The Worry Window is the theory that injection with the experimental Covid vaccines has a magical property of increasing infections immediately after the first dose, and that this magical property is either magically self-hiding in most of the data on post-injection-infection-rates or has been systematically hidden by guilty researchers who know that the Worry Window is real.
Because the Worry Window is real (per the theory), all reported values for infection rates in the Covid vaccinated are not valid. Real Covid vaccine infection efficacy is probably always negative.
What Isn’t the “Worry Window”?
Real.
i. 2020 Vision: The Perfunctory Covid vaccine trials reported post-first-dose infections.
Yesterday, while hate-reading a Berenson post (as we all do), I encountered the perfect summary, from prolific Covid-Skeptic-Substack commenter and writer “SimulationCommander,” of what the Worry Window myth leads people to believe is true.
I am highlighting this example not with the intention of putting anyone “on blast” (science term), but just to ensure I am not stealing illustrative comments without credit. This is what the “canon” understanding of what happened in the trials is (emphasis added):
They [Pfizer] had to know it all [IgG4 conversion, etc.] because of how they set up the trials to begin with. Allowing them to define 'vaccinated' as 2 weeks post second shot basically allowed them to only count the people who got through the worry window as vaccinated -- then we went a step further and counted those infected people as UNVACCINATED!
Your school has a 100% graduation rate if you only count the students who make it through graduation!
