
Midsummer Maladies, S741E02: "Havens of Transparency"
Legible signals for drops in severe outcome efficacy in Israel and Scotland seem... not alarming (so far). But what about that 28-day deaths rate?

not only does the study suggest that being unvaccinated is associated with a higher likelihood of being reinfected, but "full vaccination is associated with reduced likelihood of reinfection" among those previously infected1


Although I am hard-a-work at my Grand Theory of Immune Equilibrium essay, aka the Herd Immunity Impossibility essay, which I promised to send to print this week, I felt as of yesterday that there were several good reasons to interrupt progress with another topical post. On the docket:
Israel Dashboard Adds Vaccination Status to Hospitalizations!
Scotland’s August 4 Infections But Not Hospitalization Update!
Scotland’s June 23 Post-Vaccination Deaths Update Non-error!

A Diversion to Kentucky!
THE DEBATE over vaccinating after prior infection is OVER! Ok?! You! Stop debating it! Now!
As I was finishing up this entry, a “Breaking News” alert from MedPage Today crashed into my inbox. The headline informed me that a newborn baby deity had been discovered within the Pantheon of Facts. By Deputy Managing Editor Molly Walker, the article, entitled “Debate Is Over: COVID Vax Doubled Protection for the Previously Infected,”3 calmly and prudently discusses a study posted to early-release today by the CDC. Just as one would expect.
Of course not.
Evidently composed from a template labeled “Deceptive Statistics-Mongering Sales Pitch,” the icon for which must be just a funnel serving 4000 pills into the mouth of a terrified “healthcare consumer,” the article only really sustains the hyperbole of the title in so far as it repeats the contained assertion four times in the first five paragraphs. It follows this opening recitation of hosannas - the intervening paragraph is an invocation of the terrible, demonic powers of Delta - with a barebones overview of the study in question; the incredibly redundant construction featured at the top of this post (“not only will you be at a higher risk if you don’t do this, you’ll be at a lower risk if you do!”); two paternalistic “just do it - for yourself!” quotes from a concurrent statement released by our unelected Disease Control Director; and lastly, a galling assertion that “epidemiologic studies among those previously infected have been lacking.”
Oh, have they?
Now, at times I feel that I don’t really understand what epidemiologists think it is that they are doing - no, in fact I always feel that - so to make sure I was interpreting Walker’s sentence correctly, I referred back to the official definition for “epidemiology” supplied by the CDC: “The study of the distribution and determinants of health-related states or events in specified populations.” Studies of the distribution of “health-related events” “among” the “specified population” of “those previously infected,” Walker therefor is asserting, “have been lacking.” But… but… no they haven’t!4
Perhaps “lacking” is being employed here as a polite euphemism for what such studies actually “have been,” which is ignored. Further, using the new Kentucky study to suggest that individuals who have already recovered from an infection should receive a Covid vaccine - non-debatable! - constitutes continuing to ignore them.
As regards the Kentucky study itself, I find it pretty limited, due to factors which are discussed in the footnotes below. Additionally, the title is soul-crushingly bureaucratic: “Reduced Risk of Reinfection with SARS-CoV-2 After COVID-19 Vaccination — Kentucky, May–June 2021.”5 One must pause to give thanks for alcohol, after ingesting a string of linguistic public health drudgery such as that. And… as long as our destination, rhetorically, is going to be Kentucky… certain “pairings” spring readily to mind.
But, sadly, our analysis must precede our therapy.
The authors looked at individuals with PCR/antigen test-confirmed infections in Kentucky’s National Electronic Disease Surveillance System in May and June who had previously been registered as a PCR/antigen test-confirmed infection in 2020.6 They then fabricated their “control group” into existence by randomly matching each test-confirmed reinfected individual to two individuals of the same age and sex who were confirmed infected in the same 7-day span (in 2020) as they. Once all 246 reinfected subjects, of whom 50 were vaccinated and 196 were not, had two “control” peers, the overall rate of vaccination among the reinfected (20%) and the control group (34%) were compared.7 From the study:

The use of date-matching hopefully partly corrects for any great difference in how unvaccinated an vaccinated previously-infected Kentuckians were behaving in May and June; the unvaccinated must surely be more on the less risk-averse, and therefor more active side than their vaccinated counterparts.8 So, we can provisionally accept the construction of the pseudo-control group, and move on.
Because math is evil, the observed results mean that 56 (and a half) more vaccinated Kentuckians (of the same age, sex, and prior infection week) would have had to score for a reinfection to reflect their share of the overall “control” population: these 56.5 Kentuckians were therefor “protected” by the Covid vaccines. To double-check our math, 56.5 more vaccinated reinfections would get us to:
(50+56.5)/(179+(39x(179/284))+50+56.5) = .343
Looks good. Thus Walker’s arrival to the vaunted, but nonsensical “Doubled Protection” claim (doubled… what protection?), and subsequent declaration of the end of all debate over taking an experimental drug which has not completed a single reproductive toxicity trial even if you have test-confirmed strong likelihood of natural immunity. Limits of the study are discussed in the footnotes,9 but let’s take the Kentucky results as having indeed divined reality, and delivered into existence a perfect, ideal Fact. Fine, great: “Double Protection, Non-Debatable!” What would that mean?
