
The third IgG4 / tolerance study, briefly
Delta vs. BA.2 "breakthrough" infections offer a glimpse of increasing tolerance in 2022.

Summary (click to expand):

The IgG4 story begins with Irrgang, et al, which will soon be a year old:

There isn’t much that can be added to Irrgang, et al. without a time machine. It shows the mRNA-vaccinated beginning to drift into an unknown territory — like the first few seconds of a car not left in park beginning to roll down a hill. Will it keep going? Will it crash?
Meanwhile, other studies have offered indirect answers to that question — new memory B Cells, which might possibly put the “brakes” on IgG4, do not arrive after breakthrough infection (reviewed here).
Eight months later, arrives a third preprint looking at IgG4 directly1 (the second was reviewed here):

i. Results vs. title
My goal is to briefly extract relevant information regarding IgG4 and present it to the reader. This will represent a different focus than that suggested by the title. Therefore, consider this unofficially a review of “the third IgG4 paper” with no discussion of the more complicated elements suggested by the official title.
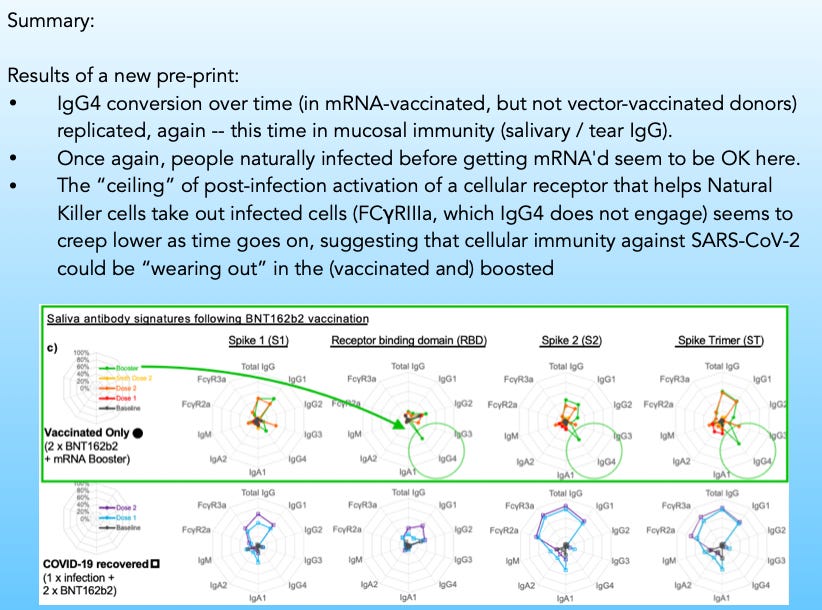
ii. IgG4 increasing after booster, in blood and in the mucosa.
Versus what is found after earlier doses, there is a sudden surge of IgG4 appearing after the booster. The way the results are presented does not allow confirming that this surge follows a slow trend of conversion in the months after the second dose, as with the prior two IgG4 papers:

iii. Non-mRNA first exposure does not lead to IgG4
This result is not reproduced in the group who started off with a vector vaccine (and then got an mRNA-based 3rd shot later):
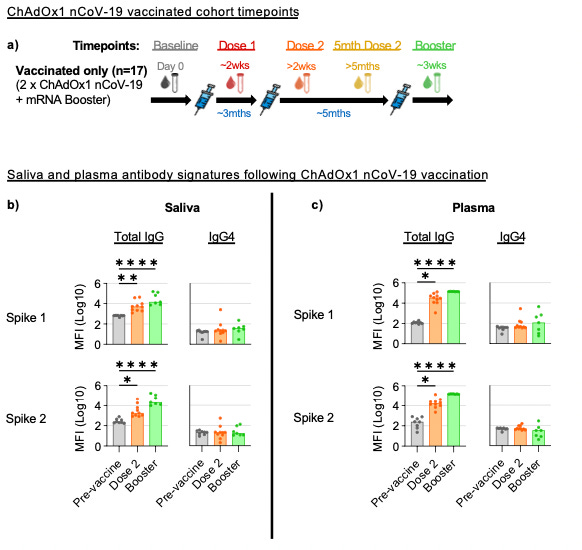
Nor is it reproduced in the previously infected plus double-injected; however, this group is not followed for a very great length of time. Still, nothing is offered to cast doubt on the results in Buhre, et al., that found previous infection protective against IgG4 conversion.2
Does IgG4 hinder cellular immune response? FC receptor-binding offers hints
Irrgang, et al. used an in vitro assay to show that post-booster blood with higher IgG4 wasn’t as good at prompting T Cells to kill cells in response to spike, vs. samples from the same donors after the 2nd dose.3
Selva, et al. offer a less direct glimpse into the same question by measuring how much antibodies against the spike protein (or parts of the same) are able to bind to the receptors that activate those cellular defenses, FCγRII and IIIa.
Serum antibodies don’t seem to lose FCγ-binding after the third dose, when compared to the second. Saliva antibodies, on the other hand, may show a bit of a drop, though primarily the difference that is noticeable is in comparison to the previously infected.

A bigger change appears when mRNA-vacinees who are infected with Delta after two doses are compared with those infected with BA.2 after three doses. Obviously, direct comparison is hazardous, since the variants may also influence immune response differently; additionally, the sample size for both groups is small.
Nonetheless, our two groups and their outcomes:

FCγRIIIa engagement starts out higher in spike-binding antibodies (however, this may simply reflect higher overall antibodies after the third dose) — but the additional increase prompted by infection is muted. Is this a sign that the “capacity” or “ceiling” for cellular immune response to the spike protein is being lowered?

Or is it merely an accident of the small sample size, and subtle differences in the variants and in sample timing? But if the former, my prediction for the potential consequences of the same remains as outlined in my “Tolerance and Severe Disease” series (not good).
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Selva, KJ. et al. “Lasting first impression: Pre-existing immunity restricts mucosal antibody responses during Omicron breakthrough.” medrxiv.org
Given all this tolerance being generated, it would almost seem as if they are preparing the populace, nay priming them for viral kill shots? Or perhaps create the most bestest necessary pharma medication merry-go-round evahh!
Or maybe they will admit / exclaim this phenom "Tolerance! Oh noes!!" and then offer the "solution", leading to...
I see a meme coming, "Vaccinate me harder, Daddy". Or perhaps due to rule 34, it's already been done.
Or do you think they are just that bleeding myopic and "new tech" gung-ho and profit-driven that the Ig4 conversion / tolerance was not on their radar, the horse has bolted, too late to close the gate, if we stop doing what we've been doing we'll essentially be admitting the mistake, so let's kick that effects can down the road and deal with it later?
ie do you think this is deliberate or just a run of the mill complete and utter cock up?
Are there any other precedents of over-medicating leading to a similar tolerance phenomenon? I mean, of course, outside the whole MRSA nightmare happening in hospitals and general pandemic of antibiotic resistance like, everywhere...