Readers who have previously encountered my comments on severe efficacy have likely already read my standard disclaimer: To wit, I hold a position on the legitimacy of the Covid vaccines that isn’t different from most skeptics, and yet my opinion on the efficacy of the Covid vaccines is the same as the mainstream. I think they work the way it was eventually agreed they work — prevent severe disease — but this does not mean anyone should have used them. This sentence implies its own justification: i.e., I think there are other factors in the decision of whether they should have been used, beyond whether they turned out to work. Is this a “complicated” view of the product in question? Only in the sense that life is not a comic book.
Very well; I have repeated the essence of my position. It is further elaborated in my previous post, which also summarizes my case for severe efficacy being real (“there sure is a lot of real-world evidence for it”).
Being 100% right all the time is easy, you probably do it (false)
Now, to characterize the narrative which most Covid vaccine skeptics have adopted about themselves, things have gone as follows: First the experts said Covid vaccines would stop infection, and this was false. Then a series of compromised promises were offered, and all of them also turned out to be false. And oh boy, do we have The Receipts.
But is this really plausible? Wouldn’t it be, just in general, more realistic that these products ended up performing somewhere in between useless and perfect — like any product? For those that cling to the belief that the Covid vaccines were useless: Isn’t it just more realistic that at some point on the escalator of diminishing promises, somewhere before the bottom, the reality of the vaccines met the claims?
If you think of a number between 1 and 6, it is unlikely that I won’t roll it on a die after 3 or so tries. But probably I would not have rolled it on the first try; and if you denied I had rolled it on try 3 simply out of resentment for me being eventually correct, your denial would be just that.
And this, I feel, is the attitude most skeptics have taken with mainstream authorities. “They shouldn’t have made a guess to begin with, not possibly being able to know real-world and long term outcomes based on a perfunctory and rushed trial; therefore they can’t be allowed to be correct even after having the long term data.”
Well, sorry, but of course they can: The problem that led to their wrongness (guessing without knowledge) has been corrected (they have knowledge). Whereas, the skeptics by and large would still insist they were right on the first guess, and that any new information which contradicts this guess is a “trick” or a “lie.”
Berenson’s Truth
Overview
Alex Berenson, absolutely the avatar of this attitude, has recently produced two posts which recycle his long-standing severe efficacy denialism. In one, he offers a totally backwards interpretation of a new study finding that healthier unvaccinated people wind up hospitalized for severe Covid-19, and in another, he sums up his current overall position on the topic of Covid vaccine efficacy.
Before we look at the Ohio study, let’s consider the topic of the other post: Severe efficacy denialism, 3 years in. In a way, this will create a supplement to my argument for severe efficacy from the previous post (linked above): “There sure is a lot of real-world evidence for it; and, justifying a conclusion opposite this real-world evidence requires extreme lengths of cherry-picking, assumption, and contradiction-evasion.”
The reader may scroll past this part if only interested in the new Ohio study.
Overview of the “Epistemic Fouls” in Berenson’s severe efficacy denialism:
Assuming unfavorable results must be bias artifacts
Denying that favorable results could be bias artifacts
Declaring that the vaccinated can’t be compared to the unvaccinated (!), selectively comparing the unvaccinated to the vaccinated despite previous claim
Hiding (or making less accessible to the reader) unfavorable data
Treating hospitalization rates as some kind of “distraction” (!)
Refusing to think rationally about outcomes in non-elderly adults
Refusing to model the healthy user bias theory to see if it can really explain away the data — it is just a magic, “bad juju” that causes all unfavorable observations
1 and 3: Assuming unfavorable results are bias artifacts; declaring that the vaccinated can’t be compared to the unvaccinated
Berenson second recent post offers an overview of his opinion on Covid vaccine efficacy after three years. Because virtually nothing he claims in this post differs from his position in 2021, it is more helpful to exhume and autopsy his first reaction to real-world data on severe efficacy, from that same year. To round out the picture, his top post, which is also almost 3 years old, will also be discussed.
Berenson has been right about many things, but he has been wrong about severe efficacy in the real world since “day one.”
When Israel added hospitalizations to its real-time Covid-19 dashboard, in August during the Delta wave, it immediately reported that the vaccinated were being hospitalized at a lower rate per-person than the unvaccinated. This was even though, at the exact same time, the vaccinated were being reported as infected in the same dashboard at about the same rate as the unvaccinated.