It would mean, the Covid vaccines only demonstrated 53% “infection efficacy” for previously-infected recipients in Kentucky.10
Therefor, previously-infected individuals should not receive the Covid vaccines.
It would mean, that if all of the approximately 260,000 Kentuckians11 who had recovered from an infection with SARS-CoV-2 in 2020 had been vaccinated, 110 more reinfections would have been “prevented” in May and June.12
For the remaining 259,840 Kentuckians whose post-infection natural immunity is what is actually protecting them from symptomatic reinfection - including for the 142 of them who would still be counted as reinfected despite vaccination in those two months - receiving the Covid vaccine will have done nothing at all for them (in those two months).13
(August 10: For correction notice on this section, see the bottom of footnote 9.)
While showing the math that leads to that result, we can extrapolate it to six months, to model the potential “booster” efficacy that Walker presumably would also arrive to herself, i.e. by projecting that triple-dosing might not actually prove less effective at preventing (re)infection. Because overall cases in May and June appear to have been low (20,396), we will use the July 1 to June 30 overall case rate to extrapolate to a six month exposure/prevention rate.
Kentucky yearly case rate:
Total cases on June 30, 2021 - Total cases on July 1, 2020
465,167 - 16,154 = 449,013
6-month exposure/prevention multiplier:
.5(449,013) / 20,396 = 11
In the footnotes, the possibility of significant false positives for “reinfections” is addressed. Overall, unvaccinated previously-infected Kentuckians (using the .577 rate of the synthetic age / sex / infection week profile constructed by the study as a proxy for actual overall unvaccinated rate) seem to have scored for infection at .255 the rate of all Kentuckians:
Unvaccinated reinfection rate (using “control”-type model) relative to general infection rate:
(179/(260,000 x .577)) / ((20,396-179)/(4,468,000-(260,000 x .577)) = .255
This is much higher than was observed in earlier population-wide reinfection studies: We could chalk this up to possible (asymmetrical) false positives; but I am comfortable acknowledging that gradual mild and asymptomatic reinfection should be expected, and is how immunity is supposed to work. The reader, however, is free to apply their own corresponding “likely false positive” discount to our simulation.
Using the observed reinfections, and the implied “prevented” reinfections, and applying the efficacy rate derived above (results rounded to nearest 1):
May and June potential “prevented” infections for previously infected recipients
.53 x (179+17+50+56.5) = 160
6-month potential “prevented” infections for previously infected recipients
(.53 x (179+17+50+56.5)) x 11 = 1,764
Not 1,764 severe infections. 1,764 mere (probably mild or asymptomatic, possibly false-positive) reinfections with SARS-CoV-2, “prevented” by 260,000 injections of an experimental drug.
Doubling our exposure/prevention multiplier, we can plot prevented reinfections gained by double-dosing a quarter million previously infected citizens in terms of days of average statewide infection per year:
Yearly prevented reinfections per 520,000 doses / (July 1 to June 30 infections in Kentucky / days in a year)
((.53 x (179+17+50+56.5)) x 22) / (449,013/365.25) = 2.86916
At a 53% “reinfection efficacy” rate, half a million doses of Covid vaccine delivered to a quarter-million previously infected individuals would save Kentucky a mind-bogglingly huge 2 days, 20 hours, 51 minutes, 35 and a half seconds-worth of total confirmed infections per year.

Israel Dashboard Adds Vaccination Status to Hospitalizations
But the signal for a change in trend for vaccinated severe outcomes looks… alright?
Israel’s lofty Ministers of Health have apparently tired of their hobby of delivering updates on hospitalization figures for the fully Covid-vaccinated via TV news reports that must be translated to the internet by Times of Israel online staff.15 Current hospitalization levels, as well as other vaccination-status-delineated stats, are now presented directly on the Ministry’s Covid-19 Data Dashboard.16 Since I am not on the Ministry mailing list, this change came to my attention via the recent post by Alex Berenson.17 However, I disagree rather strongly with his conclusions about how to interpret the newly available data. It is not clearly “bad,” nor clearly “getting [that much] worse.”
