


Negative Long Covid Efficacy in Kids (maybe): New, large American study
Higher rates of presumed Long Covid after "breakthrough" infection

Higher rates of putative and diagnosed Long Covid per-infection in vaccinated kids
Complementing last week’s study, a new study1 has been published in which the question of outcome rates per-infection is extremely relevant to a useful interpretation of the results.
The study (Razzaghi, et al.):
The question last week:
Do the Covid vaccines reduce the rates of severe disease in children if they are infected? (no).
The question this week:
Do the Covid vaccines increase the rates of Long Covid in children if they are infected?
This study suggests the answer is yes.

If true, this (per-infection) increase is mild, but would still represent a substantial net negative for kids and teens in the long term given the rareness of severe outcomes (and no proven reduction of the same anyway). I will revisit the relevance of the “long term” qualifier when discussing the findings below. As for the mechanism of “negative Long Covid efficacy,” I can only suggest my own previously-elaborated speculation that IgG4 tolerance may be increasing post-infection harms among the young (whereas for the old, any such increases would be masked by reduction of severe acute infections):

If false, it would likely be because the increased rates of post-infection conditions being used as a proxy for “Long Covid” in this study are driven by direct injury from the Covid vaccines. In which case, obviously, the vaccines are still a net negative. Alternately, Covid vaccination introduces some bias for increased reporting of Long Covid or other illnesses despite the fact that the unvaccinated controls were matched for demographic factors and timing of unrelated health encounters — this is plausible, but not compelling.2

The setup
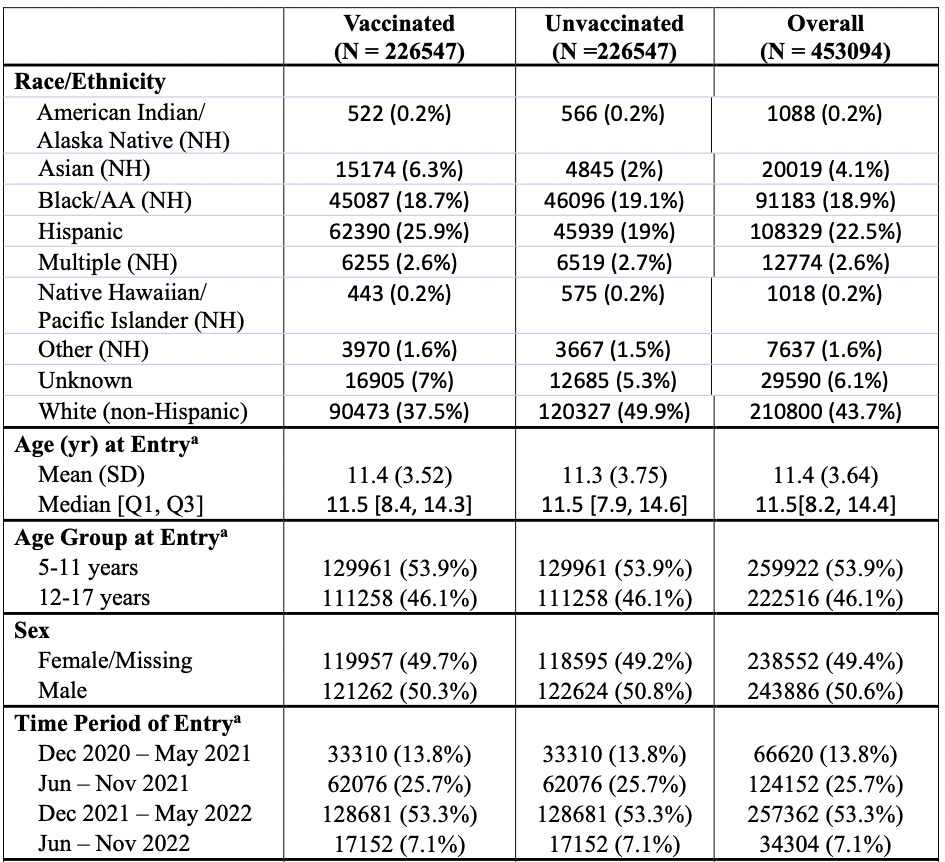
The approach taken by Razzaghi, et al. resembles last week’s reviewed study: In a large network of American healthcare systems, Covid-vaccinated teens and older kids (5 - 11 years old) are matched with unvaccinated kids who had interacted with their respective systems for some other reason around the same time.3
Both cohorts are limited to “valid matches” in terms of time of entry and demographic characteristics; this reduces the representativeness of the results, but better answers the question of what difference the vaccine makes.
Overall, there are 129,961 each of vaccinated and unvaccinated 5 - 11 year olds, and 111,258 each for the teens. It’s a big study.
This is not to dismiss the limited reliability of the data. Is being diagnosed with such-and-such so-and-so days after a reported infection really “Long Covid,” or an unrelated coincidence? Nonetheless, there is little obvious reason to presume that Covid vaccination introduces a bias for increased or reduced false positives for Long Covid. All that should matter, therefore, is whether actual Long Covid is more or less common in either group.
Results
As with last week’s study, the “headline” results merely launder infection efficacy as “Long Covid efficacy.” The only difference is that Long Covid efficacy is found to be lower than infection efficacy.
For example
Since few raw values are available, I will simply offer a crude example of the type of results observed in this study. Say that 15% of unvaccinated kids were reported as infected, and .1% as diagnosed Long Covid. Then say that in the same observation window 7% of vaccinated kids were reported as infected, and .07% as diagnosed Long Covid.
In this example case, the per-infection rate of Long Covid must be 1.5 times higher among the Covid vaccinated.
This outcome is reported by the authors themselves, as in the above table regarding “breakthrough” infections. It is further evident in a simple comparison of infection efficacy with “headline” Long Covid efficacy.
Results in Razzaghi, et al.:
Unadjusted, “Baseline” Diagnosed Long Covid efficacy (1 - (vaccinated Long Covid / unvaccinated Long Covid) over the observation period, regardless of infection rate)
Children 5 - 11 (Omicron only): 16% (82 events in both cohorts)
Teens 12 - 17 (2021 and Omicron): 41.7% (194 events in both cohorts)
(So, Covid-vaccinated kids have fewer Long Covid diagnoses, though the reduction is lackluster even viewed through this lens. But even before continuing it should be obvious that this is still too low (lower than infection efficacy will be).)
Infection efficacy (1 - (vaccinated infection / unvaccinated infection)
Children 5 - 11 (Omicron only): ~48%
Teens 12 - 17 (2021 and Omicron): ~58%
Note, again, that without the raw numbers for infections, it is not possible for me to reproduce the authors’ findings from scratch in order to prevent an error in interpretation on my part. One element of the study which prompted extra review on my part was Table S2’s “Immunization status” variable. This finds that “Immunized prior to infection” lowers the odds of Long Covid. However, this simply reflects a disconnect between the described variable and the likely denominator (which is “immunized at all”). This consideration mostly represents an abundance of caution on my part; the conclusion I offer here is confirmed in the authors’ own discussion of the findings regarding “breakthrough” Long Covid efficacy (see bottom of this post).
Conclusion: The vaccine is worse at preventing overall Long Covid than preventing overall infection itself, which means it is increasing per-infection Long Covid.
To reframe these results in the models used last week for severe efficacy:

