


The Natural Immunity Illusion Illusion, Pt 2
Pfizer vaccine efficacy flags in Israel. But what about the previously-infected?

Continued from Part 1.

As he was talking with them, Goliath, the Philistine champion from Gath, stepped out from his lines and shouted his usual defiance, and David heard it. Whenever the Israelites saw the man, they all fled from him in great fear.1
Delta Goes to the Battlefront
Our version of David is no future king. Delta, who comprises the super-majority of the current “cases” of infection with SARS-CoV-2 in Israel, will not be hailed by the songs of her dancing women for his gains; nor win Saul’s daughter in marriage; nor lead willing soldiers in raids on her enemies. Rather, he will be cursed by all for bringing ruin. Even now, he scatters the (Pfizer-BioNTech-contracted) defenses of the kingdom, garnering headlines for stripping the so-called vaccine of its once-proud “94+% effective” status.2 And though David’s escapades have yet to push hospitalizations for severe Covid-19 past the triple-digit mark, he has whipped the Israelites into a state of crisis. The Ministry of Health has reinstated indoor mask mandates barely two weeks after revoking them;3 the list of foreign lands for which visitation is banned or restricted, due to the “risk” that doing so will strengthen David, has expanded to encompass a quarter of creation;4 the ousted king, who himself foisted this now-failing armament on his people in his failed bid to retain power, has called for the immediate triple-dosing of all the kingdom’s elders, citing the advice of unnamed priests;5 the foreign manufacturers of the armament meanwhile have cited their own failure in Israel to justify their formal request to allow triple-dosing in their own homeland;6 and the new king, for his part, has urged the commoners to act as though full lockdown has been (re-) decreed, in order that it will not have to be.7
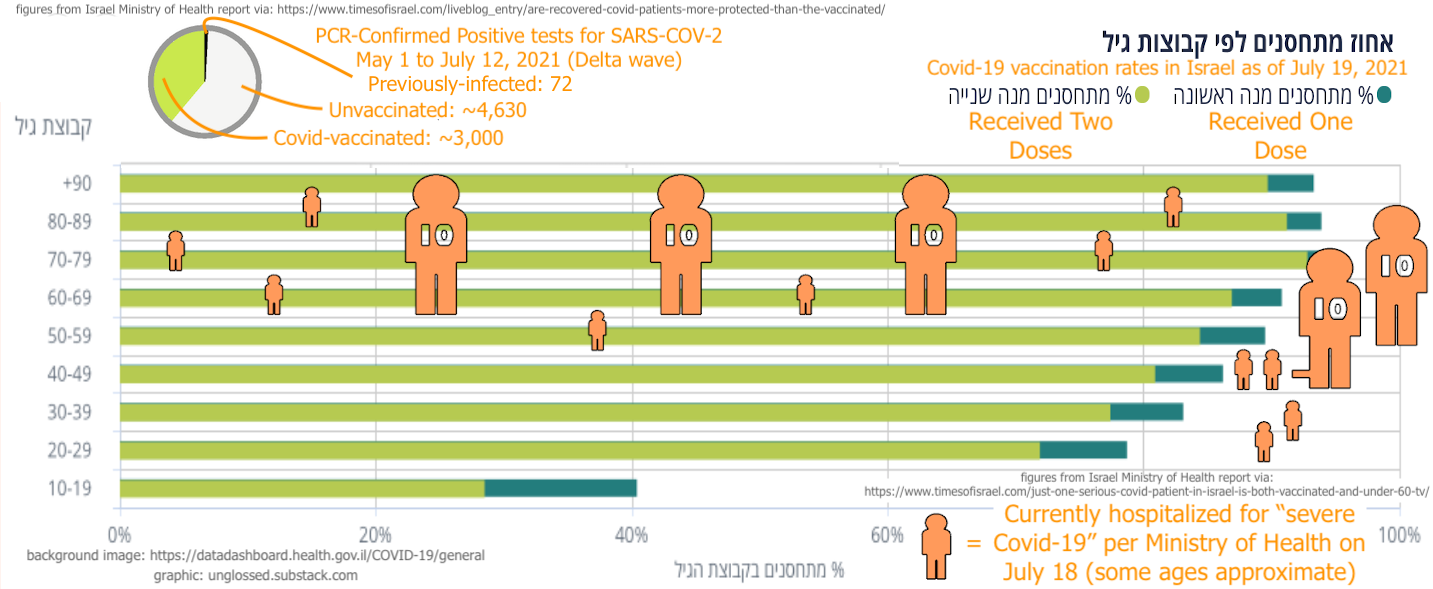
Yet the new king, despite the taunting of the old king, has not renounced the failing defense system that he inherited; and the Ministers of Health, perceiving the implications of their renewed panic on the public’s faith in their wisdom, have made efforts to reassure their flock that the defense system yet holds against David’s embarrassments. As night fell over the battlefield on Sunday, Channel 12 News cited Ministry figures concerning the 61 citizens who were currently hospitalized for severe Covid-19: Although 37 are fully vaccinated, only one of those is below 60 years old, and only by a few years. Meanwhile - a-ha! - of the 24 unvaccinated, 10 are older than 50, but 12 are younger than 50 (but older than 40), and 2 are younger than 40.8
The Ministry has a point. As well-above 90% of Israelis over 60 are Covid-vaccinated, it makes sense that if 36 Israelis over 60 are seriously ill with Covid-19, 36 Israelis seriously ill with Covid-19 would be Covid-vaccinated. The same pattern obtains among those entries in the American CDC’s VAERS reporting system where cause of death is Covid-19: Of course these deaths “from Covid-19” are occurring among the vaccinated, because they are occurring among Americans over 80 years old, who are all vaccinated.9