PCR-confirmed infections appear nearly as commonplace among Covid-vaccinated
At present, comparative rates of PCR-confirmed infection between the unvaccinated and the partially and fully vaccinated in Israel seem a bid muddled. Rates appear equal in the weeks before the “Delta wave,” only to recently diverge so that the vaccinated fair better than the unvaccinated. We will find a stronger, but equally variable signal of infection efficacy in the Scotland data below. Yet, Israel’s results should not be discounted. PCR-test positivity rate has only risen to 3.31% amid the Delta wave, which suggests a relatively robust level of screening-testing (the dashboard does not display the percentage of “cases” which are asymptomatic, as far as I can tell). First we may examine absolute case counts, bearing in mind that the Covid-vaccination rate in Israel is 55%. Because the dashboard buttons are sticky in Chrome, screenshots here are manually translated:
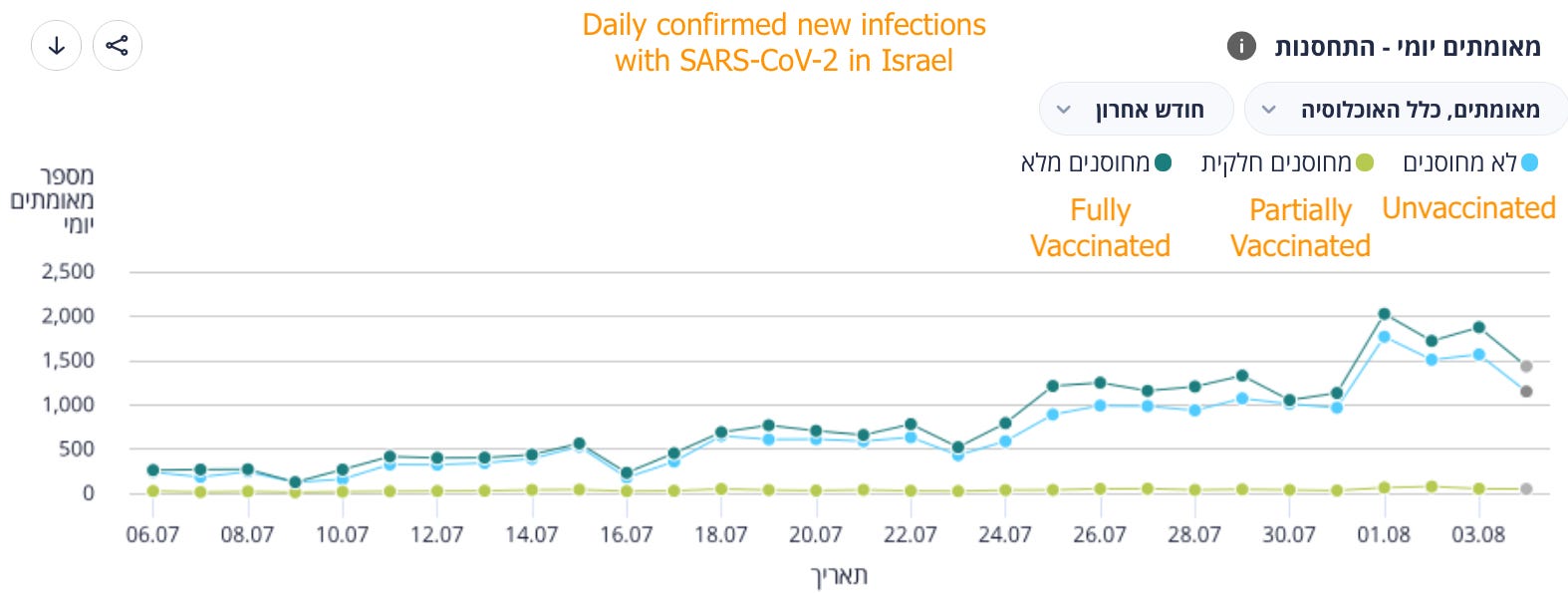
The actual rates of positive tests for both groups is also given in the dashboard, and nearly matches the absolute counts in appearance. Thus in Israel at least it is not true, nor apparently ever had been true, that the Covid vaccinated only appear to be PCR-confirmed infected nearly-as-often-as holdouts due to high rates of vaccination. Here I use the per-100k rates for individuals over 60, who have already exited the 180 day post- 2nd dose window in great numbers:18

So, here there is no downward trend in apparent Pfizer vaccination infection efficacy rate: Because it has been 0% all along. In fact, the higher sampling afforded by the Delta wave in the final weeks of this graph is the only thing that rescues it from such abysmal performance, resulting in an apparent ~35% efficacy rate in the August 3 snapshot (again, the results in Scotland below will be more favorable).
It is still possible that, because of the selection bias toward individuals who are symptomatic or otherwise seek out a test, there are more asymptomatic cases among the Covid-vaccinated than the unvaccinated. That, however, would merely reflect a positive signal in (mild or worse) outcome efficacy. The resulting signal for infection efficacy would turn out to be even more negative - perhaps bringing the rates into perfect alignment, indicating an apparent infection efficacy of 0%. But as the positive test rate in Israel, once again, is quite low, it seems safe to regard the Ministry’s given rates as a proxy for “infections with SARS-CoV-2.”