Berenson immediately reported this as a “terrible” failure for the Covid vaccines. Why? Because of the theory (or rather assumption) that the vaccinated in Israel were all healthier than the unvaccinated. Quoting from his August post:
Because the tiny fraction of older people who are unvaccinated in Israel at this point are almost certainly materially different than the vast majority who are. As far as I know, the Israel government hasn’t broken out the differences. But given the pressure to vaccinate, a significant number of those older unvaccinated people are likely simply too sick to tolerate the vaccine - especially those over 80, where overall vaccination rates are even higher.↗
Certainly there would be demographic and statistical differences — bias — between the vaxxed and unvaxxed. But bias is a reason for saying, “Well, let’s be cautious in interpreting this early evidence from Israel for severe efficacy being real.” Not for throwing it out the window immediately.
2 and 3: Denying that favorable results could be bias artifacts, comparing the unvaccinated to the vaccinated despite previous claim
Further, can one really believe that a concern for bias would have prohibited Berenson from announcing that the Covid vaccinated were being hospitalized at an equal or higher rate per person? Of course not. Berenson obviously would have led with this finding — just as, in November of the same year, he incautiously reported that non-elderly British adults were dying at a higher rate. This remains his top post on Substack even though readers at the time could see that the graph was a meaningless comparison of two very differently-aged adult cohorts. (While at the time more non-elderly unvaccinated were dying from Covid 19, of course the unvaccinated, who are younger, would be dying much less overall.) This, from the same man who replied to the Israel dashboard in the August post by declaring “comparison between vaccinated and unvaccinated isn’t useful.” It’s obviously useful to him whenever it suits the right conclusion; as long as it does so, in fact, being unrelated to SARS-CoV-2 infection outcomes is actually a plus.
Comparing X and Y makes me look wrong: Not useful. Comparing X and Y makes me look right: Useful.
Berenson has never cared about the hazard of bias when the results favor his conclusions on severe efficacy; this hazard is just his cope for all the evidence that the unvaccinated had higher rates of hospitalization everywhere before mid-2022 (after which, most now have the advantage of natural immunity).
4: Hiding (or making less accessible to the reader) unfavorable data
Perhaps more tellingly, Berenson’s August, 2021 post performs the tactic of referring to the unfavorable information in the Israel dashboard, without showing it at the same time:
In an effort to play down that reality [that more vaccinated were hospitalized in absolute numbers], Israel has begun to provide data comparing RATES of serious illness in older people who were not vaccinated and those who were. And those show that as of now, unvaccinated people are still becoming seriously ill significantly more frequently than those who aren’t.
But that comparison [i.e., the only relevant comparison for severe efficacy] hides a very big problem.
[Further comments on healthy user bias, mostly already quoted.]↗
Berenson:
Refers to data unfavorable to his and his readers’ preferred conclusion (“this data exists”).
Informs his readers why the unfavorable data is unreliable.
Finally, towards the bottom of the post, shows a sideways photo of the dashboard with values not annotated and with an instruction not to compare the vaxxed to the unvaxxed.
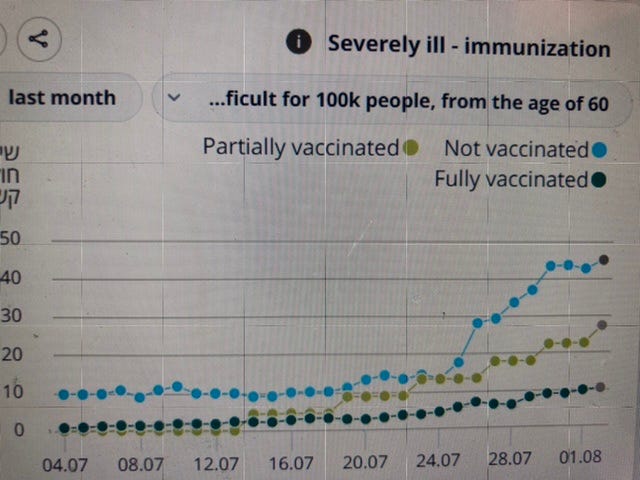
Readers should know what the Israel data says — they should know just what it is that he is arguing is a statistical illusion upon which they should not base any decisions (see item 6, below, for the numbers in question). In this case, Berenson does eventually show the relative hospitalization graph, but only because he does not want to produce his own graph to show what is his true focus, the vaccinated alone:
Remember - comparing unvaccinated and vaccinated at this point hardly matters. THE DARK GREEN LINE IS THE ONE THAT COUNTS:
In his severe efficacy denialism, Berenson relies on obscuring data (over 60 years in Israel) or outright hiding data (under 60 years in Israel, see item 6 below) so that even readers sympathetic to his views cannot appraise or criticize his justifications for dismissing the same data. He infantilizes his reader in exactly the same way as mainstream fact-checkers do: In fact, the data isn’t just unreliable, it’s evil, it’s corrupting of good morals, and you hoi polloi mustn’t be permitted to actually know what it says.