Meanwhile, as rates of full Covid-vaccination for Israelis between ages 30 and 49 are also quite high - between 77 and 80% - the hospitalization of 14 unvaccinated and 0 Covid-vaccinated appears to show that the Pfizer Covid vaccines are preventing (the already rare instance of) severe Covid-19 illness among recipients under 50. Moreover, the middle-aged adult unvaccinated still remain overrepresented compared to the elderly vaccinated:10
On the other hand, this assurance from the Ministry grates against their update from late June, when they assured the Times that “under 16%” of the ~24 citizens who were seriously ill with Covid-19 were fully Covid-vaccinated.11 That previous assurance sharply undermines the new assurance. If, among the severely ill, the number of unvaccinated has climbed from ~20 to 24 in the last 20 days, and the number of Covid-vaccinated has climbed from ~4 to 37, the trend developing during this burgeoning “third wave” is not promising:
Hospitalizations for Severe Covid-19 in Israel circa June 24
Unvaccinated: ~20
Covid-Vaccinated: ~4
7-Day Average Daily New Cases: 104
June 14 7-Day Average Daily New Cases: 15
Hospitalizations for Severe Covid-19 in Israel on July 18 (% change from June 24)
Unvaccinated: 24 (+20%)
Covid-Vaccinated: 37 (+825%)
7-Day Average Daily New Cases: 791 (+660%)
July 8 7-Day Average Daily New Cases: 411 (+26%)
The increase in PCR-confirmed infections seems to have had disproportionate impact among the Covid-vaccinated and, accounting for the lag between infection and hospitalization, merely a proportionate impact among the unvaccinated.
We can therefor easily imagine that a drop to Pfizer Covid vaccine serious-outcome efficacy may lie around the corner, proving to be just another “lagging indicator.” On the other hand, such a drop would have to be contextualized with the timing of vaccination of the individuals currently driving the change: If the efficacy at ~180 days after 2nd dose is lowered, the efficacy immediately after remains untouched, as it was already demonstrated during the late winter wave. It would almost have to do so, unless the age of Covid-vaccinated Israelis with severe Covid-19 lowers to include populations who were only more recently dosed.12 Thus, we will have to wait until any difference in (the already rare!) serious-outcome rates emerges for younger age groups to judge whether the serious-outcome efficacy “fades” at the same rate.
13Even more significantly, the proposition that Covid-vaccination will bring about “herd immunity” appears completely refuted. If Delta has achieved Covid-vaccine escape (or if it has merely happened to come along at the moment when Covid-vaccine protection is expiring), it would not really matter, in terms of herd immunity, whether recipients were still protected from severe illness: They are not contributing to herd immunity! Thus it doesn’t matter if Israel is at 50% Covid-vaccinated, 75% Covid-vaccinated, or 100% Covid-vaccinated. Israel cannot get to the Coronavirus czar’s 80% herd-immunity benchmark if Pfizer Covid-vaccine recipients are not functionally immune to infection.
Neither can any other country.
