




Over at Injecting Freedom, Aaron Siri has posted an update on Public Health and Medical Professionals for Transparency’s legal battle to dislodge the FDA’s trove of documents related to the Pfizer Covid vaccine, which are currently non-available due to the agency’s incredibly reasonable 75-year paperwork collating timeline.

Siri further reveals that immediately preceding the Department of Justice case worker’s counter-brief in support of the earnest and quite unfairly harassed paper-collators in the FDA Freedom of Information Act office (ten souls in all - an eye-popping ~0% of the agency’s workforce!1), who as it happened couldn’t make it to court personally, out of concern for catching the virus supposedly fended off by the drug approved on the basis of the documents they need 75 years to release, several more backlogged documents were nonetheless published, including the FDA’s comprehensive Clinical Overview, a top-level summary of everything that was known and should have been publicly disclosed regarding the trial a year ago.

Highlights:
It’s readable!
Worry Window = Fake
The vaccine was never expected to prevent infection / transmission
Solicited Adverse Events widespread, Non-solicited AEs (serious outcomes) absent, Withdrawal circumstances unclear
Regarding the first point, much of what is presented in the Clinical Overview has already appeared in other trial documents, including the bewildering, official Pfizer Protocol.2 Likely an aggressive and talented investigator could have, or already has, already discovered almost all of rest (edit: in fact, the post-1st dose numbers were in the original NEJM publication of trial results; they merely haven’t been discussed or acknowledged much through this year!3). But readability makes a difference: The clear declaration of non-interest in (and non-expectation of) “infection efficacy,” and the intricate plotting of post 1st dose infections, are thus “news to me,” at least. These points, and the lack of revelations on adverse events, are what I will highlight below.
And for anyone who has long wanted to understand the Pfizer trial design for themselves, the first 30 pages of the Clinical Overview are an excellent document. Go get reading.4

What, Me Worry Window?
(Edit: As acknowledged in the disclaimer above, it turns out these values were already in the NEJM trial report the entire time!)
Pfizer’s reported vaccine efficacy has been shadow-boxed to oblivion, throughout the year, for only including results X days after the 2nd Dose (both 7 and 14 days were used, for separate outcome measurements). The censorship of infections occurring between the 1st Dose and the 7/14 days benchmark was taken as a clear signal of rampant infections due to vaccine-induced immune weakening. Why else would a corrupt, billion-dollar drug marketing company not reply to analyses posted by anonymous substack authors?! In reality, Pfizer’s mRNA transfection course performed exactly as should have been expected: Very little difference in the first 11 days, a bit of difference afterward (once antibodies could be expected to have been produced and absorbed into tissues where the virus might try to do its thing), with steady improvement up until the 7 and 14 days post-2nd dose cutoff.
Interestingly, the raw counts presented in the March follow-up analysis include infections missing from the December “final” analysis, for both BNT162b2 recipients and placebo - another clear demonstration of the gaps and inconsistencies in Pfizer’s vendor data collection last autumn.6 However, the post 1st-dose “worry window” vaccine efficacy in both renditions is decent.
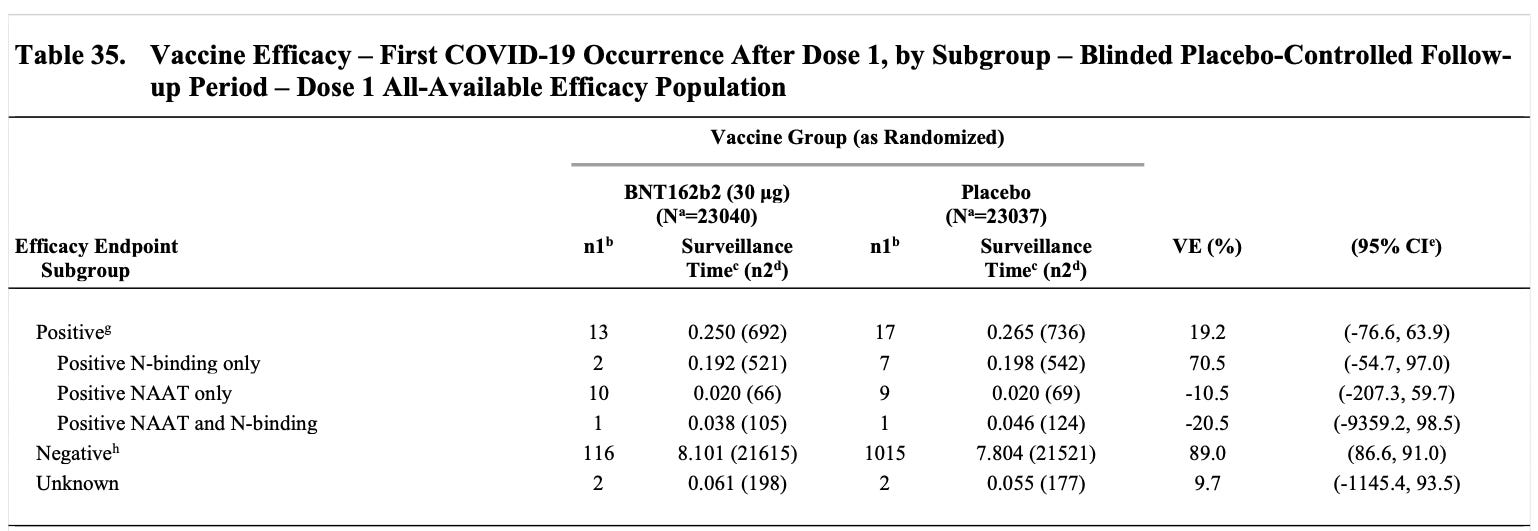
The raw counts, in the March “follow up” analysis, with associated VE values:

The plots, as of the same analysis:
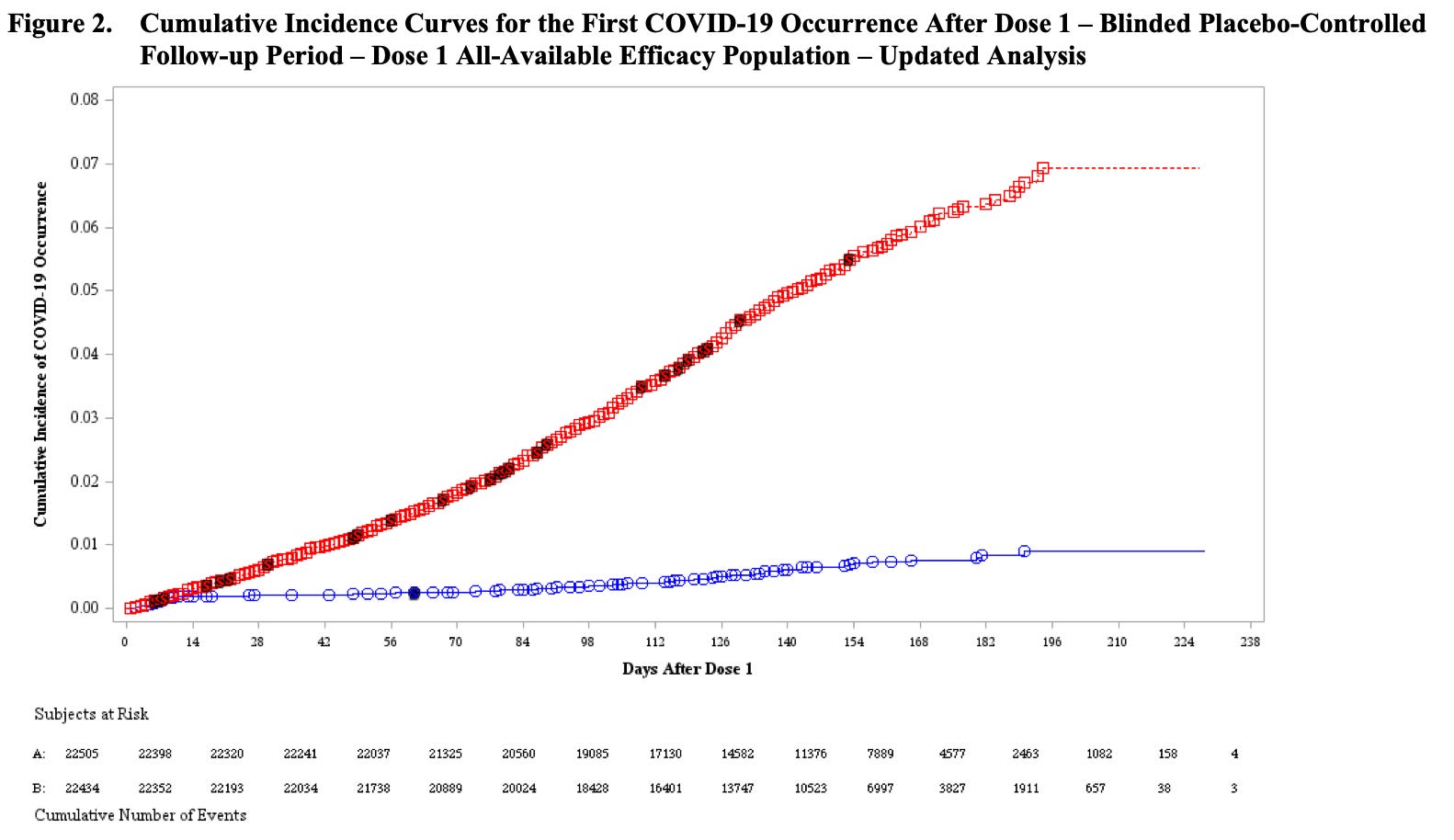
The dark “S”s are severe cases.
Note that subjects begin to drop off in droves after day 84, presumably after the unblinding leads to a reduction in the placebo group. All the values for BNT162b2 recipients after day 84 should probably be considered unreliable. However, our interest is in the first few days: The 1st-dosed do not experience a higher rate of infection. That’s because the innate immune system, and mucosal immunity in particular, does not actually just “check out,” by unspecified means, when offended by a novel antigen in the shoulder or bloodstream.
Should Pfizer have included all post-1st-dose infections in their initially published efficacy values? I’m really agnostic on this point. There were so many other reasons for any healthy person not to have taken an experimental vaccine against a highly survivable virus, that this legalistic quibbling over the 7 day cutoff seems to me to entirely miss the point (reasons including that duration of protection was openly impossible to know). Moreover, the overall “vaccine efficacy” if presented in December would have been 82%, rather than 95% - a difference which only matters in context of Pfizer’s competition with two other equally flawed, experimental drugs.
There is no scandal, here. The only early results (besides potential hundreds of unrecorded adverse events) that were truly worth “hiding” up until this point were, perhaps, the trial’s severe efficacy values. These could be considered misleading, given the low sample size - there was only one (FDA-defined) severe case of “Covid 19” among recipients - yet in fact this result proved the closest to the eventual real-world figure:7