Now, this isn’t necessarily claimed by proponents of the Worry Window, as far as I know. It is just what someone reading Worry Window claims would naturally imagine would be the case. “If this Worry Window thing is true, they must have hidden post-1st-dose infections in the trials!”
So, call this a strawman version of the Worry Window argument. Or the bailey to the motte; even if it’s only an implied bailey. My justification for starting with the strawman is that I think lots of readers believe the strawman is true. In fact, I also imagined this must be the case — surely no one would make claims about the Worry Window if trial data contradicted it, without at least acknowledging that data and claiming that it was likely fraudulent.
Fraudulent or not, the data was already published two years ago.1 First doses did not increase recorded infections in the trial; post-first-dose infections were not assigned the status “unvaccinated.”
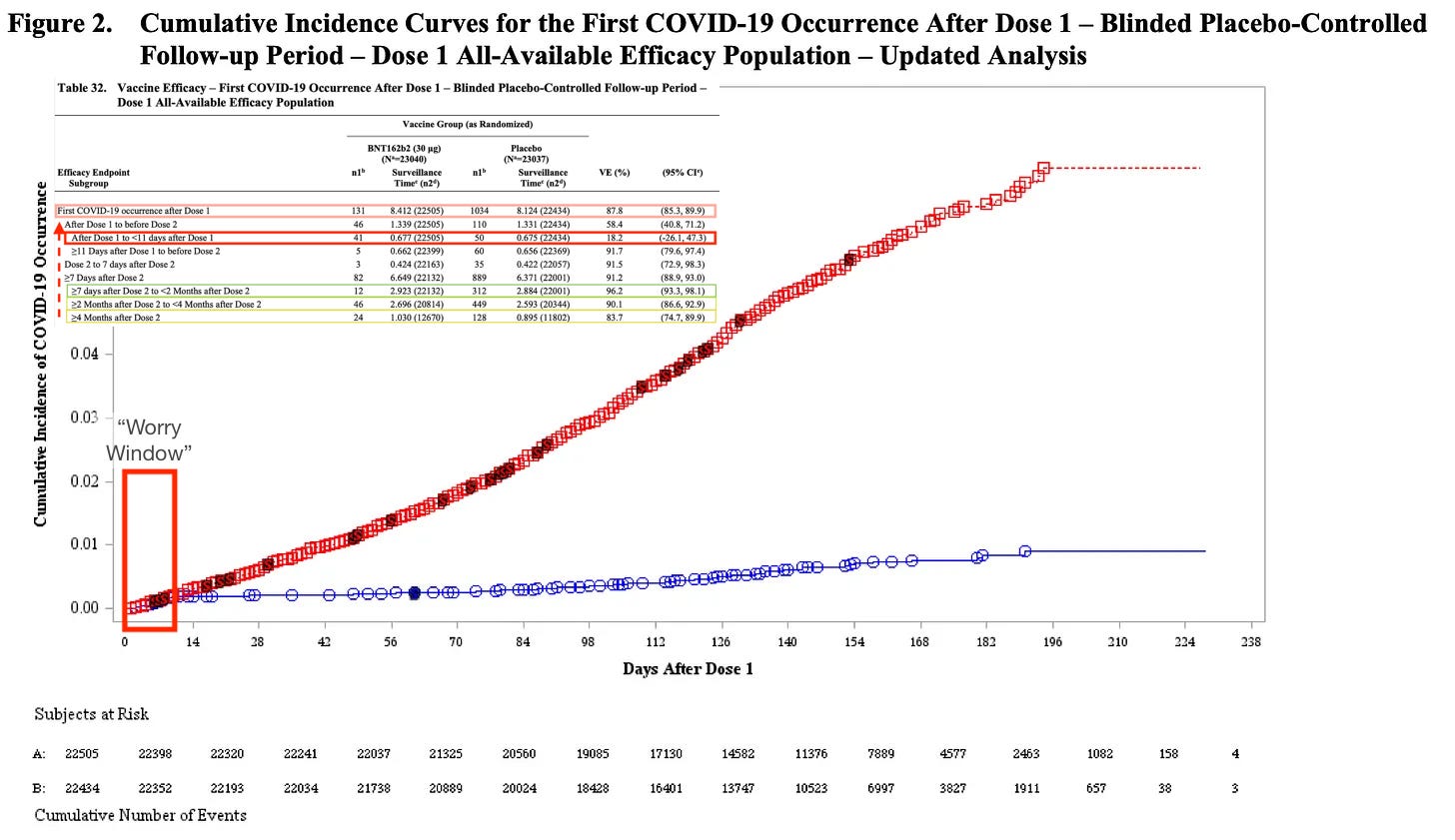
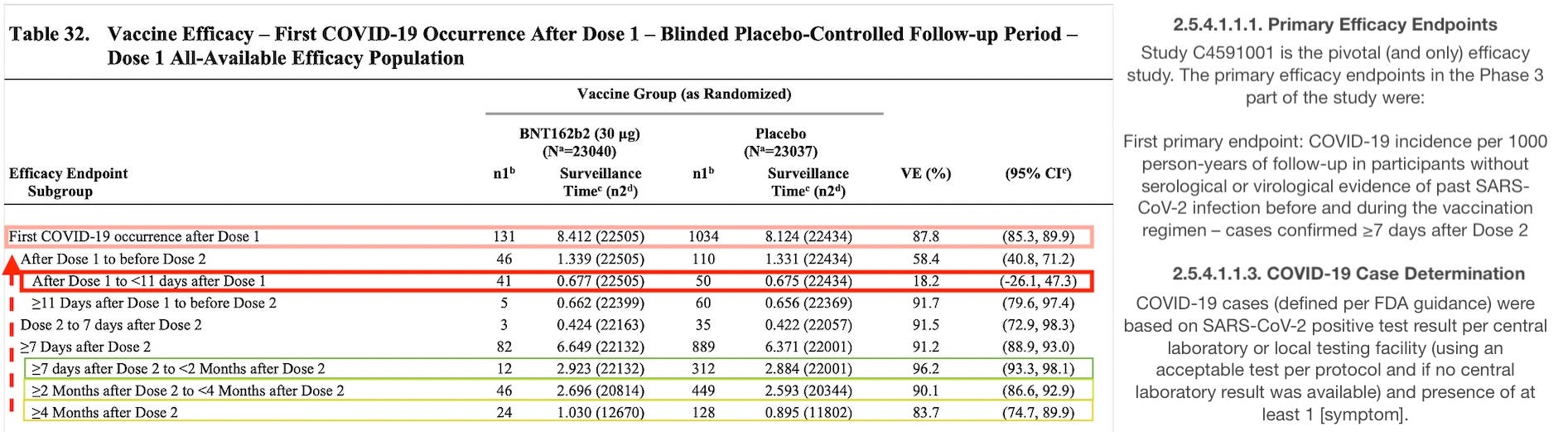
https://phmpt.org/wp-content/uploads/2021/12/STN-125742_0_0-Section-2.5-Clinical-Overview.pdf p. 54. With inset from p. 86. “Disease onset appears to track together for BNT162b2 and placebo until approximately 11 days after Dose 1 (consistent with the data shown in Table 32), at which point the curves diverge with cases steadily accumulating in the placebo group and remaining virtually flat in the BNT162b2 group. The darker-appearing symbols for both BNT162b2 (blue circles) and placebo (red squares) curves in Figure 2 have an “S” written inside the open symbol, which denotes severe cases.”