This, more than anything else, gives the lie to the recent efforts by various national public health boards, including Israel’s, to shift their own goalposts and redefine Covid vaccine “efficacy” from infection immunity to “severe outcome immunity,” in accordance with the legalistic definition contained in the fine print produced to support their rushed trials and authorizations, and in opposition to what the public would naturally have imagined they were being sold in the winter and spring. It is a fraud, this goalpost-shifting. The herd immunity goal was never simultaneously dropped, and has been used as a bludgeon to shame those who haven’t obeyed their elite patrons’ “suggestions” quickly enough. Therefor these so-called vaccines were intended to grant immunity from infection, not just according to the narrative logic under which they were sold to the public, but per the aggressive and autocratic threats made by government officials to the neighbors, family, and coworkers of the yet-unvaccinated that those people, explicitly would be the difference between driving SARS-CoV-2 to extinction and allowing vaccine-escape.
Thus, things do not look good for Saul’s 2.6 billion-shekel mail-order defense system. But Israel’s hopes - and humanity’s - have never truly rested on it! For even as the kingdom’s synthetically-generated antibody army falls into disarray, our version of Goliath - natural immunity - continues to issue his call of defiance to David, having already cowed David’s elder brothers into silence. And David, amidst his sowing of confusion in the ranks of Saul, has heard it.

Then he took his staff in his hand, chose five smooth stones from the stream, put them in the pouch of his shepherd’s bag and, with his sling in his hand, approached the Philistine.
Statistics currently emerging on Delta’s success in overcoming natural immunity suggest… the stone has missed its mark. Unfortunately, citing these statistics is a bit arduous, given the Israel Ministry of Health’s predilection for issuing updates through their intermediaries at Channel 12 and 13. Fog of war, and all that.
In the update reported by Channel 13 on July 12, the Ministry revealed that, according to preliminary data, there have been only 72 PCR-confirmed reinfections since May, which is considered the beginning of the summer wave. This puts their share in total infections in the same time period at ~.93%, whereas their share (that is, the amount of individual confirmed positive-tested “cases” of SARS-CoV-2 before May) in the overall population is ~9.3%.
Meanwhile, Covid-vaccinated Israelis account for 57-63% of the overall population, and 39% of summer wave PCR-confirmed infections. While the Times of Israel liveblog begrudgingly acknowledged the Channel 13 report,15 which corroborates the figures we will be using here, a more thorough review of the implications of the report is provided by the alternative Israeli-media outlet Arutz Sheva:16
With a total of 835,792 Israelis known to have recovered from the virus, the 72 instances of reinfection amount to 0.0086% of people who were already infected with [SARS-CoV-2].
By contrast, Israelis who were vaccinated were 6.72 times more likely to get infected after the shot than after natural infection, with over 3,000 of the 5,193,499, or 0.0578%, of Israelis who were vaccinated getting infected in the latest wave.
We may also echo the reinfection (is rare) studies reviewed in Part 1, and compare the reinfection rate to the not-previously-infected infection rate.
Our caveats: As with the PCR-based (and antigen-test-based) studies, the “not-previously-infected” group likely includes some number of previously-infected individuals who were not sorted into the previously infected group by PCR test, and the degree of screening-testing in both previous waves and the current waves is a factor to take into account when comparing these results with other countries or other studies (with the supposition that very high levels of screening-testing will make PCR positive-testing statistically less indicative of functional natural immunity). Additionally, these preliminary findings may be revised upward if more confirmed previous infections are found within the elapsed portion of summer wave infections. Nonetheless, using the (probably approximate) 7,700 figure and subtracting previously-infected from the overall population of Israel:
PCR-Confirmed infections with SARS-CoV-2 between May and ~July 12 in Israel
Previously-PCR-confirmed infected reinfection rate: 72 / 835,792 = .000086
Not previously-PCR-confirmed infection rate: 7,628 / 8,217,208 = .000928
Covid Vaccinated overall infection rate: 3,000 / 5,193,499 = .000578
Unvaccinated overall infection rate: 4,628 / 3,859,501 = .001199
And with that, we may revisit the studies reviewed in Part 1:
Previously-infected (PCR or antibody test confirmed) vs general/remainder population positive test rates during selected “waves” or arbitrary study periods, ratios
Pilz, S. et al. “Austria” PCR-test study: .0027 / .0285 = .09
Sheehan, M. et al “test-takers only” PCR-test study: .007 / .039 = .18
Shrestha, N. et al. “Necessity” PCR-test study: 0 / .043 = 0
Lumley, S. et al. “OUH” antibody study: .002 / .02 = .1
Rovida, F. et al. “Northern Italy” antibody study: .0178 / .0663 = .27
Rovida, F. et al. (Pavia hospital reconstruction): .0081 / .0637 = .13
Israel “Delta Wave” July 12 preliminary report: .000086 / .000928 = .09
Again, as the dust settles on this battle, the outcomes for previously infected may be revised upward. Additionally, most of Israel’s previously-infected population at the beginning of May were confirmed positive for SARS-CoV-2 in the winter wave; and most have probably been double-Covid-vaccinated. Thus, their performance during the summer wave can not be considered as robust a demonstration of the duration of natural immunity as the “Necessity” study, which set a cutoff for its previously-infected cohort in November and tracked them to mid-May. Nonetheless, as regards resilience to Delta, Goliath’s outline seems to still tower above the battlefield.
