


The "Preliminary Findings" Paper
For Pregnant Covid Vaccine Recipients, the Divide Between Life and Loss Hinges on the Denominator

It’s not 82%.
Even a medical or research professional, however, could be forgiven for forming that impression when interpreting footnote “†” of Table 4 of the study titled “Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons” published late this spring at The New England Journal of Medicine website.1 In fact, some professionals did reach that conclusion, prompting a public letter to NEJM to “correct” the lower figure printed on the table itself. Rather than 12.6%, the letter alleged, it should say 82%.2 This disparity seems wildly egregious - but what does the figure represent? The incorrect, but easy-to-reach impression, is that it represents the percentage of under-20-weeks-pregnant Covid vaccine recipients who experienced miscarriage.
In fact, it does not represent this at all.
In this table, the percentage of study subjects of some category who experienced miscarriage at the time of publishing is listed as 12.6%. This value is the proportion of those 104 subjects within the entire population of subjects of that same category, numbering 827. But in footnote “†,” it is clarified that only 127 subjects in “the category numbering 827” received their Covid vaccine within the first two trimesters. As a miscarriage (the term used in medical literature is “spontaneous abortion”), must by definition occur within the first 20 weeks of pregnancy, the reader is left to conclude that the 700 subjects who were in their 3rd trimester must be excluded from the denominator in the table. This would mean that the correct definition of the proportion is 104/127: 82%.

The misapprehension stems from the self-defining nature of “the category numbering 827” employed by the authors, which is not clearly demarcated within the text of Table 4, and even remains elusive when the reader tries to add up the numbers or digest the complexities of the eight footnotes. The category numbering 827, is: All completed pregnancies.
Thus, Table 4 excludes all the pregnancies that were still ongoing at the time of the table’s creation. “All pregnancies that were still ongoing” includes all 1st-trimester pregnancies that did not experience termination.
That is the missing element of what would be the denominator necessary to produce the value which Table 4 is endeavoring to represent:
Spontaneous abortions / Subjects who were vaccinated within the first 20 weeks of pregnancy.
Instead, Table 4 actually represents:
Spontaneous abortions / All completed pregnancies at the time of table creation.
And, of course almost all of “All completed pregnancies” were vaccine recipients in their 3rd trimester: Successful pregnancies generally end when the 3rd trimester ends. Subtracting 3rd trimester vaccine recipients from Table 4 thus gets us no closer to the denominator we need, and thus neither 12.6% or 82% are the correct value for what Table 4 seems to be (but isn’t) saying.
This misapprehension is cemented by two corollary design choices featuring on Table 4. First is the title: “Pregnancy Loss and Neonatal Outcomes in Published Studies and V-safe Pregnancy Registry Participants.” This implies that the denominator delivered below is “in [all] V-safe Pregnancy Registry Participants.” However, it only represents the percentage of miscarriages within all completed pregnancies at the time of publishing, as we have just reviewed. The second misleading design choice is the side-by-side comparison of the 12.6% value with the normal range of pregnancies which end in miscarriage, a category which Table 4 pretentiously labels “Published Incidence” (this column is where the “Published Studies” in the title are located).
These two misleading choices and the bizarre footnote have garnered the Preliminary Findings report a status of infamy within hotspots of Covid vaccine skepticism, an infamy which extends by association to the mainstream press which - presumably because it would rather not bring up the question of reproductive health implications for the mRNA and vector Covid vaccines at all - has shown no interest in the controversy surrounding the paper. Preliminary Findings finds itself on the receiving end of many “outsider-whistleblower” Covid vaccine skepticism posts, and is currently the top result in Google for the phrase “preliminary findings” itself.3 Yet, the misleading choices which here seem at first to be hiding a scandal turn out instead to be suggesting a scandal where one does not quite exist. This puzzling outcome makes perfect sense if we assume a single, easily plausible explanation:
The study authors used a pre-existing template designed for fully completed pregnancy studies.
In a fully completed study, one in which by definition the category “pregnancies that were still ongoing” does not exist, the denominators “all completed pregnancies” and “all pregnancies” are interchangeable. Thus, the format on the right-hand column of Table 4 provides a valid construction to determine the percentage of each outcome within the total pool of participants - again, what the title of Table 4 suggests the table represents. In other words, we are seeing a table that was intended to include all participants being employed to only include the various participants who had for whatever reason “dropped out” of the running at the time of the report. It is further plausible to assume that the table is designed for a study in which the number of participants recruited after the first 20 weeks is negligible; otherwise, one presumes that a clear distinction would have been built into the construction of the value for proportion of miscarriages in the right-hand column. Only by granting these assumptions, does it make sense for the right-hand column to be compared with the value in the left, i.e. normal trends for miscarriage.4