Of course, as rate of exposure always looms as the unmeasured “confounding factor” in any comparison in infection rates between two groups, apparent infection efficacy is not always real infection efficacy. Elderly Israelis who are unvaccinated may be disproportionately insulated from exposure. Younger Israelis who are Covid-vaccinated may be disproportionately exposed, potentially due to employment in the healthcare system. Both these things would skew unfavorably for the Covid vaccines, meaning the truth is not as bad as the observed result suggests.
Drop-off in severe outcome efficacy appears to have slowed, if not stalled
In our examination of the Ministry of Health’s quoted figures from June 24 and July 18, we found an alarming disparity in the change in absolute amount of hospitalization of the Covid-vaccinated, compared to the unvaccinated.19 But this signal seems to be more wobbly than appeared at first, and “severe illness” efficacy seems either to be holding or only falling slowly even as more individuals leave the 180-day window.
We can use the Ministry tables to compare apparent severe illness efficacy between July 18, where we had left off, and August 3. We will compare ongoing severely ill rates per 100K with PCR-confirmed 1-day infections per 100K from 10 days prior.20 Here, a disparity in rate of clearance from the hospital between Covid-un/vaccinated may be offered up front as a possible confounding factor. Additionally, PCR-confirmed positive cases are used as a proxy for “equal amounts of exposure risk” despite the aforementioned potential exposure confounding factor - once again, the low PCR-positivity rate permits such a gambit.
The formula is “Percentage “Prevented” Severe Illnesses Among Covid-Vaccinated per PCR-Confirmed Infection Compared to Unvaccinated.” Disclaimers: 1) Because I loathe this sort of relative “risk calculation” trickery, I am also very bad at it; my PCR+ daily snapshot ratio may be upside-down. 2) I am dismissing the industry-standard handicap of using custom math rather than infection rate to approximate exposure rate, since the debate at the moment is centered on, “What difference do the Covid vaccines make to outcome, given that they do not seem to prevent infection or spread?” 3) Results for partially Covid-vaccinated are ignored. Thus:
100-(100x(Rate of Severe Outcomes Vaccinated / Rate of Severe Outcomes Unvaccinated))
Thus, using an arbitrary ten-day delay for PCR confirmed infections daily rate and ongoing severe outcome patent rate:
100-(100 x (Ongoing severe rate / -10 day PCR+ daily rate snapshot) Vaccinated / (Ongoing severe rate / -10 day PCR+ daily rate snapshot) Unvaccinated))
What is revealed using this math is that vaccinated hospitalizations prevented per PCR-confirmed infection for over-60s has apparently degraded since the 18th, but not nearly at so fast a rate as might have been guessed from our calculations before. Additionally, the apparent efficacy has increased for patients under 60, despite the scarcity of vaccinated under-60 patients on July 18, thanks to a larger influx of unvaccinated under-60 patients:
July 18 apparent Covid vaccine severe outcomes efficacy for 60 and above:
100-(100x((3.1/6.1) / (10.2/3))) = 85%
August 3 apparent Covid vaccine severe outcomes efficacy for 60 and above:
100-(100x((10.7/12.7) / (48.5/16.6))) = 71%
July 18 apparent Covid vaccine severe outcomes efficacy for under 60:
100-(100x((.05/4.7) / (.2/6.9))) = 63%
August 3 apparent Covid vaccine severe outcomes efficacy for under 60:
100-(100x((.2/15.1) / (1/16.5))) = 78%
If we repeat this tabulation in another 16 days, we may have better evidence of a meaningful trend.
Scotland’s August 4 Infections But Not Hospitalization Update
Does Scotland offer a second real-time window into outcome efficacy? Not yet.
What Israel and the UK share, besides vertical geographic elongation and a fraught mother-daughter dynamic, is both an admirable forthrightness with Covid vaccine efficacy outcomes and a breathtakingly intrusive public health bureaucracy that seems to regard its own citizens essentially as well-behaved livestock.
So in the majestic backwater province of “Scott’s Land,” where the favored local pastime is performing “referendums” on independence as if the outcome will not merely be fabricated by the handlers feeding results into the gigantic, glossy displays under which the wiry suit-clad ambassadors of their overlords pirouette sensually,22 the fruit of both of these qualities is the stunningly comprehensive and publicly available “Public Health Scont’s Land COVID-19 Statistical Report.”23 Two of the billion diverse metrics tracked within this weekly-updated probe into the intimate nether-realms of the conquered hill-country subjects of The Crown™ are the ongoing rates of infections and hospital admission, by Covid-vaccination status!