In the more pro-Covid-19-alarmism Times’s account of the Ministry’s preliminary report, the blog author makes sure to relay what those “health officials” who are skeptical of the Philistine giant’s survival have to say about this. Emphasis added:
Some experts conclude that those who had COVID are relatively safe from reinfection. But other health officials counter that the data does not take into account that new outbreaks did not spread in areas that previously saw massive outbreaks during the pandemic, such as in the ultra-Orthodox community, reports Channel 13.
Apparently it did not occur to them, that smaller rates of infection in such areas, would be yet more evidence supporting natural immunity’s efficacy.
Delta Goes to the Battledrome
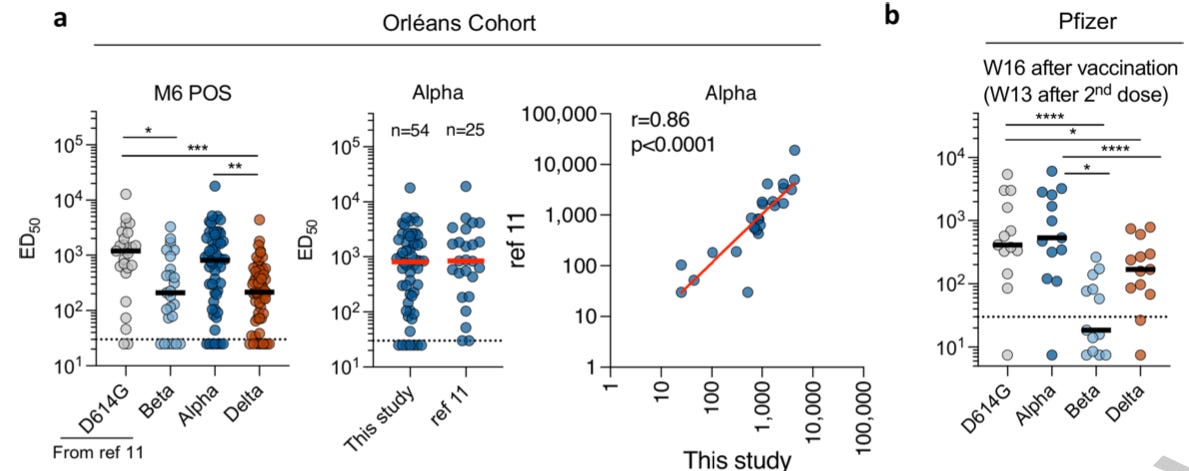
We have arrived, at last, to the alarm-raising, but not really alarmist study published online at Nature four days before the Israel Ministry of Health report, “Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization,” by Planas, D. et al.18 In this study, convalescent - that is to say, previously infected - subject sera - that is to say, blood plasma - was tested to look for differences in effective inhibition of four versions of SARS-CoV-2: “D614G” (out of Europe, all the rage in summer 2020), Alpha, Beta, and the dreaded Delta.
The study is of a baroquely elegant but grandiose design, played out on the esoteric instruments of molecular biology reporter-proteins and high statistics. We will not be doing the design or the practical mechanics any justice in our review here. To do so, frankly, would be a chore. (In fact, readers not eager to read about the study’s novel methods may safely skip to the conclusion.)