Determining the Denominator
Reviewing the study in order to try to determine what the denominator in Table 4’s miscarriage figure should be turns out to be no easy task. Because the element of study design employed by the authors to generate Table 4 either presumes (because it is a generic template) that all subjects meet the standard for study inclusion upon inception, or simply failed to take the countervailing conditions of the study in mind during study design, participants who received Covid vaccination within the first 20 weeks of pregnancy are not singled out.
That presents a bit of a problem if the denominator we are interested in is, “participants who received Covid vaccination within the first 20 weeks of pregnancy.” Which… it is. As the definition for miscarriage employs the 20-week window, any comparison of post-vaccine miscarriage rates with normal trends must limit itself to those vaccine recipients who were still within the window.
Instead, the study divides subject vaccine timing almost exclusively by trimester. From Table 3, which outlays the demographics of the V-safe Pregnancy Registry subjects who make up Table 4 (the first two columns break down Pfizer and Moderna Covid vaccine recipients; the third is the total):
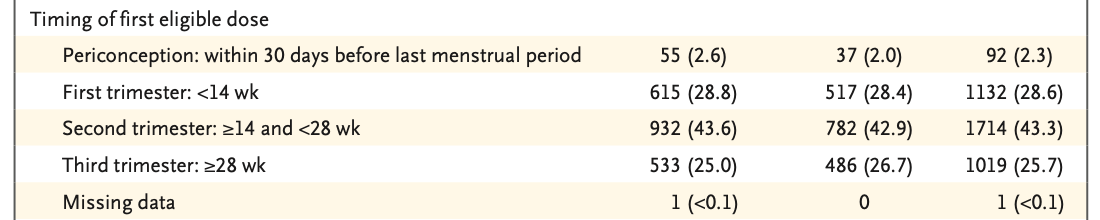
This forces us to estimate how many 2nd-trimester recipients were still within their first 20 weeks. The authors don’t plot specific reported weeks-along anywhere in the paper and appear not to have collected granular weeks-along data at all. (The process of the study, including “participant” selection, is detailed further below.) Thus, a proportional multiplier will have to do. The first six of the fourteen weeks of the 2nd trimester are within the 20-week statistical miscarriage risk window. Thus we can estimate how many 2nd-trimester participants were between weeks 14 and 19 when they received the Covid vaccine:
(6/14) x 1714 = 735
Adding these to the participants in the periconception (92) and 1st-trimester (1132) categories yields our provisional denominator: 1,959. This means that the reported rate of miscarriage at the time of publishing was:
104 / 1,959 = 5.3%
It turns out, however, that the authors provide a figure for reported miscarriages within the 1st trimester specifically: “A total of 96 of 104 spontaneous abortions (92.3%) occurred before 13 weeks of gestation.” While the percentage outcome for all participants who were vaccinated at any point within the first 20 weeks is still valuable, any amount of granular division of vaccination timing is far better at revealing how the timing affects outcome (or not).
Limiting results to participants who received the vaccine within the first 13 weeks of pregnancy (96 miscarriages out of 92 + 1132 participants) would yield a value of:
96 / 1,224 = 7.8%.
Both our estimated <20 week and our given <13 week cohorts compare excellently with normal trends of 10-25%. If they were to have made it out of the statistically ominous 20-week window with such results, their blessings would be legion. There’s just one problem: How many participants were still in their first 20 weeks at time of publishing?
The Preliminary Findings paper does not tell us.