Many other Covid vaccine skeptics rely on this same heavy-handed censorship of whatever it is they are refuting. Refer, then vilify — but do not show. It is why the Covid skeptic community by September, 2021 had already become so out of touch with what data actually says.
5: Treating hospitalization rates as some kind of “distraction” from absolute counts
When Berenson writes, “In an effort to play down that reality [more vaccinated hospitalized in absolute number], Israel has begun to provide data comparing RATES of serious illness in older people who were not vaccinated and those who were,” what does he even mean?
How can a focus on rates be “an effort to play down” absolute counts, rather than first and foremost a good way to provide perspective?
If there were equal numbers of unvaccinated and vaccinated people in Israel, there would be no difference between the ratio of absolute cases and case rates; but since there are different numbers of people in all age groups, we use rates, not absolute cases, to understand whether a given piece of evidence supports Covid vaccine efficacy. Severe efficacy must be a question of rates (ideally, per-first-infection). By even being able to think and write such a sentence as above, Berenson reveals that he doesn’t actually care whether severe efficacy is real or not.
Instead, he only cares about what “looks bad” (absolute numbers when it comes to severe Covid-19; rates for unrelated deaths).
THE DARK GREEN LINE IS THE ONE THAT COUNTS
In this, he shares the same mentality as public health experts — the hoi polloi can’t understand risk, and if they have access to the (unreported) truth about absolute counts, or see data with misleading age comparisons, they will reach the wrong conclusion. The only difference is that Berenson wants this.
Public health experts downplay vaccine failure (the % of recipients who still experience severe outcomes) because they know that many people will opt out of a less than perfect product. Berenson wants to emphasize vaccine failure for the same reason. But his psychological projection is too extreme — merely electing to focus on rates is not an effort to deceive the public.
Rates are what are important!
Actual severe efficacy is not a distraction in terms of vaccine efficacy, even if it is not the only consideration for using the vaccines. But this is what Berenson seems to believe.
6 and 7: Refusing to think rationally about outcomes in non-elderly adults or the healthy user bias theory
So now, just what were the hospitalization rates that Berenson only barely revealed to his reader in August, 2021?
Here is what the Israel dashboard figures were as of the 3rd: 10.7 ongoing hospitalizations per 100,000 for the vaccinated vs. 48.5 for the unvaccinated in the over 60-year-olds group; 2 vaccinated per million vs. 10 unvaccinated for the under 60-year-olds.
Remembering again that infection rates were not too different between both groups (vaxxed and unvaxxed) at the time, these numbers suggested something between 70 - 80% per-infection severe efficacy.2
Berenson doesn’t tell his reader this, because after all, the information is unreliable. And we know it’s unreliable because of, for example, all the presumed over-80-year-olds in the under-60-year old group.
That’s sarcasm. The 5 to 1 rate of hospitalization among unvaccinated under-60-year olds was not driven by 80 year olds on their deathbed. Yet remember that Berenson’s dismissal of the Israel dashboard data leaned on an assumption about the very oldest (emphasis added):
a significant number of those older unvaccinated people are likely simply too sick to tolerate the vaccine - especially those over 80,
Whatever goes on among octogenarians cannot account for lower hospitalization rates in non-elderly adults.
In fact, it should require extraordinary evidence to claim that severe efficacy on the order of 80% could be observed in middle-aged adults due to user bias, let alone to assume it off-hand and never revise this assumption after another year of replicated findings (no comparisons can be made after mid-2022, as the unvaccinated all have natural immunity).