The authors mixed convalescent sera with cultured live samples of their four versions of SARS-CoV-2. After fifteen minutes, these mixtures were poured out onto sweet, innocent reporter-gene modified target cells, who had nothing but the convalescent donor’s antibodies to protect them from doom. Meanwhile other sweet, innocent reporter-gene modified target cells were left under the protection of synthetic “monoclonal” antibodies, or the antibodies of donors who were at various stages of Covid-vaccination. This design built upon as well as repackaged the design and results of an earlier trial by the same authors.19
In the first study, donor samples were diluted 1/30, and this was the baseline for arbitrarily designating which donors were “neutralizers” or not: Those donors whose samples stopped the target cells from expressing spike protein, fusing to their neighbors, and forming the blue-light sensitive GFP protein that signifies fusion, at 1/30 dilution were the “neutralizers.” Their samples were then diluted further, to find the neutralization breaking-point. To correct for the noise of molecular happenstance, all of these tests were repeated multiple times, and statistical machinery was employed to decode the resulting chaos. Samples that had a higher dilution breaking-point were regarded to be more effective at blocking the viral spike proteins.
In a way, it’s a brilliant (and apparently novel, or at least hyper-specialized) methodological construction, which piggybacks the cell-fusion effect of SARS-CoV-2 and turns it into a sort of viral measuring-wheel. In another way, it’s quite a flawed approach, and possibly not ready for prime time.
In the follow up study which includes Delta, at least, the authors reduced their initial “neutralizer” dilution benchmark, having apparently determined that 1 / 30 was not sufficiently sensitive to differences between samples and produced too many false “non-neutralizers.” In fact, once they were testing the “post Pfizer-vaccination” groups, they seem to have set the starting point at 0 dilution. This makes sense. The elegance of the “S-Fuse challenge” design is that, unlike ELISA, there is theoretically no limit to the possible dynamic range of “difference-seeing.” If the exposure of ELISA needs to be carefully calibrated for every given purpose, the French authors’ S-Fuse assay method meets reality no matter where it is hiding. Except, in reality, S-Fuse has a significantly low ceiling on theoretical sensitivity. Achieving the measurable result depends on a large enough number of target cells 1) taking up SARS-CoV-2; 2) manufacturing and expressing spike protein; 3) successfully binding the spike protein with their “opposite GFP sex” neighbor’s ACE-2 receptor to unite into a supercell blob; 4) forming the post-union complete GFP protein within the blob so that when a particular wavelength of blue light is shot at the cells, the reader detects the emission of particular wavelengths of green light. Although long incubation times (18 hours, in this case) give the virus ample time to make up for a slow start, there is a limit to how low the S-Fuse test viral exposure can be calibrated without risking that GFP readings will be low even if the virus is not being inhibited by anything. Therefor, this approach has a built-in bias toward at least some degree of overkill. What the S-Fuse challenge calls a 0, might not be a 0. Even at an undiluted concentration, failing to “neutralize” the virus in this framework does not tell us anything absolute about the immune potential of the donor, whose blood plasma in real life would be circulating throughout the body, not trapped in a cage match with no backup.20
Thus, what the study characterizes as “non-neutralizer” is only in the context of the unknown limitations of sensitivity of their S-Fuse test. This itself is not a knock on the S-Fuse design,21 per se. Traditional, ELISA-based antibody tests, after all, have their own limitations as regards their employment for “qualitative” antibody testing - which is to say, for determining if a sample “has antibody” - whereas their value for “semi-quantitative” testing - here’s a bunch of samples, do some bind more than others? - is more robust.
Furthermore, the authors’ ostensible primary interest is in the evolution of the spike protein, and mining as much observational data as possible about how this evolution impacts successful antibody-evasion and cellular infiltration, and what insights into the magical world of proteins may be gleaned from this; not in functional immunity. The study primarily wants to look for differences between strains of SARS-CoV-2, not between human immune responses. In fact, there’s not even any apparently useful way to yet distinguish between differences in “antibody-evasion fitness” and “cellular fusion fitness” when evaluating S-Fuse results, as the spike protein is always evolving in both those directions at once.22 We therefor might question their choice of title. It could, perhaps, do with a question-mark at the end.
And that, at last, brings us to the core of what the French study effectively demonstrates, albeit with actual cellular infection being measured instead of blunt antibody-binding.