Judging by this hidden gem of paradoxical autocratic transparency, both infection efficacy and “hospitalization efficacy” seem to have been improving until recent weeks, during the summer wave, and now waning. For infections:

It is an interesting graph. Most notably, “breakthrough” infections are not declining as aggressively as unvaccinated infections. But a finger-as-tape-measure estimate suggests that the recent fall-off of infection efficacy is more like a regression to the rates which preceded the recent wave of confirmed infections. Additionally, who knows what disparities there may be in exposure rates between the given cohorts, as well as how many within the 2 Dose group are “recent arrivals” who are “juicing up” the apparent efficacy value of the group as a whole. But as the “mysterious” reversal of the United Kingdom’s summer wave has stalled, if not itself reversed in recent days (no surprise, with the aggressive protests and the official reopening), this graph should continue to be worth watching.
As for hospital admissions, as always it must be kept in mind that the Covid-vaccinated are for the most part older. The Scotland report includes an all-ages hospital-admission rate, which resembles the curve above - but which tells us very little since the elderly are more vaccinated - and an age-delineated graph which uses absolute number of admissions, not rate. Meanwhile, Tables 15 and 16, which offer the previous four weeks of infection and hospitalization rates, are also not age-delineated. Still, future releases of the report may add this wanted feature. Watch this space, as the youngins say.
Overall, things seem not so bad on the outcomes efficacy front. If the prosecutors of Israel and Scotland, in this trial, are closing their case for convicting the Covid vaccines on the charge of “not causing antibody dependent enhancement,” the jury of reality seems impressed. And the past week’s-worth of expert alarmism that the Covid-vaccinated elderly all across the world are a triple-dose “booster” shot away from armageddon - and indeed, Israel has already rolled out boosters as of July 30 - might be entirely overblown. It seems the defense, for their part, will have to pull off a come-back, when court re-adjourns in the fall and the winter.24
Scotland’s June 23 Post-Vaccination Deaths Update Non-error
Oh my God! Did the Covid vaccines kill 1200 Scots?! (No.) Did they save 3000?! (Unclear.)
The Scotland weekly report also includes a very intriguing glimpse at a possible adverse-events signal among vaccine recipients. However, this figure has not been updated since the June 23 posting - and the update in question seems to have completely messed up the math.
Here, the given results in June 23, with “expected deaths” calculated based on figures from 2015-19:26
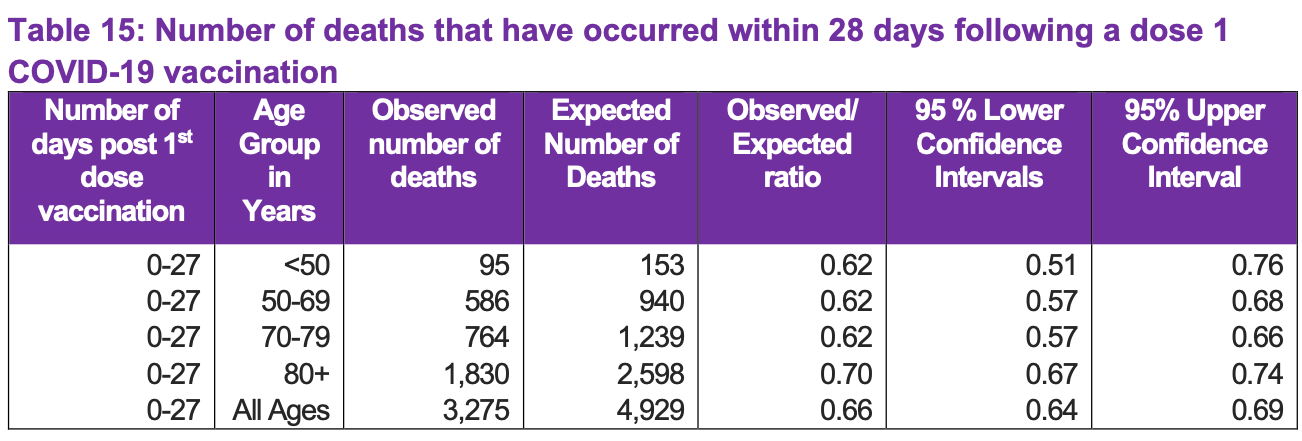

The “expected” figures, however, seem patently absurd, given that in mid-May, 28 days before the June 11 cutoff employed by the table, Scotland was only at 55% one dose- and 29% two doses-received.27 However, it turns out that they almost all seem to hold up.
First to approach things the wrong way: If we use National Records of Scotland figures to reconstruct an average 28-day deaths rate, we achieve:28
(57579+56728+57883+58503+58108) x (28/(5x365.25)) = 4,428
If we were to attack that figure with multipliers of .55 and .29 (plus a discounted add-on for individuals dosed in the following 28 days), we would arrive at the result that the All-Ages deaths for Covid vaccine recipients was roughly 600 souls higher than expected, for both doses! However, this would be eliding the disparity in the age of Scots who had received the vaccine by mid-May - precisely those groups which drive most of Scotland’s normal 28-day death rate. Using data from Public Health England, 29 Scots aged 70 and above were already at 90% Covid-vaccinated on May 4, rising thereafter to 97%. And statistics from the National Records of Scotland affirm, as would be expected, that these age groups are the primary drivers of mortality.30 Thus, a total reconstruction of Expected Deaths values for every age group is required. Great…
Now to approach things the correct way. To provide a simplified discount for in-progress post-dose windows, May 29 respective vaccination rates are employed for all vaccination-rate multipliers.