Berenson has never thought seriously about this problem. In fact none of the advocates for the Healthy User Bias Theory have bothered to produce a model for just how strong such a bias would have to be to generate an ~80% per-infection severe efficacy value. As I show in my prior post, this kind of skew is almost impossible: If you include only the very “unhealthiest” in the unvaccinated group, then actually the vaccinated aren’t particularly “healthy” either — they are merely average — and the ratio of severe rates should be far less than a strict comparison between the healthiest and unhealthiest users. The same happens if only the healthiest get the vaccine, though this would not fit with high vaccination rates anyway. And in reality, obviously both groups were not pure outliers but a blend of all types. Healthy User Bias advocates are really asking water to flow uphill with their assumptions; and they should at least try to model how this could possibly take place.
And, even if healthy younger adults preferred the Covid vaccines, this too would not explain severe efficacy in younger adults. Remember that “healthy” young adults were anecdotally over-represented in severe cases and deaths both before and after the vaccines, when compared to higher-risk groups. Therefore, in lower-risk groups, it is seemingly even less likely that healthy user bias can cause illusory severe efficacy. (I have a separate post in mind for this point, so for now I will leave it at the anecdotal argument.)
Conclusion, relevance to severe efficacy denialism in general
Berenson’s recent overview only adds to his August, 2021 post by incorporating his opinion on the uselessness of boosters. As I have no substantial disagreement here, there is nothing else to review.
My other justification for digging up the older post is that it serves as a template for basically all severe efficacy denialism that strayed beyond the more easy-to-dismiss CDC data in the ensuing three years: All of it went through these extreme lengths of “fouling the data” — like an outmatched basketball team who cannot let the other side take a shot. (This is when not simply inventing new rates by changing the denominators; which I gave the related term “toddler basketball.”) Isn’t this behavior itself a confession that severe efficacy is simply real?
As a fitting example of the evergreen relevance of Berenson’s first post on this topic, let’s consider his new report on the Ohio hospital study.
The Ohio hospital study
Now we come to Berenson’s review of a study reporting outcomes among 112 severe Covid-19 patients hospitalized at OSU hospital.3He writes:
On Feb. 6, Ohio State University researchers published a stunning finding - stunning to anyone overwhelmed by mainstream media mRNA propaganda since 2021, anyway. Vaccinated Covid patients hospitalized with respiratory failure were more likely to die than the unjabbed. 70 percent died, compared to 37 percent.
The gap persisted when the researchers matched patients by age and comorbidities. “Vaccination status of hospital-admitted COVID-19 patients may not be instructive in determining mortality risk,” they wrote. […]
One reason the single-hospital papers show worse vaccine outcomes than bigger data sets from public health bureaucrats is that the physicians who write them typically - and correctly - identify Covid patients who received only one shot as vaccinated.
In the agglomerated papers, those patients are categorized as unvaccinated [No, actually; even CDC papers tend to just exclude what few partially vaccinated there are, not to misclassify them]. That statistical trick makes the vaccines look better. But it does nothing to help the patients who have received them.
The rest of his post is a mention of IgG4 measurements in the new paper, a reference to two related studies with ambiguous outcomes, some opining on the biology of severe efficacy, and, very importantly, a reference to mainstream severe efficacy claims. The latter is important, as they make it clear that Berenson views this new paper as another refutation of severe efficacy. Meanwhile, I won’t comment on his biological theories4, as it would be distracting — however, I lay out the biological basis for the plausibility of severe efficacy here.
Thus, only the paragraphs above directly discuss the results of the Ohio study. And so once again, Berenson is referring to data, without showing it.