At the viral exposures used by the authors, only recently 2nd-dosed vaccine recipients and natural immunity donors at 6 months post-infection could inhibit Delta even at very low donor sample concentrations, but only the latter group also did well with Beta.24 Another group, which was both 12 months post-infection and vaccinated, scored best across the board. Meanwhile, even at high donor sample concentrations, (Beta and) Delta (at the viral exposure used by the authors) was effective at evading inhibition from both 1st-dose vaccine recipients and natural immunity donors at 12 months post-infection. From the study. “Ref 11” merely refers to the recycled results from the authors’ earlier-published trials. The dotted line merely serves to compare the initial baseline dilution to the 0 dilution baseline in the Pfizer results:

Comparison between the post-infection samples and post-Covid-vaccination samples is not all that useful, in the premature construction offered to us here. Whether 6 and 12-month convalescent serum is less effective at inhibiting SARS-CoV-2 than ~2 and ~3 month post-2nd dose in a blood sample is barely interesting. We would want to see either earlier post-infection performance, or later post-Covid-vaccination performance. Only time-matched side by side comparisons of natural immunity and Covid-vaccine immunity might reveal interesting differences between the two responses. A lowered inhibition after 12 months (from infection or Covid-vaccination) is not significant in of itself in any way; it merely reflects natural immunity working as per design.
The corollary to “antibody decay” in humoral immunity is “antibody ramp-up;” this is the “memory,” or adaptive portion of immunity. Further, humoral immunity - antibodies - does not work in a vacuum; it is itself complemented by cellular immunity, which also has the advantage of adaptation when facing previously-encountered opponents. To reprise the central refrain of Part 1; lowered antibody response does not imply lowered functional immunity. Only observation of real-life reinfection rates would give us the data with which to correlate antibody levels to reinfection risk. Until then, the burden of proof is on the virus; and normal expectations of natural immunity’s duration must prevail in our risk assessment. But beyond that, to even imagine that time-diminished antibody efficacy in the S-Fuse “Infection Simulation Battledrome” implies the would-be defeat of the absent warriors, adaptive humoral ramp-up and cellular immunity, is stretching the study results too far. I mean - come on!
These are our bodies! Our immune systems! They have served us and protected us from the billion microbiological hazards encountered daily for eons! They aren’t invincible, but their works are more intricate and incredible than human minds and instruments can measure! We must balk at the suggestion that we trade them in, crumple them up and toss them into the recycle bin - merely upon the report that a virus ate up a few cells somewhere over in France.
25Here we may observe echoes of our analysis of the study from Singapore. In both that study and this one, it was necessary to parse the “significance” of the measured results both in terms of how significantly different the measurements were, and what the differences signified in the real world. The authors asserted that the measured differences were not significant in either aspect; we concluded that the measurements were significantly different, but that the real-world significance was unknowable. Here, we agree with the authors that the results are significantly different, but we disagree with any external interpretation that these differences suggest any meaningful real-world significance.
The context in our Singapore evaluation was that the implications of higher antibody-binding to pregnancy are, to reclaim the legalistic slanders levied against natural immunity, “unclear,” and “not well-described.” In the S-Fuse challenges, the implications of lower antibody-inhibition between 6 and 12 months post-infection are extremely clear, and extremely well-described, and with most viruses the implications are that these changes are insignificant. Proof that SARS-CoV-2 does not behave like most viruses must come from real world reinfections; otherwise the operative expectation is that it will behave like most viruses. Is that a double-standard? Yes. Risk assessment is nothing if not a tapestry of double-standards.
All that the S-Fuse study demonstrates is how various evolutions of the SARS-CoV-2 spike protein affect antibody-evasion and cellular fusion, not functional immune escape, natural or vaccine-induced.
Broad immune escape may come, one day. Continuing to search for early warnings of its arrival will only add length to the trail of false alarms which proceeds it.
There is a world of people with year-old antibodies to SARS-CoV-2 out there, and they aren’t getting sick.
Goliath is not afraid of death. He courts it; he calls out to the brothers of David to test his strength. Goliath knows he will not live forever. So too with natural immunity. It does not always last forever.27
Antibody concentrations lower over time, after recovery from infection. Although antibodies can be quickly ramped up upon reencounter with their corresponding antigen, there is a window left open to any given virus to catch the immune system off guard with a high viral-load event, or via antigenic shift. Gradually, natural immunity from a given bug transitions from the near-digital realm of infection immunity, to that more analogue spectrum of “outcome immunity” in which Israel’s Pfizer Covid vaccine recipients already find themselves. Then, like in the OUH study, a brief asymptomatic or mildly symptomatic illness is followed by an increase in (natural-infection derived) antibodies, and the cycle starts again.