A Sham from the Start
But just what is “vaccine efficacy”? Despite the assurances of Pfizer’s marketers in the Public Health Harem that these experimental drugs would prevent infection and transmission (until they wouldn’t), nothing of the sort was ever promised to the FDA.
The Clinical Overview documents that what would later become evident was already known by the FDA in December: Pfizer did not attempt to evaluate whether these vaccines stopped infection. From pages 28 & 29 (original emphasis replaced with my own):
2.5.4.1.1.1. Primary Efficacy Endpoints
Study C4591001 is the pivotal (and only) efficacy study. The primary efficacy endpoints in the Phase 3 part of the study were:
First primary endpoint: COVID-19 incidence per 1000 person-years of follow-up in participants without serological or virological evidence of past SARS-CoV-2 infection before and during the vaccination regimen – cases confirmed ≥7 days after Dose 2
Second primary endpoint: COVID-19 incidence per 1000 person-years of follow-up in participants with or without evidence of SARS-CoV-2 infection before and during the vaccination regimen – cases confirmed ≥7 days after Dose 2. […]
Case Definitions
COVID-19 cases (defined per FDA guidance) were based on SARS-CoV-2 positive test result per central laboratory or local testing facility (using an acceptable test per protocol and if no central laboratory result was available) and presence of at least 1 [symptom].
Positive tests in absence of symptoms were necessarily excluded - the study didn’t measure them. This was known by the FDA before the Emergency Use Authorization.
There was never any reason for the government to suppose, or suggest, that these vaccines would lead to mythical “Herd Immunity”, eradicate the virus, prevent eventual immune escape (incubated by constant asymptomatic transmission), or contribute to the safety of individuals who could not take them.9
Jury Duty
(For correction notice on this segment, see footnotes11)
Although the Clinical Overview provides a readable version of the trial design, it is obscurantist to the extreme with regards to Adverse Events. Two charts of participant counts feature bewildering changes to the participant pool, including between 240 - 302 BNT162b2 recipients removed for “protocol violations” sometime around the second dose (the count is only 240 in the March “follow-up” report):