80+
Overall 28-day average death rate: (9,528+9,542+9,776+9,350+9,333+9,270+9,517+9,796+9,722+9,701+9,658+9,733+9,570+9,699+9,733) x (28/(5x365.25)) = 2,206
Through the first dose window expected: 2,206 x .981 = 2,164
Observed: 1,830
Through the second dose window expected: 2,206 x .944 = 2,082
Observed: 1,270
This corrects the outlandishly high First Dose Expected value used in the report (which seems to drive the corresponding over-the-top All-Ages value), but still leaves us with a miraculously aberrant real outcome for deaths after the Second Dose. This disparity far exceeds the normal monthly under-average resulting from the higher rates in the winter; and Scots over 80 had already reached 90% First Dose rates by the end of January, besides.31 No. It’s just not acceptable. Don’t these stupid geezers know they’re supposed to be dead?!
The authors chalk this up to the virological cycle - the 80 year-olds whose departures were due in April, when the 2nd-Dose rate surged from 50% to 90%, had got all their dying out of the way in the winter wave of infections with SARS-CoV-2. We can grant this explanation, absent any means of assessing whether death reports from April are simply backlogged. If so, it means that the “expected” rate for 80+ should be vastly discounted in some impossible-to-assess manner, and how the real rate compares to the correct expected rate is in fact unknowable.
Alternately, approximately 1000 Scots over 80 contracted SARS-CoV-2 in the weeks after their first dose, were thus excluded from a 2nd dose, and died after the 1st Dose 28-day mark. This, however, merely slots in with the “lag in reporting” speculation: It leaves us with no grounds to say what the “real 2nd dose expected deaths” figure should have been.
Moving on. Here, May 29 average vaccination rates for 70-74 and 75-79 year-olds are employed, without any weighting for population (the rates were virtually identical anyway):
70-79
Overall 28-day average death rate: (6,021+7,745+5,818+7,462+6,039+7,856+6,297+7,810+6,238+7,605) x (28/(5x365.25)) = 1,056
Through the first dose window expected: 1,056 x .997 = 1,052
Observed: 764
Through the second dose window expected: 1,056 x .997 = 1,052
Observed: 585
Again, an apparent post-carnage miracle or possible lag in the data, both implying that the expected value should actually be somehow discounted.
For the next set we will examine, discrete vaccination progress multipliers for each 5-year group are required.
50-69
Through the first dose window expected: (((1,623+1,699+1,669+1,702+1,647) x .949) + ((2,233+2,302+2,256+2,351+2,291) x .975) + ((2,975+3,082+3,075+3,165+3,233) x .999) + ((4,770+4,767+4,490+4,462+4,369) x .995)) x (28/(5x365.25)) = 879
Observed: 586
Through the second dose window expected: (((1,623+1,699+1,669+1,702+1,647) x .38) + ((2,233+2,302+2,256+2,351+2,291) x .498) + ((2,975+3,082+3,075+3,165+3,233) x .725) + ((4,770+4,767+4,490+4,462+4,369) x .957)) x (28/(5x365.25)) = 644
Observed: 365
Again, we have affirmed the authors’ math - and again, observed rates of death are vastly below trend to such an extent that the “expected” values must essentially be thrown out the window. And without a knowable adjusted expected value, we can make no plausible claim that there either is or is not a signal of deaths as an adverse reaction to the Covid vaccines.
And if, once again, this is not an error, or a macabre artifact of post-1st-Dose infections that led to deaths after the 28-day window, it additionally suggests that a rapid correction to the winter excess deaths values is in store, at least for Scotland (arriving at this conclusion is why I have gone through the trouble of checking the math only to affirm what the report already says).
Thus SARS-CoV-2, these results suggest (and common sense dictates), is nothing more than a ripple of stress passing over the surface of human life, primarily displacing those who are already at its margin, mid-exit. Despite Scotland’s rapidly aging (and only barely growing) population, 2020 was only the 3rd highest for absolute deaths since 1980. To complement this self-contradicting memento mori, we may close with a screen-grab of the Scotland mortality statistics used to complete our otherwise pointless verification of the report’s figures. Bagpipes not included:



Walker, Molly. “Debate Is Over: COVID Vax Doubled Protection for the Previously Infected.” (2021 August 6.) MedPage Today.
ibid.
See, of course, The Natural Immunity Illusion Illusion, Part 1.
