


Notes on sudden cardiac deaths
Children are dropping dead without warning. Determining if it's because of the vaccines or the virus may be the most important question humanity faces - and might be unknowable.


The New (Cardiac) Abnormal
Children — teens, at least — are mysteriously dropping dead. Deciphering why might be the most important question of the present era. Interestingly, the media has not escalated efforts to blame random environmental factors for these aberrant deaths; unlike last fall, when the public was warned that climate change and cannabis would start giving infants heart disease, the news seems uninterested in remarking on the trend of sudden child deaths now that it has actually materialized.
Meanwhile, as Sage Hana documented yesterday, un-censored comment threads now regularly lead to the crowd-sourced promotion of the theory that the experimental Covid vaccines are the cause of sudden onset deaths; while in censored threads the injections cast an obvious negative space.

In a way, I would say that the injections should be considered guilty until proven innocent: If your daughter dies in her sleep after she takes part in a reckless medical experiment, this should be taken as an experiment-associated outcome at the least.
But at the same time, the vocal “Covid Is Not Over” contingent of twitter has taken not only to crediting the virus for these sudden deaths, but using them as a justification for their continued insistence that normal life is untenable.
Sadly, they may be right even if they are wrong — millions of children have been injected; and so even if the others are not at risk, society is potentially careening toward a crisis that has never been experienced. A sort of famine of human health.
The following is thus a loose, out-of-office post to consolidate some cardiac arrest related commentary; sans the normal amount of supporting citations.
On the docket:
There is no such thing as “sudden cardiac arrhythmia.”
(Anecdotally common) non-recovery after sudden cardiac death means these are not arrhythmia arrests. Hearts are just stopping (asystole or PEA). Possible reasons related to spike protein:
Post-acute myocarditis sudden cardiac arrest.
“Circulatory arrest” - blood is no longer pump-able?
Tolerance of SARS-CoV-2 leading to viral cardiac destruction?
No uptick in cardiac / circulatory deaths in children or teens before vaccines suggests virus can’t be blamed here; but Brian sucks at working with data.
I. No Such Thing as “Sudden Cardiac Arrhythmia”
Earlier this month, Illinois representative Sean Casten published the results of the investigation into the death of his daughter:
This past June, our daughter, Gwen Casten, died of a sudden cardiac arrythmia. In layman’s terms, she was fine, and then her heart stopped.
We don’t know what caused the arrhythmia, and likely never will.
Gwen was a healthy 2022 teenager[?]. She ate well, exercised, got regular check-ups, didn’t suffer from any behavioral health issues, and had close relationships with family and friends. She was fully vaccinated, and quarantined after occasional positive, asymptomatic COVID tests during the omicron wave. She had just come home from an evening with friends, went to bed and didn’t wake up.
We are heartbroken, but we are not unique. Sudden, unexplained heart-failure among young, healthy people is rare but real.
—@teamcasten (instagram.com), October 7, 2022
Cardiac arrhythmia may, in fact, be “sudden,” but as it cannot be reliably diagnosed after death, this diagnosis is meaningless for someone found to have died in their sleep.
So either Casten’s pathologist got creative with microscopic ischemia patterns, or the cause of death was actually determined as “sudden cardiac arrest” and Sean Casten misunderstood. This comment is just to clarify that Gwen Casten’s death is therefore at least possibly, if not likely, consistent with the remarks in the next comment.
II. Non-Recovery Means Sudden Deaths Are Not Arrhythmia
One of the features that seems to distinguish sudden cardiac deaths from prior medical maladies is, well, death — very few of these stories are of the “collapsed, recovered” variety. Those who collapse are not revived.
What this suggests is that the normal most common form of arrest, cardiac arrhythmia, is not driving these events — they are either asystole or pulseless electrical activity arrests.
Cardiac arrest
Unconsciousness, collapse, and pulse-less-ness due to cessation of circulation. Types:
Arrhythmia: Uncoordinated electrical signals cause the “pump” of the heart to jam, like an engine where pistons do not fire in coordination.
Pulseless electrical activity (PEA): Normal electrical signals without action. Here, an electrocardiogram will look normal, but the heart is still not doing anything. Example causes: Traumatic blood-loss, drugs.
Asystole: Cessation of electrical signals, aka “flatline.” This is, essentially, another word for death — the heart is no longer alive. Example cause: Hypoxia (strangulation, etc.)
(All of this is as opposed to a “heart attack,” where the coronary arteries suddenly fail to deliver required amounts of blood to some part of the heart muscle, but pulse and consciousness are not immediately lost.)
And so, when lay-directed medical literature makes claims like the following:
If you see someone collapse from sudden cardiac arrest, call 9-1-1 and begin CPR immediately until an EMS crew arrives. The American Heart Association recommends hands-only CPR, asking people to perform chest compressions to the beat of the classic Bee Gees song “Stayin’ Alive.” This technique may double or triple a person’s chance of survival.