From the inset, we can see from this March, 2021 snapshot that 41 symptomatic, PCR-positive infections were recorded in the 11 days after receiving purportedly blinded experimental vaccine, vs. 50 after receiving blinded placebo. As a result, even if Pfizer had included all post-1st-dose “worry window” infections (highlighted in red), the sham trial was a lock for rushing the product that would fail after three months out of the door (failing efficacy is already evident in the transition from green to yellow):
More importantly, it’s not in fact the case that “hiding” these 41 post-1st-dose infections was the most “nefarious” available course of action. In order to rush the trial as much as possible, analyses were triggered when certain case counts were reached (94 for interim and 164 for final analysis), after the “fully vaccinated” timepoint. Including the earliest cases would have advanced that milestone, and still (it turns out) have delivered a win according to the statistical analysis.
However, Pfizer did not have the option of picking where to “start the clock” after-the-fact, and so chose an excessively late starting point — after the unnecessary 2nd dose. The most favorable choice would have been from day 12 after dose 1; but day 0 would have worked just fine.
They made this disadvantageous choice because, again, they had not done the work necessary to figure out how this product actually works in humans.
Or, Hahn and the FDA insisted on a late start to sabotage Trump’s reelection, consistent with their redundant (suspiciously perfectly redundant) choice of a half-participants-at-60-day "safety" threshold.2 Either way, starting 7 days after the 2nd dose delayed the release of the experimental poison with little difference in the flimsy, illusory infection efficacy that was only going to last a few months anyway.
iii. The “Suspected Covid-19” problem.
With official results of the perfunctory, sham trial addressed, now let us get to the more interesting question of whether those results are erroneous or fraudulent.
From here, this post will be structured around the evidence offered by “HART,” in the post “It gets worse before it gets better” from November 29, 2021. I believe this was authored by HART’s Clare Craig, as she has been active on the topic.
The original Pfizer trial stated that in the first week after vaccination there were 40% more cases of suspected covid in the vaccinated than in those given the placebo (409 vs 287). They make the claim:
“It is possible that the imbalance in suspected COVID-19 cases occurring in the 7 days post vaccination represents vaccine reactogenicity with symptoms that overlap with those of COVID-19.”
Of course they could have answered that question by ensuring that everyone with suspected covid was properly tested. In a separate submission they admit that 1 in 7 (699 people) who had suspected covid in the first 7 days after the second dose had no test result. They claim this number was small but there were only 910 positive test results over the course of the entire study. Why did they not ensure sufficient testing during this period?
The question here is whether the “Suspected Covid-19” issue is a result of definitions used during the trial, or an actual increase in infections that were missed in testing due to incompetence or deliberate imitation of incompetence.
Trial definitions mandate that at least one of the following symptoms plus a positive test constitute a confirmed case; thus at least one without a positive test would count as a “suspected” case.3
The list would clearly result in the Covid-vaccine group reporting “at least 1 symptom” as a result of side-effects from the experimental vaccine, in every case where they contacted their trial site as opposed to merely recording the same symptom in their “e-diary.”
The FDA’s comment that “It is possible that the imbalance in suspected COVID-19 cases occurring in the 7 days postvaccination represents vaccine reactogenicity with symptoms that overlap with those of COVID-19” is thus objectively plausible.
But could both side effects and true Worry Window Infections™ be at play here?
No, as I will show. It would have required deliberate suppression; but deliberate suppression would also have censored placebo infections.
First, there is no signal that 7-days-after “suspected” cases were less frequently tested.