Almost needless to say, the middle column is placebo. What were these “important deviations”? Page 79, in the “follow-up” section, defines “most” of them as incorrect and spoiled doses:
There were 240 participants in the BNT162b2 group and 60 participants in the placebo group excluded for having important protocol deviations on or prior to 7 days after Dose 2. In the BNT162b2 group, most of these deviations were related to improper administration of the investigational product (203 participants, as compared with 23 participants in the placebo group). Specifically, in the BNT162b2 group most PDs were due to dosing/administration errors (errors in dilution of the vaccine, 76 participants) or administration of investigational product that was deemed not suitable for use (temperature excursions in shipment or storage at the distributor, 110 participants) that would have not applied to placebo [which cannot expire or be wrongly diluted].
Since the Emergency Use Authorization, VAERS has reported seemingly thousands of incorrect doses thanks at least in part to Pfizer’s dilution scheme - including hundreds of wrong dilutions or accidental adult doses given to children aged 5-11 since November.12
The Clinical Overview demonstrates that the FDA was aware, at least by March, that not even the trial vendors could correctly execute Pfizer’s delivery procedure, even after having practiced on the 1st dose. Even “worse,” the rush-designed cold chain failed for .7% of BNT162b2 recipients, depending on what one is supposed to use as the correct denominator per the chart, suggesting they did not receive a viable product. Why didn’t this prompt any apparent pause or review of real-world procedures by Pfizer or the FDA?
(Because they do not care.)
These 203 “improper administrations” still leave a gap of almost 100 withdrawn recipients in the December “final” version. So what were these “important deviations”? Other documents may offer a clue, but the Clinical Overview seems unclear. Since the “follow up” portion lists fewer removals, perhaps some of these subjects were re-included in the eventual trial results, but with important outcomes potentially censored after they had been “processed.” Or perhaps the numbers in the December version accidentally double-count placebo recipients in the BNT162b2 group (302-52 = 250?) - another sign of excellence and fidelity in the trial data. And yet even if that is the case, 37 BNT162b2 recipients withdrawn “on or around the 2nd dose” seem unaccounted-for in March.
Meanwhile, seemingly 1000s of adverse event categories are catalogued in the Clinical Overview, with very low event counts recorded in almost all cases. Most conspicuously, cardiac events show little difference between BNT162b2 recipients and placebo. But the Pfizer trial, much like others, included almost none of these event categories in the rosy and innocent list of solicited outcomes that participants could self-report on their 7-day tracker profile; nor were they screened for during the bare-bones blood sample collection schedule. Participants could only have these extra categories of outcomes recorded into the trial through intervening trial administrators or doctors.13
Thus, all the strong signals in the event list merely echo the solicited symptoms. Still, the charts for solicited signals are surprisingly active, given the lower results obtained in the Phase 1 trials:

Overall, the adverse events portion of this document seems to reveal nothing about what actually happened to trial participants. In fact, it reports fewer events and deaths than the previous Pfizer leak.14