What they aren’t mentioning is that CPR is useless for asystole and many types of PEA. In fact, despite the name, CPR does not “resuscitate” anyone — all it does is delay damage from ischemia (lack of oxygen) in the brain and heart. With that delay, the outlook for revival and functional recovery after defibrillation is higher. But defibrillation only works with arrhythmia. It is useless for PEA and asystole. And so CPR doesn’t help anything with those two, except if it turns out that the PEA in question is caused by drugs, in which case different drugs can restore a pulse.
But the reason you are told by the literature that CPR is so effective, is that most cardiac arrests outside of the hospital in the “Before Vaccine Era” (BVE) were from arrhythmia.
The apparent, anecdotal permanency of these sudden onset deaths therefore suggests that the dead are going from being conscious one moment, straight to asystole or PEA. This provides a clue for the etiology. To my mind, it suggests three possibilities:
Post-acute myocarditis sudden cardiac arrest.
Furthermore, myocarditis is an important cause of sudden death,23 as well as childhood cardiomyopathy.24 A recent long-term study of pediatric myocarditis demonstrated that the greatest burden of myocarditis may not be apparent for 6 to 12 years after diagnosis when children die or need to undergo cardiac transplantation for chronic dilated cardiomyopathy."
Since we know subclinical myocarditis may affect ~3.5% of Covid-vaccinated teen boys (per dose?), the only question is if previous prognoses for myocarditis (which might be more skewed toward severe, clinical cases) translates to this entire 3.5%. Fortunately, at least this seems to be a true Russian Roulette outcome from injection, with the other 96.5% not showing markers of myocarditis:
“Circulatory arrest” - the goopy blood thing.
More concerning are ECG results from that same study, which suggest vastly more widespread cardiac harm after injection (18% of 202 male and 99 female teen Pfizer/BioNTech recipients had ECG abnormalities after the 2nd dose). These rampant abnormalities, and the sudden deaths of teens and others, may be cardiac distress caused by blood thickening. Whether one attributes the disturbing reports of amyloid, string-y white clots to the spike protein or to immune-mediated endothelial perforation, it seems plausible that these giant clots could sabotage the engine of the heart by blocking the “fuel injection system.” Either this or more widespread defects in blood viscosity can plausibly result in PEA just as occurs from traumatic blood-loss: The blood is still in the body, but the heart cannot mount the required pressure to pump it.
Tolerance-assisted viral cardiac destruction.
The last proposed mechanism reflects the apparent correlation of sudden deaths with the recent BA.4/5 summer wave. It may be that IgG4-mediated tolerance of the spike protein results in long-term “smoldering” of the virus after infection. While these antibodies still neutralize the virus, they lead to T Cells ignoring infected cells, which ultimately may result in the virus eating away at the heart. This theory was in fact proposed by Igor Chudov early this summer:
Tolerance ultimately makes deaths “from Covid” look like deaths “with Covid”. If a spike-tolerant boosted person dies from a heart attack that happens due to overexpression of the virus, it may seem unrelated. But it is NOT unrelated.
Igor’s remarks build off of my post reporting on IgG4 tolerance and some discussion in the comments. And, as always, credit for first proposing that the Covid vaccines will induce tolerance goes to Markael Luterra, who writes at Dendroica Project and his blog.


III. Brian Doesn’t See an Uptick in Teen Cardiac Deaths in 2020/2021 (But he sucks at data-ing)
For reasons elaborated further in the appendix below, I attempted to compare CDC statistics for deaths due to diseases of the “circulatory system” by age group. These death codes correspond both to cardiac arrest and stroke, among other things.
It is clear that “The Pandemic™” drove an increase from baseline for younger and middle-aged adults. One thing I will note about this increase is that “sudden cardiac arrest” isn’t really a pathological diagnosis at all. As discussed in segment I, pathologists can’t usually make sense of why hearts stop after the fact. So the virus may have indeed caused an increase here, but only because I00-I99 codes may have been a default for undefined deaths after enough time went by to process them and find no other obvious cause. An easy demonstration of this generic misdiagnosis potential is that in prior years, “circulatory system”-coded deaths surge every winter.
Delineating whether the I00-I99 increases recorded for 2020-2021 are realistically describing “cardiac deaths” as opposed to out-of-hospital infection deaths (with extra diagnostic ambiguity potentially driven by deaths in homeless), would essentially require modeling a comparison with other potentially flawed data, like the “VA long Covid” series. The reliability of the CDC’s stats showing increased cardiac deaths in The Pandemic™ era, in other words, might well be unknowable.
What is clear, however, is that no such trend appears in the 0 - 19 age group. The virus therefor does not seem to explain this summer’s trend of sudden deaths in teens (a period which won’t really be reflected in the CDC’s stats for a few more months, due to lags in death classification).