Dissecting the Study
At this point, it is appropriate to pause to point out the abundance of authors who contributed to this amazingly superficial report. The byline is 21 names long:

It is initially difficult to ascertain whether primary data collection of participants used to form Table 4 was conducted by the authors themselves or the V-safe Pregnancy Registry team which recruited and collated the eligible “participants.” However, it is suggested from a comment within the Results section that, even with an army of talent at the helm, either the study or the Registry had fallen behind in observation and follow-up among 1st (and 2nd) trimester participants:

“Limited” may refer to the simple fact that a mid-study report necessarily excludes scheduled follow-ups that still lie in the future, or it may mean that of the scheduled follow-ups which had already elapsed, few had been completed. That is a big difference; yet the mere inclusion here and elsewhere in the study of such vague constructions of common English, impenetrable not because of their technical obscurity but because they fail to describe what happened in reality, bode poorly. The entire report comes off as either perfunctory or rushed. One wonders why it was released at all.
If the study was designed as a broad survey of medical outcomes, it seems pointless to have employed the V-safe registry: Based on the incompleteness of the Preliminary Findings report, it seems clear that a V-safe-based result will not functionally be complete any sooner than a totally post-hoc analysis of pregnancy outcomes conducted through normal methods of medical data harvesting. And if the study was designed for a more real-time appraisal of pregnancy outcomes, there was no need to target such a large pool of participants that even with 21 authors mining the data of the V-safe Pregnancy Registry task force, the authors were apparently overwhelmed. Surely a few hundred participants would be adequate to survey the v-safe pool.
In fact, neither of those flaws are quite the case: the authors’ method turns out to be merely accessing and processing the pool of Pregnancy Registry data available on March 30. Thus, the number of participants is not the problem. The authors are not overwhelmed; their report is premature - even for the standard one would imagine should apply to a “preliminary” report.
Step 1: The creation of the pool.
5During the timeframe from which the participants are gathered, the vaccines were primarily available and distributed to the elderly and to healthcare workers. Thus - just like in the study from Singapore - American female healthcare workers and their future children are the de facto substitutes for the reproductive health trials that the Covid vaccines were never subjected to before Emergency Use Authorization.
Some of the healthcare workers who received vaccines during early rollout self-registered in V-safe, a CDC app-based adverse event monitoring trash-can whose methodology is unimportant to the results in Table 4. What is relevant about V-safe is the Pregnancy Registry: App users who, in their registration survey, indicate that they are pregnant, receive a follow-up call from a V-safe commando team which seeks to enroll them into a more thorough and intimate adverse reaction monitoring regime. Here the study itself provides an adequately coherent description of reality:
For [women] who choose to enroll, the pregnancy registry telephone-based survey collects detailed information about the participant, including medical and obstetric history, pregnancy complications, birth outcomes...
As of the end of February, 35,691 V-safe app users had indicated that they were pregnant. By the end of March, the Pregnancy Registry team had attempted recruitment of 5,230 of those end-of-February pregnant V-safe app users, and 3,958 were successfully recruited. 3,719 of those recruits were healthcare workers. This is where the study enters the scene.
In fact, the 3,719 “participants” of “the study,” as framed above in accordance with the impression a reader would initially receive from the paper, are not actually involved in the study at all: They are the participants of the Pregnancy Registry follow-up pool, which is among the three separate 3rd-party data sets the authors used to create the Preliminary Findings report. The other two sources are the overall V-safe app results, and the tiny snapshot of pregnancy outcome reporting data in the crowd-sourced VAERS reporting system - both cutting off at the end of February. The first of these appears to provide the material which commands most of the authors’ under-the-hood effort: It is subjected to various statistical magic potions and construed into tidy charts. This forms the basis of the first two graphics in the report. Tables 3 and 4 are based on the Pregnancy Registry data pool. Table 3 is elaborate, but only concerns participant demographics. Table 4, displaying the outcomes of Registry participants, appears to be all but an afterthought to the authors.
The actual outcomes of pregnancy for pregnant recipients of a novel and experimental vaccine are seemingly regarded as of trivial consequence compared to the pressing question of “Did they report more chills than overall recipients? What about headaches?”
Step 2: There is no step 2.
Because the authors’ use of language can not be over-relied upon for any given point of fact, it is questionable to conclude decisively from their own methodology description that no follow-up data from after March 30 is included in the study. But as a thorough reading of the rest of the text provides no indication otherwise, this description of the methodology must be taken for its word.6
This, cross-referenced with the Pregnancy Registry follow-up schedule above, allows us to decode how many participants were still in their first 20 weeks, and how extensive the lag in reporting was at the time of publishing. Our premises thus far:
The Pregnancy Registry data included in Preliminary Findings cuts off at March 30, only 4.3 weeks after the end of the participant registration timeline (February 28).
Table 4 consists entirely of the analysis of the Pregnancy Registry data.
Pregnancy Registry follow-up is conducted on a 10-12 weeks schedule.
Thus the not-yet completed follow-up calls described by the paper are indeed calls that were still scheduled in the future as of March 30, and would have included the first follow up call for almost every 1st- and 2nd-trimester participant, which means for almost all Pregnancy Registry participants in the first 20 weeks.
What Table 4 shows, therefor, is not “pregnancy outcomes at the time the data was processed, on March 30” but “pregnancy outcomes (primarily) reported at the time of participant registration.”7
This still appears to function as a proxy for an observation window which extends beyond the immediate receipt of vaccination. The time-lag between vaccination, registration in the V-safe app, and initial enrollment in the Pregnancy Registry, appears to be several weeks for most recipients, even though the authors make no analysis to this effect. We can consider two approaches. From the Table 4 values and footnotes already quoted above, it is apparent that 700 of 1,019 3rd-trimester vaccine recipients had already concluded pregnancy when they were contacted and enrolled by the V-safe Registry for follow-up. Applying this ratio to the normal 13-week length of the 3rd trimester yields an upper bound for our approximate average registration delay of 9 weeks.8
On the other hand, if reporting of live birth is occurring after registration (but before scheduled follow-up), the 3rd-trimester birth / 3rd-trimester participant ratio is not informative. Simply using the difference between participant registration end-date and the time the data was accessed by the authors (4.3 weeks) might yield a better value, or splitting the difference between the two (~7 weeks).
Either way: Between vaccination, and registration, there is a window. Either way, it is not big. For the purposes of establishing a coherent impression of the outcome-experiences of Covid vaccine recipients in their first 20 weeks of pregnancy, it is utterly insufficient. Yet that is all that this report provides us.