See https://www.fda.gov/about-fda/fda-basics/how-many-people-are-employed-fda-and-what-areas-do-they-work, which does not itemize the FOIA staff separately.
For previous discussion of the flaws in the trial design, including insufficient outcome monitoring, see “Perfunctory².”
Whereas the Pfizer Protocol document openly broadcasts that the trial was over-ambitious - too broad and too frequently-modified to have been executed with accuracy - and incredibly shallow in patient outcome measurement, the FDA’s Clinical Overview effectively disguises both flaws, by subtracting design elements removed by eventual amendment, and plotting thousands of AE event categories that the trial was not actually constructed to record.
Excellent, but still beguiling in respects. There is at least one moment of doublespeak in the trial description portion, for example. On page 18, “The structural elements of the vector backbones of BNT162 vaccines are optimized for prolonged and strong translation of the antigen-encoding RNA” is followed a few lines later by “RNA [in general] […] is transiently expressed,” both points listed as benefits to the platform. Here the Overview reveals the ad hoc nature of Pfizer’s eventual use of the pseudouridine-based candidate (see “Liquid Cancer”).
There are additional interesting tidbits and evasive segments, including reference to a “variant booster trial” (ongoing? called off?), a concrete description of the single reproductive toxicity assay (dosing a few rats for a few days and not reporting the raw results), and some galling assertions about how the vaccine both doesn’t need to and can’t be evaluated for pharmacokinetics:
2.5.3. Overview of Clinical Pharmacology
Pharmacokinetic studies are not usually required for vaccines. Measurement of the plasma concentration of the vaccine over time is not feasible.
Presumably they meant to write, “not favorable.”
As revealed by Ventavia whistle-blower Brook Jackson. See, again, “Perfunctory².”
Which highlights: Thacker, Paul. “Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial.” (2021, November 2.) The BMJ.
The “incomplete” worry window infections as counted in the December “final” analysis, with associated VE values:

Note that Pfizer used a case-count cutoff for their final analysis, under the reasoning that 164 cases (between both groups) was enough to satisfy statistical formulas that can magically vouch for reality if assumptions about reality are fed into them beforehand.
For Phase 2/3: the sample size assumed a true VE of 60% after the second dose of study intervention, for which a total of approximately 164 first confirmed COVID-19 illness cases would provide approximately 90% power. This would be achieved with 17,600 evaluable participants per group (or 21,999 vaccine recipients randomized in a 1:1 ratio with placebo) for a total sample size of 43,998. This assumed a 1.3% illness rate per year in the placebo group, accrual of 164 primary endpoint cases within 6 months, and 20% of the participants being non-evaluable or having serological evidence of prior infection with SARS-CoV-2 (potentially making them immune to further infection).
For this incredibly smart and good reason, the “final” analysis took place less than 2 months after the 2nd dose (as inferred by the 0-2 month infection counts in the “follow-up” analysis).
Here, note, that Pfizer only hoped for a statistical high certainty of a “Severe VE” of at least 30%. Due to the small sample size, they were not able to achieve this high certainty by the cutoff derived by their incredibly smart and good statistical assumptions. And yet in fact severe efficacy went on to at least appear to be 70% or so, even after infection efficacy dropped to 0 (as I have argued since August, based primarily on my inspection of the July outcomes in Israel; see “Midsummer Maladies”).
Additional graphs display post-1st-dose “case” counts by age, race, and prior “case” status. Although these are end-point VE values, and cannot isolate the “worry window” from the rest of the to-March “follow-up” period, they contain interesting data (they can further be compared with the corresponding post-2nd dose charts, to estimate “worry window” values; I may post these results in an update edit: preliminary math suggests that the elderly will show negative efficacy during the worry window, due to 0 placebo cases in the over 75 group!).
Elderly BNT162b2 recipients seem to fare well, from 1st dose to March:

Previously-NAAT positive BNT162b2 recipients seem to fare poorly (likely an artifact of small sample size); meanwhile N-antibody seropositive do just fine (suggesting no attenuation of natural immunity, only a discount on VE as the naturally immune in the placebo group are already well-protected):
(index link anchor)
Again, this may have already been essentially disclosed in previous FDA releases. It is only that the Clinical Overview is readable and coherent on this and other important details.
Here, again, matters are still a bit ambiguous, as it would turn out that “vaccine efficacy” was in fact a pretty good proxy for “infection (and transmission?) efficacy” in the real world - but only for a very short period after the 2nd dose. As infection efficacy seemingly drops to 0 after ~4 months, this distinction becomes irrelevant except in so far as it speaks to the state of mind of the Public Health Harem last winter.
(index link anchor)
The original version of this segment did not include the Overview’s explanation about expired/incorrect doses.
For mis-dosing of children, see “In Orphania.”
For earlier (adult) administration errors, see Crawford, Mathew. “Disturbing Details About Vaccine Adverse Events Reporting.” (2021, December 1.) Rounding the Earth.
See, again, “Perfunctory²,” and the testimony of Maddie de Garay and Brianne Dressen detailed in “And a Waste of Time.”
As mysteriously revealed on page 23 of https://www.fda.gov/media/151733/download (pdf)
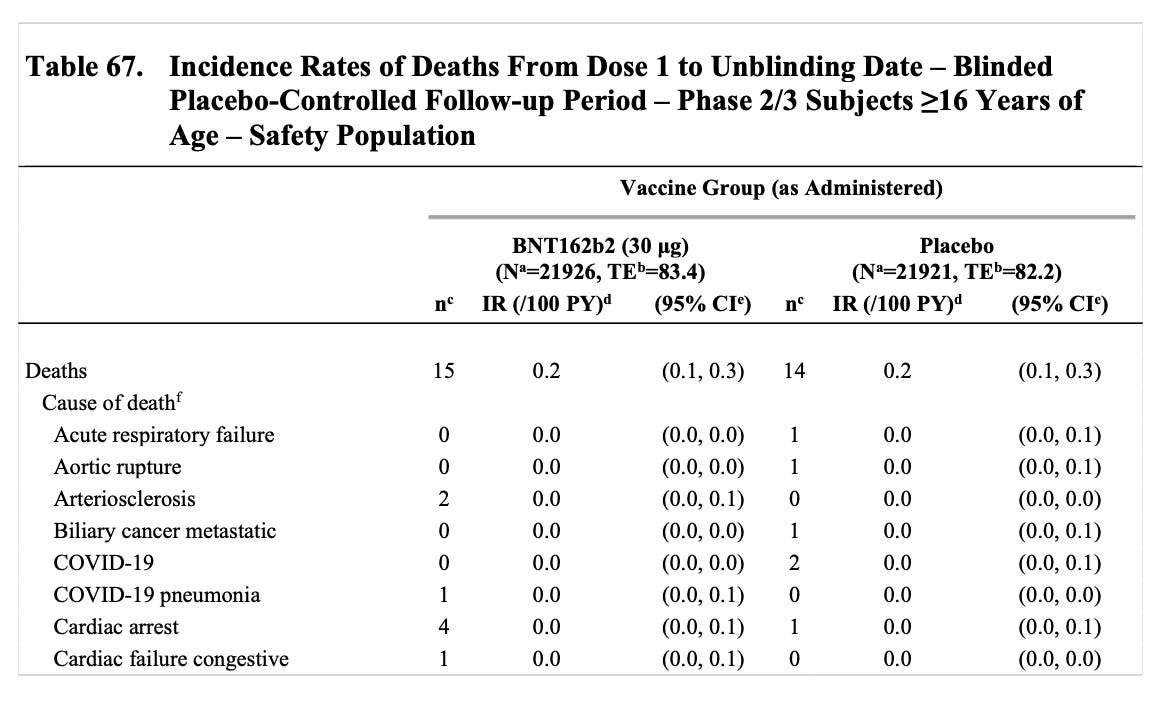
From Dose 1 through the March 13, 2021 data cutoff date, there were a total of 38 deaths, 21 in the COMIRNATY group and 17 in the placebo group. None of the deaths were considered related to vaccination.
The Clinical Overview only lists 15 and 14 deaths, respectively - the same numbers claimed by Pfizer in July - though it does include the disproportionate value for cardiac arrest reported elsewhere:
I keep replaying all of the lies that the people were told in my head. My stomach turns, considering that too many still believe those lies, even now. "Safe and effective", "Will prevent you from getting infected", "Will keep you from getting severe disease, hospitalization and/or death", "Vaccinated people cannot transmit the virus.", "This is a pandemic of the unvaccinated"... incompetence, greed, power, control, evil- I don't even care what the reasons are anymore. We are beyond any excuse for these companies, public health agencies, government leaders, local health authorities, school board directors, etc.
Pfizer without end: https://www.skirsch.com/covid/MoreHarm.pdf