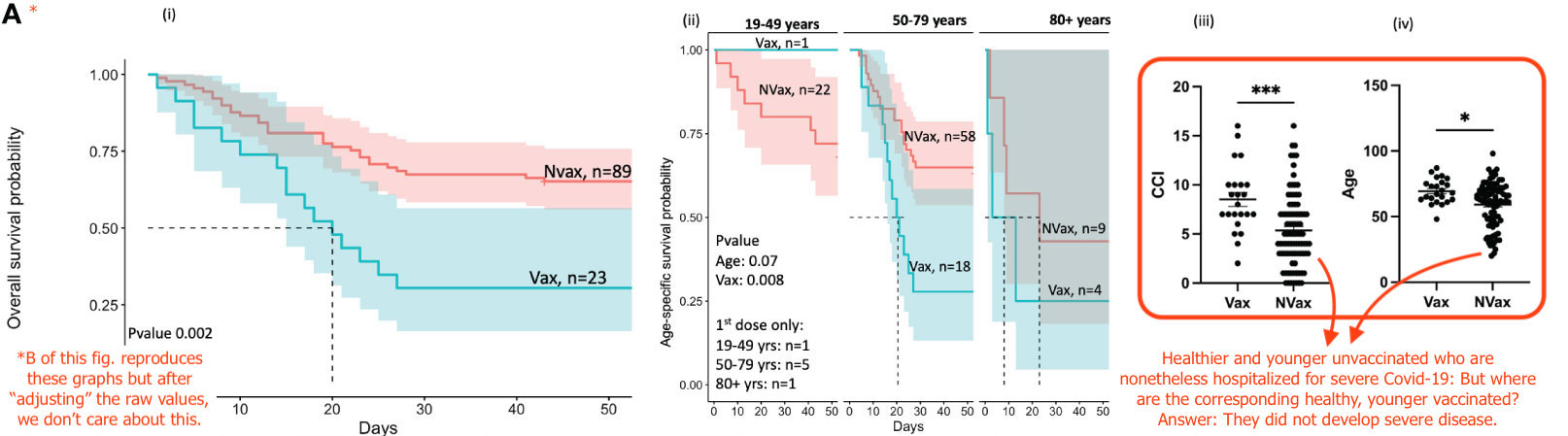
Here is the relevant figure from the new study. For context, unvaccinated cases (“NVax”) include hospitalizations that took place before the vaccines were available, which dilutes post-2020 “user” bias (or non-user, in this case) among the unvaccinated:
It is, let’s not use “misleading,” but less than informative to refer to the results in the new paper, not show them, and claim that the same results could not be explained by group differences in age and comorbidities because the two groups were “matched” in a separate analysis. Berenson fails to tell the reader that actually, the qualities of who ended up in the hospital among the unvaccinated and vaccinated were extremely different. Certain types of vaccinated just weren’t being hospitalized, whose counterparts among the unvaccinated were.
Who gets hospitalized; who dies?
Berenson’s point is that the hospitalized vaccinated almost all died. Once again he commits the “fouls” of refusing to acknowledge that bias could drive a favorable result (the vaccinated were all more unhealthy) and refusing to think through the implications of efficacy in middle-aged adults.
If over the course of two years, both before and after vaccine availability, non-elderly adults are being hospitalized for Covid-19, then the same should happen among vaccinated non-elderly adults in a model where severe efficacy is not real.
It doesn’t matter, in this model, that the vaccines provided short-term infection efficacy that reduced the amount of infections among the vaccinated in the study window. If some infections happened among non-elderly adults, then post-infection outcomes should have been the same: A low but non-zero rate of hospitalizations.
Even though these cases are rare, they belie the idea that “unhealthiness” is the only real driver of severe infections in the unvaccinated. As with any viral infection, people tend to be more susceptible to delayed immune responses as they age beyond their early teens — this is a lottery; it has nothing whatsoever to do with who is healthy. Healthy unvaccinated still showed up to this hospital in Ohio. There is nothing about preferring a vaccine that can stop this from happening to this same small portion of any group of healthy adults except that the vaccine prevented their stupid immune systems from falling asleep at the wheel. Magic healthy user bias juju can’t do this. (This doesn’t mean that healthy people should take Covid vaccines; the vast majority are going to be fine with natural infection; and for all we know, those who wouldn’t have been are just going to trip on a different virus anyway.)
So then, what really counts here? In the strict context of severe efficacy (and Berenson explicitly frames this study as a refutation of severe efficacy), the question is how many vaccinated and unvaccinated end up in the hospital after vaccine approval and up to November, 2022. The answer is 23 and 43, respectively.
This would then need to be converted into a rate based on the number of infections among both groups throughout 2021 and 2022, and breaking results down by age group would be useful; but basically what we see happening in this hospital is the vaccinated majority of Ohio avoiding the outcome of severe Covid-19 throughout the first two years of their existence as vaccinees.