Rushing to Judgement
The Preliminary Findings paper is certifiably a mess.
If, like we did with the Singapore syncytin-1 study, we imagine that Preliminary Findings was released with the deliberate intention of downplaying concerns about the reproductive health impacts of the vaccines, it differs from its sister-in-crime in that it doesn’t seem to have been initiated with that intention. And because the authors were not working from a premise that pregnancy outcomes would be the most interesting part of their report, they are entirely unprepared to present the outcome data in the misleadingly positive light cast by the stupendously early data-collection cutoff: Instead, they achieved the opposite, presenting the outcome data in manner which made the report appear to be nakedly attempting to disguise an outright catastrophe. Unlike the Singapore study, in which the astonishing observations are nimbly reframed by the authors as totally-not-astonishing, the Preliminary Findings report is so unable to change course from its initial broad and slow-paced design that it merely crashes onto the stage in a giant, smoldering heap.
9Yet had the report managed to reframe its data in a manner suitable to the apparent intentions of its early release, it would still constitute a document of malpractice and manipulation from conception to print. V-safe and VAERS are both ill-suited to the tasks for which they were created, because the problem of measuring the health impact of vaccines was never taken seriously by the CDC in advance of the Covid vaccination experiment. V-safe has no internal mechanism to correct for the selection biases inherent to any modern phone-based survey system; and VAERS has no policing mechanism to correct for incorrect or false reports on the one hand and missed reports on the other - at the moment, the system is completely overwhelmed with user-submitted Covid vaccine adverse reactions, as appear to be other similar resources like WHO-Uppsala’s VigiAccess site.
Two of the largest systems created to throw red flags when there is a signal of biological toxicity in a vaccine are both buried in their own output, which is now ironically being offered by anti-anti-vax-alarm-ists as a reason not to regard their output as being of significance (then why did we make the systems in the first place?). The authors certainly do not fail to acknowledge these limitations themselves. But so what? While compiling an analysis and overview of V-safe/VAERS results is a useful service, it is the province of public and private data hacks, not medical researchers.
A serious attempt to observe and understand pregnancy outcomes for Covid vaccine recipients would recruit subjects directly, establish a clear chain of custody for outcome measurement, and, most crucially, plot vaccine recipients according to granular weeks-along status at time of vaccination. A Preliminary Findings report of such a study would then clearly indicate how many participants were out-of and still-within the 20-week window before offering a provisional comparison to normal rates of miscarriage.
But there’s the rub: This study is not a serious attempt to observe and understand pregnancy outcomes for Covid vaccine recipients. No such serious attempt has yet been published.
While millions of citizens in America and elsewhere are subjected to a completely unprecedented gene-therapy experiment misleadingly labeled as a vaccine, the impacts to fertility and successful pregnancy remain an afterthought.10 The impacts weren’t measured before release. The public health apparatuses to measure the impacts after release are overwhelmed. And the medical research community is not equipped to measure the impacts in anything like real-time. This is true for every category of impact: But upon reproductive health, unlike the broader disease-focused obsessions of our healthcare system, the literal continuance of our species rests. Which is precisely the reason that no one still of child-bearing age should have been allowed to receive the vaccine at all.
Those who do receive it, in the end, sadly have no one to blame but themselves. A glaring blindspot existed in the legal barriers to selling an unproven and broadly untested medical intervention to the public at large, a blindspot with billions of dollars lying on the other end of it; Pfizer, Moderna, and Johnson & Johnson loudly announced their intentional passage through the blindspot, and the public at large happily slept-walked into their potential destruction.