The numbers on post-vaccine and overall “suspected” cases at the time of the EUA submission (November 20, 2020) were as follows:4
Reported symptom, no PCR-positive
7 days after injection:
Covid vaccines: 409 cases
Placebo: 287 cases
Any time:
Covid vaccines: 1,594
Placebo: 1,816
(Total: 3,410)
HART claims that “1 in 7” were not tested. This is based on values as they stood some months later, when there were an additional ~1,500 suspected cases. These values do not purport to represent first-7-days cases (they might; they might not):5
If first-7-day cases were overrepresented in “not swabbed,” then not-swabbed should reflect the extreme imbalance in first-7-day cases (more vaxxed).
As both groups have similar chances of not being tested or testing too early, the likelihood and circumstances of tests being missed appears to be the same for the “rush” of suspected cases after BNT162b2 injection as for any other time. It should also be kept in mind that sites recruited subjects on a rolling basis, so any “early gaps in testing” (which appear to have been rampant) would not have affected medium and late-trial recruits experiencing “worry window” infections after those early weeks. “First 7 days” did not fall on the same part of the calendar for everyone.
If “suspected Covid” cases at the time of the EUA submission were being driven by “worry window” infections, it would certainly be problematic that negative PCRs were returned for .88 x 409 = 360 of them.
Second, assuming that non-tested “suspected cases” were actual infections leads to the problem of “not testing” being more accurate than “testing.”
If the other 50 were non-tested true positives (implying 91 actual Worry Window Infections), in other words, it would be baffling how “reporting a symptom and not getting a test” proved a more accurate way of identifying an infection that “reporting a symptom and getting a test.”
“Getting a test assay”:
Sensitivity: 41/91 = 45%
Specificity:* 0/360 = 0%
“Not getting a test assay”:
Sensitivity: 50/91 = 55%
Specificity: 360/360= 100%
*Assuming none of the not tested were negative for infection.
At best, one could propose that no-test false negatives were as common as test true positives, i.e. that 11% or 5 to 6 of those ~50 no-test “suspected” cases were true infections.
Deliberate Test-Suppression Required
The accuracy of the “not getting a test assay” (under the assumption that more than 5 or 6 of the ~50 untested “Suspected Covid” cases were real infections) is mathematically problematic, if not impossible, under the assumption that actually being infected in the “worry window” would not make not-testing more likely (as opposed to a scenario where non-testing usually followed from random chance or discretion).
Only if we assume a deliberate attempt to not-test patently likely infections can we explain the accuracy of the “not getting a test assay” in somehow hiding 50 Worry Window Infections. Of course, there is a glaring problem here.
A deliberate attempt not to test likely infections would have also half-way hidden placebo group infections.
The combination of the assumption that the just-Covid-vaccinated had more real infections, but half or more of these were somehow not tested (only possible if blinded trial operators deliberately did not test apparent likely infections), leads unfortunately to the prediction that genuine placebo-group infections should have been “caught in the cross-fire.” There wouldn’t have been any way for trial operators, if they were trying not to test real infections, to know that the 50 symptomatic placebo-receivers with real infections should be tested.
It would thus either be the case that:
The placebo group, experiencing 50 infections, registered 25 infections immediately after the first dose. This is false; they registered 50 infections.
The real number of placebo infections was twice as high as 50. In which case the Covid vaccine did not actually increase infections (91 vax asserted vs. 100 placebo asserted “true” infections).
Lastly, if being injected with the experimental Covid vaccines increased the odds of an infection, resulting in a rush of “suspected Covid” cases that somehow were laser-targeted for not-testing, it would be strange that no severe outcomes resulted. Injecting RNA for spike protein should not protect against severe outcomes from immunosupression-mediated-contraction of infections (and if it did, I am not sure that is such a great argument against the injection).
(Note that this is true regardless of whether Worry Window Infections are ultra-precisely “hidden” by lack of testing, or if testing gaps are distributed randomly.)
Note, also, that for immediate infection efficacy and immediate severe efficacy to show up in a randomized trial, suggest that something beyond “Healthy user bias” explains why the “worry window” does not apply, and getting injected with the experimental Covid vaccine confers impossible immediate protection:
It keeps people home, by poisoning them so that they call out of work, etc.
The placebo, being unable to replicate this harm, does not immediately prevent infections.
