flu vaccine-induced allergy to the SARS-CoV-2 virus; Use famotidine, cetirizine, ivermectin to treat
https://vinuarumugham.substack.com/p/covid-19-severity-is-a-result-of
Immunological Mechanisms Explaining the Role of Vaccines, IgE, Mast Cells, Histamine, Elevating Ferritin, IL-6, D-dimer, VEGF Levels in COVID-19 and Dengue, Potential Treatments Such as Mast Cell Stabilizers, Antihistamines: Predictions and Confirmations
https://europepmc.org/article/PPR/PPR241819