Good for them, I guess. I’m still personally happy not to be vaccinated and worrying about lifelong anti-spike IgG4. But in terms of Berenson’s comments on who “benefits” (in a statistical) sense from the Covid vaccines, it’s notable that real-world outcomes actually support the idea that it’s the rarer, younger adults who would have experienced a severe infection — these exotic birds, not representative of their group in terms of infection outcomes — who derive the most value, or at least just as much as more vulnerable (but of average health) elderly.
A final note on the partially vaccinated
Finally (more could be said, but this study is not so interesting), Berenson’s comments regarding the partially vaccinated are not rational. It cannot be the case that the partially vaccinated make the vaccines look worse unless, either, the vaccine is enhancing infections, or something is “bad” about being unvaccinated. Since Berenson describes misclassification as a “trick,” either interpretation is possible.
The latter interpretation is the mainstream view: The partially vaccinated do not yet have the protection that the vaccine affords. Therefore they are still “unvaccinated.” I do not agree with this view; but again I would point out that there isn’t really a “trick” going on here — much if not most of the time, the partially vaccinated are excluded in these types of studies, not misclassified, and the results are not any different. You will never find a “smoking gun” post which can show a case where doing anything with the partially vaccinated changes the data in any meaningful way. So this theory is magical thinking.
If Berenson believes that infection enhancement is at play, the numbers do not support this. 7 of 23 vaccinated patients had fewer than two doses. This is an overrepresentation of about, let’s say, 5X vs. the “person-time” that vaccinees would have spent at risk of infection in the 23 months in question. Besides this, there were more survivors in this group (presumably because they resembled the unvaccinated in risk factors.)
Defiantly boasting that any positive real-world performance of the Covid vaccines, observed in August of 2021, must be false, is the opposite of caution: Bias is used to justify exactly the wrong stance toward the data.
Further, how could Berenson even know for sure that Covid vaccinated 80 year-olds in Israel were “healthier”? How could he know for sure that this, if true, actually influenced the current rates of hospitalization? What if, for example, none of the “significant number” of too-frail-to-vaccinate were in fact among the unvaccinated being hospitalized — how could their membership be responsible for the hospitalization of those others? “I’m unvaccinated by choice, and have developed a severe course of Covid-19 in solidarity with those who could not get the vaccine” — this is not possible. The point is that before one can declare real-world hospitalization data to be an artifact of the too-frail-to-vaccinate, it is necessary to know whether those individuals are even who are hospitalized. (This point also holds for all “worry window” theories, which fail over and over in the same validation, as we will see with the Ohio study.)
I worked this math out at the time, and my recorded values for this math are the source for the figures used here. These values were derived by mouse-overing the Israel dashboard (the subject of Berenson’s post) for the days of interest. The math, which has long been erased from the dashboard, can be found in my old post; forgive the ironic tone which was a reflection of the farcical nature of summer, 2021. The relevant text:
Thus, using an arbitrary ten-day delay for PCR confirmed infections daily rate and ongoing severe outcome patent rate:
100-(100 x (Ongoing severe rate / -10 day PCR+ daily rate snapshot) Vaccinated / (Ongoing severe rate / -10 day PCR+ daily rate snapshot) Unvaccinated))
What is revealed using this math is that vaccinated hospitalizations prevented per PCR-confirmed infection for over-60s has apparently degraded since the 18th, but not nearly at so fast a rate as might have been guessed from our calculations before. Additionally, the apparent efficacy has increased for patients under 60, despite the scarcity of vaccinated under-60 patients on July 18, thanks to a larger influx of unvaccinated under-60 patients:
July 18 apparent Covid vaccine severe outcomes efficacy for 60 and above:
100-(100x((3.1/6.1) / (10.2/3))) = 85%
August 3 apparent Covid vaccine severe outcomes efficacy for 60 and above:
100-(100x((10.7/12.7) / (48.5/16.6))) = 71%
July 18 apparent Covid vaccine severe outcomes efficacy for under 60:
100-(100x((.05/4.7) / (.2/6.9))) = 63%
August 3 apparent Covid vaccine severe outcomes efficacy for under 60:
A lot of T Cell Fetishization. Many people become obsessed with T Cells in this way. It is a way to hold an “advanced” understanding of immunity by merely going beyond stage one (antibodies) and stopping.