Cavanaugh, A. et al. “Reduced Risk of Reinfection with SARS-CoV-2 After COVID-19 Vaccination — Kentucky, May–June 2021.” cdc.gov
The study text describes the test types used for confirmation of infection in NEDSS as NAAT (presumably almost all PCRs) or antigen test.
That sounds like science to me!
Thus, if the study is successfully correcting for behavior patterns, a true random sample of Covid vaccination rates among individuals in the NEDSS 2020 cohort might have come out much higher than 34%.
Overall, the authors are careful in their presentation of the data - they conclude that their results only “imply” that the previously-infected should be “offered” the Covid vaccine, not have it shoved down their throat (well, shoulder tissue) sans any debate - and are somewhat thorough in pointing out the study’s significant limitations. From the Discussion section (emphasis added):
Third, vaccine doses administered at federal or out-of-state sites are not typically entered in KYIR, so vaccination data are possibly missing for some persons in these analyses… Because case investigations include questions regarding vaccination, and KYIR might be updated during the case investigation process, vaccination data might be more likely to be missing for controls. Thus, the OR might be even more favorable for vaccination. Fourth, although case-patients and controls were matched based on age, sex, and date of initial infection, other unknown confounders might be present. Finally, this is a retrospective study design using data from a single state during a 2-month period; therefore, these findings cannot be used to infer causation.
I see no reason to disagree with their estimation that relative vaccination rate likely skewed higher among those who were contacted by NEDSS, i.e. the case/patient group - thus, an equally accurate control vaccination rate might prove to be higher.
However, in mentioning that the pseudo-control might not actually be a perfect match for the case/patient cohort, the study neglects the more important problem: The study has no means of determining different risk profiles among the previously infected. To put it simply, revealing the “infection efficacy” within the pseudo-control population is not the same as revealing the infection efficacy for all previously infected individuals. Removing the selection bias of only looking at the reinfected would be necessary to ascertain an efficacy rate that applies to all previously infected as a whole. Thus, the use of the word “control” for such reverse-fabricated statistical apparitions is not very appropriate, and elides the study’s built-in bias. So, it’s a good thing that “control” isn’t in the name of this category of study design, so that the results can be used to manipulate lay readers into imagining drugs work when they do not. (It is in the name.)
Even more importantly, the authors missed mentioning the potential sampling error of a high false-positivity rate among reinfections!
Because reinfections are rarer, they implicitly have a higher false positivity rate than original infections.
In NIII Part 1, we concluded that positive PCR-testing seems to operate in practice as a proxy for infection, in that individuals who score positive are unlikely to score positive again later (after 90 days post-resolution of symptoms). A high-level of screening-testing might reduce this correlation, but some screening testing seems not to make too much trouble (based on the Shrestha, N. et al. “Necessity” study). In short, we concluded that the PCR-test false positivity rate is not actually that high in most (non-high-screening) contexts. However, this goes out the window if we are examining positive tests among the previously infected.
Again, because math is evil, the rareness of an outcome increases the rate at which positive measurements of the outcome observed by an otherwise “accurate” testing method are false, especially if the test method is applied in a random or screening basis (this is called the “Bayesian Boogaloo Effect”). In the Lumley, S. et al. “OUH” study, for example, we observed that 1 of the 3 “PCR-confirmed reinfections” was a clear false positive. A higher false-positive PCR-test rate can be expected both among previously infected Kentuckians who were screening-tested, and who showed up for a test due to a cough or a colleague’s positive test (though probably not for PCR-tests prompted by more severe symptoms; however, who even says there were any such outcomes among the “reinfected”?).
When comparing outcomes between the previously infected and not, this false positivity rate is not such a problem - it is a handicap, in fact, which only favors rating the results for the previously infected as possibly even better than they appear. When comparing outcomes between two groups of previously infected individuals, it means you possibly or probably are not measuring the outcomes that you seek to compare very accurately. Without a more thorough system of real-time follow-up-testing to verify all individuals within the case/patient group as actual “reinfections” - impossible in a study that, by design, used another agency’s data rather than putting feet on the ground - this potential noise rate casts a shadow of doubt over any “reinfection group comparison” study.
Further, antigen testing might have lead to an even higher rate of false “reinfection” than PCR-testing. The authors’ text explicitly states that antigen-test-confirmed “reinfections” within the NEDSS data were not excluded:
A case-patient was defined as a Kentucky resident with laboratory-confirmed SARS-CoV-2 infection in 2020 and a subsequent positive NAAT or antigen test result during May 1–June 30, 2021.
Correction added on August 10: An earlier version of this section of the essay, as well as this footnote, was based on an incorrect reading of the description of the NEDSS criteria for positive cases. Namely, I read “antigen test” as “antibody test!” The significance, in terms of potential false-positives, of NEDSS including antigen tests might still be moderate or high. I haven’t done much reading into antigen tests, since few studies include them; but conveniently, another recent MedPage Today article potentially sheds some light. See: Gever, J. “Roche, Abbott COVID Antigen Tests Just So-So in Real-World Data.” (2021 August 09.) MedPage Today.