Both of the following graphs come with a strong User Assumes Risk disclaimer. Due to my ineptitude at working with spreadsheets, I had to manually cut and paste all of the CDC’s numbers to produce an age-stratified plotting. If I made any mistakes, then the graphs are wrong. My resulting spreadsheets are linked for each graph.


If this summer, after the current data lag passes, shows a clear uptick in I00-I99 deaths in the 0-19 group, there isn’t really any way to cite the “Pandemic” as precedent. It will be a truly new abnormal.
Appendix: Rationale for this post
(I wrote the following to more adequately contextualize why I am presenting these three comments in a half-cooked form.)
Since reading and reporting on Carolyn Barber’s Fortune article, I have been paying more attention to the feed of user “@MeetJess” and the “Covid Is Not Over” segment of twitter generally.
Though too much of a newcomer to this strange culture to provide insightful anthropology (and I hope to cease observation before the point where I can decipher whether “adenodog” is self-parody or not), my impression is that @MeetJess is spear-heading a desperate attempt in this quarter of mentally ill shut-ins to fashion a reality where the new normal of sudden deaths everywhere isn’t “vaccine-new,” but “virus-new.”
@MeetJess posts daily threads re-compiling the same news posts that re-report the Veterans Affairs database analyses by Yan Xie and Ziyad Al-Aly, or ancient studies from spring, 2020 that focus exclusively on poorly-treated severe infections, or anything else that can exaggerate the risk for casual encounter with the virus. Today she retweeted a funny-looking graph by @greg_travis:
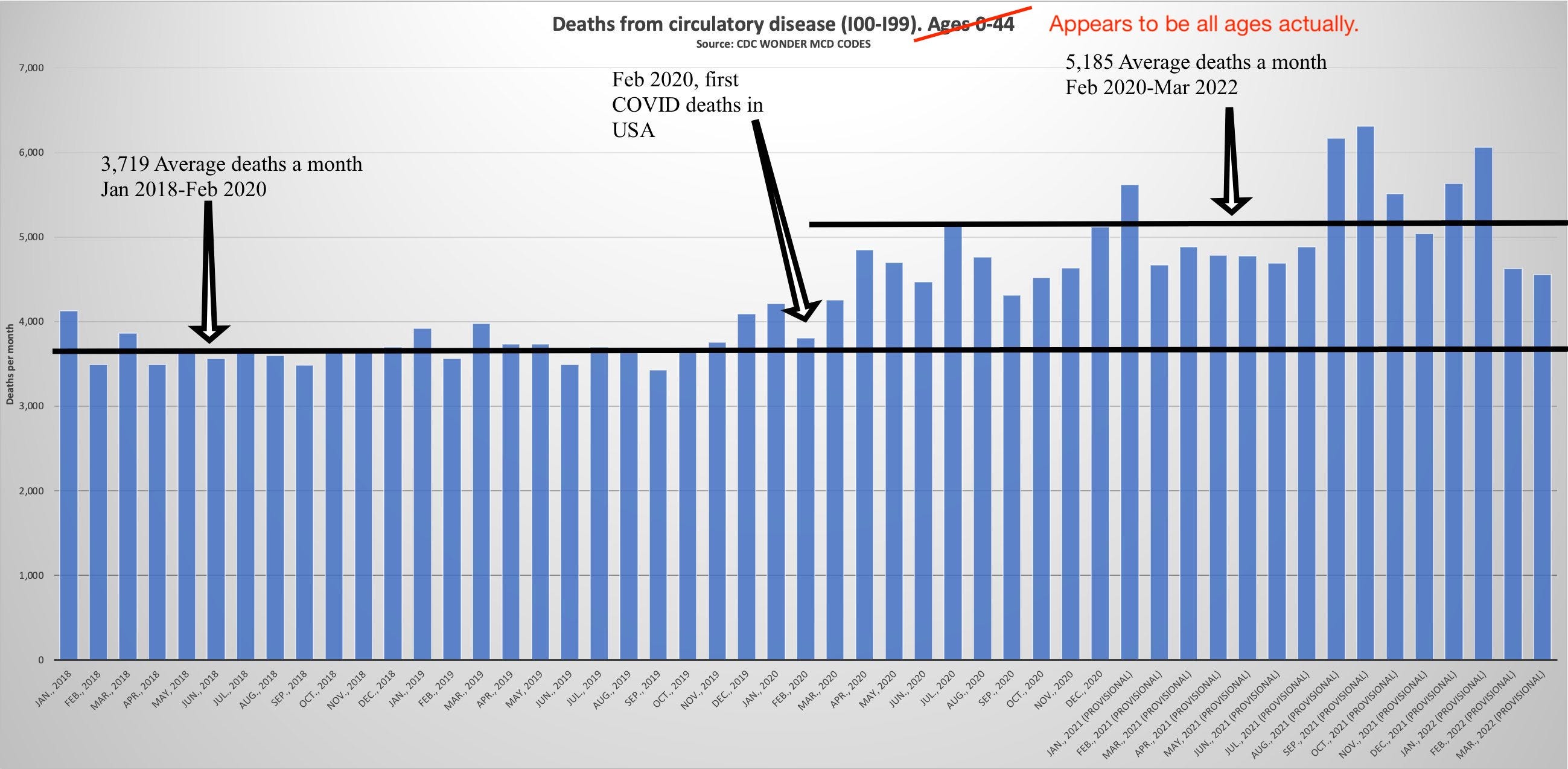
Travis then posted the numbers for 0-24. This is reproduced in the reply screen-grabbed here in order to summarize the way the denizens of C Is Not O World would like to weaponize this type of data:

What’s funny about “Prof Jeffery S Morris”’s comment, of course, is that the black lines don’t correspond to the change in trend in this age group: It doesn’t occur until injections become available to younger adults in May, 2021 (what is Morris the professor of, self-owns?).