Like you say, this comes down to the initial, too good to be true, repeated ad nauseum claims of ~95% generalised efficacy (back then there was rarely a distinction made between infection/hospitalisation/death healthy/young, young/old).
To break it down (because it is somewhat non-linear and oft misunderstood): 95% efficacy equates to a 1:~20 växxed:unvaxxed risk ratio i.e. vaxxed should be ~20 times less likely than unvaxxed to get infected/hospitalises/die. Real world data very quickly showed effectiveness was vastly less against infection, much less against hospitalisation, and also less against death.
Your example calculation of ~70% efficacy (under 60's population) based on Israeli data, equates to a ratio of 1:~3 I.e. vaxxed were ~3 times less likely to be hospitalised.
Hospitalisation for a middle-aged person going from 20 times less likely to only 3 times less likely is a very considerable loss of effectiveness, and, to play pharma's "trick" of highlighting relative risk reductions: this represents an ~85% relative reduction in the relative risks (advertised relative risk ratio 1:~20, real world relative risk ratio 1:~3)
Keeping in mind that theses were relative risk ratios, we'd need to know the absolute risk before we can consider the actual absolute risk reduction benefit.
I know, I know, Brian will say I am stuck in their paradigm, and the mandates were unconsciable regardless, but I just wanted to restate that numbers did not justify mandates even if Brian has shown Berensons inflated claims (mirroring? the Pharma MSM) are untenable.
It honestly feels as if the COVID skeptic side is in a precarious position. It doesn't seem like much headway is being made regarding any reconciliation over the mass vaccinations and the adverse events. Because of this there seems to be some strange scramble going on, with lots of infighting and a need to hark on points that seem rather moot at this point. What utility is there to pushing the idea of no efficacy, vaccine shedding, or things like that at this point when there are likely to be better points to be made?
This is probably why we are seeing this surge in fringe ideas or conspiracies, or even absurd claims being taken as fact. It's weird to see all of these things happening, and yet it's a likely consequence of any movement that may fizzle out and needs to find a way to sustain itself, because irrespective of the comments suggesting "we are winning" I really don't see much of anything happening any time soon.








Like you say, this comes down to the initial, too good to be true, repeated ad nauseum claims of ~95% generalised efficacy (back then there was rarely a distinction made between infection/hospitalisation/death healthy/young, young/old).
To break it down (because it is somewhat non-linear and oft misunderstood): 95% efficacy equates to a 1:~20 växxed:unvaxxed risk ratio i.e. vaxxed should be ~20 times less likely than unvaxxed to get infected/hospitalises/die. Real world data very quickly showed effectiveness was vastly less against infection, much less against hospitalisation, and also less against death.
Your example calculation of ~70% efficacy (under 60's population) based on Israeli data, equates to a ratio of 1:~3 I.e. vaxxed were ~3 times less likely to be hospitalised.
Hospitalisation for a middle-aged person going from 20 times less likely to only 3 times less likely is a very considerable loss of effectiveness, and, to play pharma's "trick" of highlighting relative risk reductions: this represents an ~85% relative reduction in the relative risks (advertised relative risk ratio 1:~20, real world relative risk ratio 1:~3)
Keeping in mind that theses were relative risk ratios, we'd need to know the absolute risk before we can consider the actual absolute risk reduction benefit.
I know, I know, Brian will say I am stuck in their paradigm, and the mandates were unconsciable regardless, but I just wanted to restate that numbers did not justify mandates even if Brian has shown Berensons inflated claims (mirroring? the Pharma MSM) are untenable.
It honestly feels as if the COVID skeptic side is in a precarious position. It doesn't seem like much headway is being made regarding any reconciliation over the mass vaccinations and the adverse events. Because of this there seems to be some strange scramble going on, with lots of infighting and a need to hark on points that seem rather moot at this point. What utility is there to pushing the idea of no efficacy, vaccine shedding, or things like that at this point when there are likely to be better points to be made?
This is probably why we are seeing this surge in fringe ideas or conspiracies, or even absurd claims being taken as fact. It's weird to see all of these things happening, and yet it's a likely consequence of any movement that may fizzle out and needs to find a way to sustain itself, because irrespective of the comments suggesting "we are winning" I really don't see much of anything happening any time soon.