11The Preliminary Findings authors do not attempt to read the minds of the V-safe Pregnancy Registry participants, but they do provide a review of why the CDC elected to issue guidance discouraging the withholding of the experimental Covid vaccines from pregnant recipients:
Pregnant persons were excluded from preauthorization clinical trials, and only limited human data on safety during pregnancy were available at the time of authorization. However, pregnant persons with Covid-19 are at increased risk for severe illness (e.g., resulting in admission to an intensive care unit, extracorporeal membrane oxygenation, or mechanical ventilation) and death, as compared with nonpregnant persons of reproductive age. Furthermore, pregnant persons with Covid-19 might be at increased risk for adverse pregnancy outcomes, such as preterm birth, as compared with pregnant persons without Covid-19. The Centers for Disease Control and Prevention (CDC) and ACIP, in collaboration with the American College of Obstetricians and Gynecologists and the American Academy of Pediatrics, have issued guidance indicating that Covid-19 vaccines should not be withheld from pregnant persons.
If this was the same calculus made within the minds of the healthcare workers who ended up in the V-safe pool, it reflects a tragic contortion of proper risk analysis.
12Regarding the “risk” of severe illness, finding oneself in a bracket that is statistically higher than the general (“nonpregnant”) population of reproductive-age Americans still leaves one in a very low-risk bracket. The only age group at significant risk from SARS-CoV-2 is and always has been the elderly.13 Presumably the health-care workers were, if not as likely to overestimate the risk of the virus as the common citizen, even more-so on average. To a brake shop owner, it seems that everyone’s brakes are overdue for repair: his shop does not get visits from the drivers whose brakes are not.14
Regarding the (entirely hypothetical) increased risk of pregnancy complications resulting from Covid-19, it must be remembered that an increased risk requires comparison with the baseline risk. If becoming ill during pregnancy in general is a risk, removing SARS-CoV-2 from the world with a finger-snap does not inherently lower the general risk of becoming ill during pregnancy and experiencing a complication in result. Whereas, receiving an experimental vaccine during pregnancy both (hypothetically) does not lower the general risk of becoming ill and adds the (hypothetical) risk of adverse outcome from the vaccine. While it is possible to model a hypothetical overall risk reduction effect from removing SARS-CoV-2 from the world, this model would need to be adjusted for the actual practical limits of Covid vaccine efficacy.15 Perhaps weighing this modeled risk-difference against the unknowable, but self-contained risk-addition of receiving an experimental medical intervention before any reproductive health trials have even been conducted on lab animals is a subjective matter, with reasonable estimations landing evenly on both sides of the equation. This journal opines that it is not, and that the CDC decision on guidance for pregnant women is egregious.
The haste, superficiality, and verbal confusion of the Preliminary Findings paper reveals that the authors have not yet actually “found” anything. But the reader, by observing this fact, may arrive at a finding of her own: The entirety of humanity is in the midst of leaping somewhere, and the looking can be expected to take place some time circa… 2023.