However, Travis’s data doesn’t seem to be quite accurately collected or labeled, so I wanted to verify it myself.
All the same, the question of whether the ongoing tsunami of sudden deaths is being driven by the Covid vaccines alone, or along with the virus, is of course incredibly difficult to answer. The current phenomenon of teens and young adults dropping dead in the middle of mundane daily activities, from choir recital to dinner at a restaurant, is unlike anything in human experience. Is the virus also turning young people’s hearts into a “ticking time bomb”?
If this is the case, the delay between the declaration of a Pandemic™ and May, 2021 doesn’t in fact mean the virus is not driving these young deaths: The statistics simply take time to manifest after infection.
The mislabeling of Travis’s 0-44 chart was pointed out by @cineburk, who derived the following plot by accessing the CDC Wonder data herself:
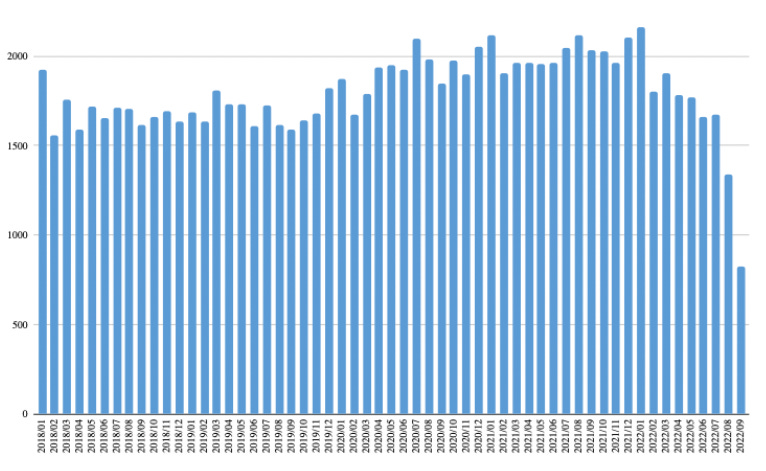
This still supports Travis’s point, however. But it leaves his graph for the 0-24 set unreliable for further analysis here. Therefore, I attempted to compile the CDC Wonder data with my own clumsy, database-illiterate fingers.
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Amazing article! And thanks for mentioning me :-)
a couple of videos of sudden deaths happening:
https://twitter.com/DiedSuddenly_/status/1584307888952311808
https://twitter.com/Mumssayradio/status/1584312861979217920
Nobody knows anything about these deaths and various governments are extremely disinterested in finding out.
Walter Chesnut also weighed in with an interesting idea that it is not the heart that is the problem but the brain stem.
https://wmcresearch.substack.com/p/a-cerebrogenic-hypothesis-for-the
In my opinion, understanding what happened will be exceptionally difficult.
Below is an example of a sudden and unexpected death BEFORE THE PANDEMIC. A 91 year old is giving a speech about history, when he collapses and dies at about 1:50 minutes. But this is a 91 year old, not a 19 year old.
https://www.youtube.com/watch?v=GZmF-TYCxz0
It seems like it's not unknowable whether the vaccine is involved.. all we need to do is look at the mortality broken down into groups of (non morbid) people, with and without the vaccine. It's true that it might be that the vaccine and virus are more deadly when combined, and this too can have reasonable hypotheses of mechanisms, if which you mention a few.
One thing that fascinates me about the C is not O people is why they would think that a virus like this would suddenly appear? Humans didn't co-evolve for millions of years with these corona viruses and then suddenly lose to them in this novel fashion! At some level they must believe the bio weapon / lab leak theory, except they aren't allowed to because science.