It Is *OK* to Allege Outright Fraud
I am not here to defend Pfizer’s integrity. I openly endorse the following statements:
Pfizer could have committed outright fraud during the Covid vaccine trials, including by:
Simply excluding participants with adverse outcomes en masse (lopsided exclusion of Covid vaccine participants was blamed on the placebo injection not being affected by errors in storage or injection protocol6). This includes if said adverse outcome was an infection with SARS-CoV-2.
Miscategorizing Adverse Events by other means (stonewalling, downplaying, etc., as in the case of Maddie deGaray during the trial for teens7).
Just making up numbers. All the numbers could be made up!
Absent some sort of overt shenanigans, it is suspicious that overall “suspected Covid” cases were higher in the placebo group (unless this is the result of an extremely high false negative rate for SARS-CoV-2 infections, which is possible).
But these things are not what the Worry Window purveyors want to claim.
Instead, it is always that there’s some sneaky, but letter-of-the-law-complying shifting of windows and terms hiding in literally every study. The composite effect is that the Covid vaccines (and no other ones) are portrayed as some sort of serial criminal constantly eluding the hard-at-work detectives on a technicality.
“I did my best to put them behind bars for infection-increasing, but this no-good judge declared a mistrial!”
JUST CLAIM IT WAS FAKE. DON’T HIDE WHAT IT SAID WITH MATH.
If the Worry Window exists, there is no evidence for it. So at best it is an assumption without support in the data.
Part 2: A look at the “Look at the Waves” argument:
Participants who developed any potential COVID-19 symptoms listed in the protocol were to contact the site immediately and if confirmed to participate in an in-person or telehealth visit as soon as possible (optimally within 3 days of symptom onset, and at the latest 4 days after symptom resolution). At the visit (or prior to the visit, if a participant utilized a self-swab as permitted per protocol), investigators were to collect clinical information and results from local standard-of-care tests sufficient to confirm a COVID-19 diagnosis.
Investigators were to obtain a nasal swab (mid-turbinate) for testing at a central laboratory using a validated reverse transcription–polymerase chain reaction (RT-PCR) test (Cepheid; EUA200047/A001) to detect SARS-CoV-2. If the evaluation was conducted by telehealth, the participant was to self-collect a nasal swab and ship for assessment at the central laboratory. A local nucleic acid amplification test (NAAT) result was only acceptable if it met protocol-specified criteria and if a central laboratory result was not available, in which case a local NAAT result could be used if obtained using one of the following assays:
Cepheid Xpert Xpress SARS-CoV-2
Roche cobas SARS-CoV-2 real-time RT-PCR test (EUA200009/A001)
Evidence of prior SARS-CoV-2 infection were determined by virological testing via NAAT on mid-turbinate swab and serological testing for SARS-CoV-2 N-binding antibodies.
Case Definitions
COVID-19 cases (defined per FDA guidance)17 were based on SARS-CoV-2 positive test result per central laboratory or local testing facility (using an acceptable test per protocol and if no central laboratory result was available) and presence of at least 1 of the following:
There were 240 participants in the BNT162b2 group and 60 participants in the placebo group excluded for having important protocol deviations on or prior to 7 days after Dose 2. In the BNT162b2 group, most of these deviations were related to improper administration of the investigational product (203 participants, as compared with 23 participants in the placebo group). Specifically, in the BNT162b2 group most PDs were due to dosing/administration errors (errors in dilution of the vaccine, 76 participants) or administration of investigational product that was deemed not suitable for use (temperature excursions in shipment or storage at the distributor, 110 participants) that would have not applied to placebo [which cannot expire or be wrongly diluted].
1. They only tested those with COVID symptoms and the trial was technically unblinded because placebo was actually saline for the first time in vaccine history (or 2nd). Participants and trial staff could reasonably guess which they got based on severity adverse events . Those suspecting they did not got the real thing would be more likely to report COVID symptoms. Also those getting the real stuff probably needed pain relief for the AE which may have masked COVID symptoms.