This study purports to find Long Covid efficacy by observing the Covid vaccinated when the vaccines are still preventing infections. This is only because observations are limited to 2022.4 However, infection efficacy must wane over the long term, and the Covid vaccinated must eventually experience infection. All that matters over the long term — especially for the young — is rates of outcomes per-infection.
If tolerance (IgG4) is making it harder to clear mild infections, resulting in lingering viral presence in select tissues or organs, it should be no surprise that Long Covid is a more common per-infection outcome. (Again, see my previous speculation here.)
What do the authors say?
Author comment on this finding is demoted to the supplemental figures, (adjacent to the graph I have reproduced here, figure S4). Nonetheless the comment is there, and reflects author awareness that this is an important question.
Understanding whether the development of COVID-19 after vaccination (“breakthrough infection”) provides information about risk for long COVID is important for several reasons.
After much throat-clearing regarding the difficulty in reliably measuring both infections (especially unreported infections and natural immunity) and Long Covid, they report:
In this analysis, we observed a small positive association between vaccination against long COVID, with an OR of 1.32 (95% CI 1.18 – 1.49) for diagnosed or probable long COVID in the combined age group (Supplemental Figure S4). For diagnosed long COVID only, the odds ratio was 1.78 (95% CI 1.35 – 2.34). Estimates did not differ strongly across age groups, though the smaller number of cases in younger children results in wider confidence intervals.
The observed association could result from any of several mechanisms; it is highly unlikely that vaccination is causally related to long COVID when the opposite is observed in the larger analyses.
The highlighted portion, however, isn’t a reasonable conclusion. If Covid vaccines are reducing (for a time) infections, then this alone explains the reduction in overall Long Covid.5 It does not at the same time imply any additional protective effect during infection. Therefore, the natural conclusion follows the observation — Long Covid is happening more after infection; the Covid vaccines have a detrimental effect during infection.
Impressed with their own faulty logic, the authors apologetically suggest that some mysterious bias has failed to yield to their efforts to match and adjust the two cohorts.
Again, this is a totally plausible explanation for the results — but not a compelling one.
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


It has perhaps been on preprint for some time. The DOI-URL dates to 2023. But I have never seen it shared or discussed before today’s publication.
For example, if Covid vaccines increase the rate of asymptomatic infections, but only by “preventing mild infections,” they may skew reported infections to less mild cases. This however would depend on having some exclusive protective effect on mild infections in children. Not compelling, as I said.
Regarding mere reporting bias, the authors found that Long Covid was less likely when vaccines followed infection. This suggests no reporting bias associated with getting a vaccine, and as well that reported Long Covid is not caused by direct injury from the vaccine. Rather, that the vaccine is exacerbating infection outcomes (which it cannot do retroactively, rather only when given before infection).
Supplemental Table S1: Entry into the study is either “Vaccination date or visit date if unvaccinated.” Previously infected are obviously excluded from matching in either cohort.
Or thereabouts. The cutoff for observation doesn’t seem to be clearly reported.
In their brief discussion of this node of the study in the main, the authors even state the same: “These results suggest that throughout the period of pediatric use, the effectiveness [“effectiveness”] of vaccine against long COVID is closely tied to its effectiveness agains the antecedent COVID-19 episode.”
Isn't there an obvious confounder that vaccinated kids will be from families that are more likely to think covid and long covid are terrible dreadful diseases, and induce "long covid" through something like Munchausen's by proxy?
I've only really met 1 person who told me they had long covid, and it was absolutely clear that, for them at least, it was a pure mental health condition brought on by the overwhelming fear in the media she consumed (plus, presumably, some sort of psychological predisposition).
Covid was her life, she was obsessed with it - and of course commensurately highly jabbed. She told me that 11 out of 12 of her friends who got covid got long covid, which is clearly absurd one way or another.
Any child in her household would have certainly been a) jabbed to the hilt, and b) at far greater risk of reporting long covid because of her mental state.
Yet another paper in which the authors go to great pains to bury the lede, which is that vaccinated kids who get COVID are 78% more likely to later receive a Long COVID diagnosis than are unvaccinated kids.