Shimabukuro, T., et. al., “Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons,” nejm.org. Note the aggressively political, cringe-inducing use of “Persons.”
As my understanding is that the letter has disappeared from the internet, I have not made any effort to validate this element of the story of the study’s reception; my account of the letter’s existence should thus be rated as a third-hand rumor. It’s a cute narrative intro, sue me.
“Preliminary Findings” would make a brilliant name for a science reporting substack, or a podcast. Perhaps it already is one - in which case, the creators’ feelings about the advancement of the NEJM study to the number 1 spot in search results must be mixed. As for this journal, it has sadly made its bed already and must lie in it.
Otherwise, if it is merely the table design created by the authors intended for the end of the study, it seems like the failure to build in a distinction between vaccine timing is sheer sloppiness.
For clarity, all outcomes included in the right-hand column of Table 4 are from the V-safe Pregnancy Registry pool. Although the title of Table 4 references other “Published Studies,” this refers exclusively to the values given for normal rates of outcomes in the left-hand column; no other studies of post- Covid vaccine pregnancy outcomes are included in the analysis on Table 4 (if indeed any have been published).
This interpretation may seem to provide the explanation for what the authors mean by the first part of “Among 1040 participants (91.9%) who received a vaccine in the first trimester and 1700 (99.2%) who received a vaccine in the second trimester, initial data had been collected and follow-up scheduled at designated time points approximately 10 to 12 weeks apart; limited follow-up calls had been made at the time of this analysis.” However, I take it to mean that 1040 and 1700 1st- and 2nd-trimester participants had completed the full process of enrollment which includes a second stage to schedule the future follow-ups, and thus not a representation of how many had yet to receive their first follow-up (which is estimated as almost all of them based solely on the 10-12 week schedule).
Here, we use a very crude assumption that 1/13 of any given 3rd-trimester cohort will experience birth on average on a given week.
(index link anchor)
“Nothing that is not a ‘vaccine’ can prompt the creation of antibodies, thus anything that prompts the creation of antibodies is a vaccine. Even pollen or shellfish.” - Instruction manual for the human body, apparently.
(index link anchor)
(index link anchor)
See “Provisional Death Counts for Coronavirus Disease 2019 (COVID-19),” cdc.gov. See also “Maternal and Infant Characteristics Among Women with Confirmed or Presumed Cases of Coronavirus Disease (COVID-19) During Pregnancy” at same, which describes birth outcomes (as opposed to patient outcomes). From Table III:

Testing positive “for Covid-19” (more accurately “for SARS-CoV-2”) seems to be associated with a very small increase in measurable late term adverse events, which itself may disappear if controlled for income (as suggested by the disparity in Medicaid as a source of payment). Meanwhile, infant survival appears completely unaffected (as suggested by the excluding-California value).
ICU admission, meanwhile, may be taken as a loose proxy for patient outcome. Currently at “Percentage of people with COVID-19 who were admitted to the ICU in the United States from January 22 to May 30, 2020, by age,” at statista.com, percentage of ICU-admission for all 30 to 39 year-old Covid-19 cases is .9, for all 20-29 year-olds is .5. The CDC’s “Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19) — United States, February 12–March 16, 2020” reports the values even higher.
The observed value of .8% ICU-admission for pregnant Covid-19 patients in Table III above therefore seems not to represent in any meaningful way an “increase” compared with their age group overall.
Actually, the owner of the shop were I bought new brakes two weeks ago says that he often sees unnecessary referrals.
22 V-safe Pregnancy Registry participants, or 0.55%, reported a diagnosis of Covid between their 1st dose and the time of their registration or most recent follow-up, which we calculated above to be ~7 weeks. Additionally, no antibody testing data is available or was collected by this report in order to form an estimation of (pre-pregnancy) post-infection natural immunity to SARS-CoV-2, which may be vastly higher for healthcare workers than the general population in this age group.