2. Why do you think they didn't just give everyone a weekly PCR test. They couldn't afford it?
3. There are other studies showing an increase in infections after the first dose.
4. The vaccine in the trial was not the same as in the real world. They switched from circular DNA in the process for the trial to linear DNA in mass production and the final product had more truncated mRNA (which might be a good thing for safety but probably not efficacy)
5. Pfizer and Moderna both reported transient reduction in lymphocytes after any dose, and studies have shown that the early IgG antibodies after infection are afucosylated IgG which causes more serious COVID. This is why in almost every country that rolled out vaccines experienced a serious COVID outbreak with increased mortality right afterwards
6. We now know Pfizer covered up at least 2 serious AE, Maddie and that lady who came down with T-Cell Lymphoma after reporting a sore arm and swollen lymph node that required surgery. Both AE If reported might have put a halt on further authorizations but went down as stomach ache and sore arm and clear sailing ahead. Pfizer is a serial criminal offender and if it was a person it would be in prison. Instead it just pays fines that come out of shareholders dividends
I don't really think we need to worry about the Worry Window anymore since probably everyone has already been infected or vaccinated with 1 dose by now.
As to what effect IgG4 has on the chronically boosted, I am agnostic. Not really sure this is going to be a problem for most people although we need to see more data, especially for those boosting every 4-6 months
Heh, it’s this sort of sloppiness that drove me to scale down my reading of the skeptic community. Not actually sure sloppiness is even the right word… although I sort of suspect that’s how tales like this one start. Someone noting that the definition of vaccinated isn’t met until weeks after the jab, finding a study that uses the same definition, and eventually that just becomes the convention that has to apply to all the numbers, regardless of whether that’s true or not. And once the concept has been birthed, you’re not putting that cat back in the bag (to mix metaphors for NO reason at all).
It’d be amusing if it wasn’t so tragic. Accuracy is distant second to narrative strength and basically all sides of every argument operate in a similar fashion. I hate being so cynical, but it’s sort of my default setting and there’s rarely little reason to move me off of “if a sizable group of people believe it to be true, then it’s probably wrong.”











A few issues
1. They only tested those with COVID symptoms and the trial was technically unblinded because placebo was actually saline for the first time in vaccine history (or 2nd). Participants and trial staff could reasonably guess which they got based on severity adverse events . Those suspecting they did not got the real thing would be more likely to report COVID symptoms. Also those getting the real stuff probably needed pain relief for the AE which may have masked COVID symptoms.
2. Why do you think they didn't just give everyone a weekly PCR test. They couldn't afford it?
3. There are other studies showing an increase in infections after the first dose.
4. The vaccine in the trial was not the same as in the real world. They switched from circular DNA in the process for the trial to linear DNA in mass production and the final product had more truncated mRNA (which might be a good thing for safety but probably not efficacy)
5. Pfizer and Moderna both reported transient reduction in lymphocytes after any dose, and studies have shown that the early IgG antibodies after infection are afucosylated IgG which causes more serious COVID. This is why in almost every country that rolled out vaccines experienced a serious COVID outbreak with increased mortality right afterwards
6. We now know Pfizer covered up at least 2 serious AE, Maddie and that lady who came down with T-Cell Lymphoma after reporting a sore arm and swollen lymph node that required surgery. Both AE If reported might have put a halt on further authorizations but went down as stomach ache and sore arm and clear sailing ahead. Pfizer is a serial criminal offender and if it was a person it would be in prison. Instead it just pays fines that come out of shareholders dividends
I don't really think we need to worry about the Worry Window anymore since probably everyone has already been infected or vaccinated with 1 dose by now.
As to what effect IgG4 has on the chronically boosted, I am agnostic. Not really sure this is going to be a problem for most people although we need to see more data, especially for those boosting every 4-6 months
Heh, it’s this sort of sloppiness that drove me to scale down my reading of the skeptic community. Not actually sure sloppiness is even the right word… although I sort of suspect that’s how tales like this one start. Someone noting that the definition of vaccinated isn’t met until weeks after the jab, finding a study that uses the same definition, and eventually that just becomes the convention that has to apply to all the numbers, regardless of whether that’s true or not. And once the concept has been birthed, you’re not putting that cat back in the bag (to mix metaphors for NO reason at all).
It’d be amusing if it wasn’t so tragic. Accuracy is distant second to narrative strength and basically all sides of every argument operate in a similar fashion. I hate being so cynical, but it’s sort of my default setting and there’s rarely little reason to move me off of “if a sizable group of people believe it to be true, then it’s probably wrong.”