Testing 10,000 asymptomatic individuals from a population with less COVID-19 prevalence -- 0.5% -- would give 34 false negatives, but a higher rate of false positives (18 in all, or more than one-quarter of all positive results).
Eight days ago, you would think this would be the headline. As of seven days ago, apparently the prevailing attitude is, “Yowzer! It’s not zero!”
The study excluded results for individuals under 18. If there were any reinfections for under-18 Kentuckians in May and June, all the subsequent “prevented” reinfection results would scale up accordingly. The reader may add a 1.25 multiplier, for example, to arrive at an estimated adjusted value.
We may ponder, for example, what the 50 individuals who were counted as reinfected despite vaccination in the Kentucky study must think of the - Non-Debatable! - news that the odds of the vaccine “protecting” them were only 53/47 to begin with.
(index link anchor)
An overview and analysis of the Ministry of Health updates on June 24 and July 18 was provided in the opening of NIII, Part 2.
See Berenson, Alex. “Quick update on the Israeli vaccine data.” (2021 August 3.) Unreported Truths.
The chart for under-60s resembles the above.

Confidence in the Ministry of Health’s calculations for the per-100,000k rates was established using given values for over-60s on August 3. I used 1,424,490 for the overall population over 60 based on https://knoema.com/atlas/Israel/topics/Demographics/Age/Population-aged-50-years, and used crude values of 90% for Vaccinated, 6% for Unvaccinated, and 4% for Partially Vaccinated among the overall population. This led to consistently similar results among fully vaccinated and unvaccinated groups for both the PCR-confirmed new infections chart and the “Severely ill” chart:
August 3 60+ PCR-confirmed new cases per 100k
Fully Vaccinated Expected: 100000x(379/(1,424,490x.9)) = 29.56
Listed: 28.8
Partially Vaccinated Expected: 100000x(2/(1,424,490x.04)) = 3.5
Listed: 8.9
Unvaccinated Expected: 100000x(52/(1,424,490x.06)) = 60.84
Listed: 56.1
August 3 60+ “Severely ill” per 100k
Fully Vaccinated Expected: 100000x(140/(1,424,490x.9)) = 10.92
Listed: 10.7
Partially Vaccinated Expected: 100000x(6/(1,424,490x.04)) = 10.53
Listed: 26.8*
Unvaccinated Expected: 100000x(45/(1,424,490x.06)) = 52.7
Listed: 48.5
*Since partial vaccination is a transitional state, patients who enter the category of (infected or) “serious patient” in that state are possibly frozen in that category until they are discharged, even if they would have otherwise elapsed into the fully vaccinated category by now.
See footnote 15.
The dashboard defines “severely ill,” I am almost certain, as hospitalization. Estimates for the number of days between positive test and severe illness were higher in most of the early research from spring of 2020. Few recent studies seem to provide an estimate for the intervals that obtain today. I chose 10 days, as most healthcare systems are no longer postponing hospitalization for all patients as was done in spring 2020, and as neither of the resulting values appeared off-trend.
(index link anchor)
See “Scottish referendum: How will the result be decided? BBC News.” youtube.com
For latest version, see “COVID-19 statistical report.” Or, see August 4 permalink. publichealthscotland.scot
The maligned-from-all-corners-for-causing-dissonance-in-the-narrative WHO, therefor, here might once again have struck on the Least Stupid And Therefor Most Harmful Expert Advisory Position with their recent recommendation that antibody top-up “boosters” be postponed in the West until September, so that other nations can get more of their citizens in on the mass experiment first.
(index link anchor)
This via the Our World in Data figures visualized by a Google search for “Covid Scotland stats.”
Deaths attributed to Covid 19 peaked (very roundly) in mid to late January; presumably, these patients were diagnosed before receipt of the Covid vaccine and so their deaths are excluded from the First Dose group.
I don't know how you find the time, but the depth and length of this post is impressive. Cheers
Hello again. I saw the post from Alex just a little while ago and read both you and publius' post regarding that study on vaxing the folks with previous natural immunity. The particular chart he highlighted looks like it shows that with NI you have both Nucleocapsid and Spike antibodies and after inoculation, you have trended to a mostly spike based capability. What I wanted to see if you could shed some light on what this means and if you've been jabbed are you more at risk to being in the camp with all the vax only folks with just spike antibodies and no or reduced sterilizing N antibodies? The chart shows a downward trend of N and upward of S assuming if we went out farther in time, it might continue to change? I'm sure the answer is we don't know yet. What's disturbing is if it turns out that we are trending to spike only antibodies, it looks like the NI folks are going to be in the same boat as the only vaxed group? Meaning we now have a bigger problem with this group now suceptible to mutated variants as well as potentially being factories creating more variants? I hope I'm wrong???