This is how the immune system is meant to work - calibrating itself to the reality on the ground, to the “menu of hazard” on offer by one’s fellow organisms. If herd immunity to SARS-CoV-2 is ruled out by Goliath’s thirst for challengers, so be it. Who died and made herd immunity king, anyway!?
Natural immunity is up for the battle that it calls out for, though it may not always win. And it is and always will be the only warrior that humans have. It is innate. It is self-regulating. It is designed to make existence possible on a planet where every other organism is a galaxy of cells in a galaxy of other galaxies, each individual cell a playground for self-evolving genetic junk-mail - and to do this without dependance on the interventions of science.
Natural immunity doesn’t need herd immunity; if it did, it wouldn’t exist to begin with, and neither would we.28
Continued in epilogue: The Hyperlink Archipelago…
1 Samuel 17:23
Update to Vaccine Effectiveness, July 5, 2021. Overall transmission as well as symptomatic infection rates, as measured by the Ministry of Health, have been dropped from 94% to 64%. The “serious outcome” rate has been dropped from 98% to 93%.
Times of Israel staff. “Israel to reinstate indoor mask mandate next week as COVID-19 cases keep rising.” (2021 June 24.) The Times of Israel.
Update to List of Destinations with the Highest COVID-19 Risk, July 16, 2021; I have not yet calculated the actual percentage of the globe encompassed.
Tercatin, R. COVID: Netanyahu calls for 3rd vaccine for over 50s, experts skeptical. (2021 July 7.) The Jerusalem Post.
Neergaard, L. “Looking at delta variant, Pfizer to seek FDA authorization for 3rd vaccine dose.” (2021 July 9.) The Times of Israel.
Pfeffer, A. “Israel on brink of lockdown after dropping facemask rules.” (2021 July 17.) The Times UK. Using the construction offered by this headline, we may fable-ize a man who repeatedly waits until the tide has been withdrawn for several hours before daring to place his chair by the shore, and then curses his breach of chair-vigilance for once again “causing” the return of the tide.
Spiro, A. “Just one serious COVID patient in Israel is both vaccinated and under 60 — TV.” (2021 July 18.) The Times of Israel.
Their mortal outcome may therefor be considered likely to be coincidental to their Covid-vaccination, and not yet an indicator of the dreaded ADE. Instead, they are merely being added to VAERS due to accidents of timing.
Background image from https://datadashboard.health.gov.il/COVID-19/general
Times of Israel Staff. “Israel to reinstate…”
In hospitals across the country, 26 patients were in critical condition, among them an unvaccinated child, the Health Ministry said. Over 84% of seriously ill patients were not vaccinated.
However, the dashboard value does not go over 24 for any of the days near June 24. I therefor decided to use 4 (Covid-vaccinated highest plausible June 24 baseline) and 20 (unvaccinated near-lowest plausible June 24 baseline) as the approximate values for severe cases, to be generous to Pfizer.

However, an observation of the “fading” of 2nd-dose severe-outcome efficacy would not tell us anything about the efficacy of triple-dosing, which may prove to have diminished, null, or even exacerbating impacts to severe outcomes for individuals infected with SARS-CoV-2 or even other coronaviruses or viruses generally.
(index link anchor)
“Are recovered COVID patients more protected than the vaccinated?” (2021, July 12.) Times of Israel.
Rosenberg, D. “Natural infection vs vaccination: Which gives more protection?” (2021, July 13.) Arutz Sheva.
(index link anchor)
Planas, D. et al. “Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization.” Nature.
Planas, D. et al. “Sensitivity of infectious SARS-CoV-2 B.1.1.7 and B.1.351 variants to neutralizing antibodies.” Nature Medicine. And here the authors are building on SARS-CoV-2 research approaches published in November by Buchrieser, J. et al. in “Syncytia formation by SARS‐CoV‐2‐infected cells,” The EMBO Journal. And there, Burchrieser, J. et al are repurposing research Burchrieser conducted with a smaller team on protein-dependent placental formation-retardation from July, 2019 in “IFITM proteins inhibit placental syncytiotrophoblast formation and promote fetal demise,” Science. Why not just have titled it, “INSERT GLOBAL STERILIZATION CONSPIRACY THEORY HERE”?
Further development is sure to verify and improve the potential sensitivity of this approach, but as it stands, the study’s failure to include comparative results between their “S-Fuse non-neutralizer” samples and “traditional” SARS-CoV-2 antibody tests (which are calibrated according to observed antibody concentrations in recently infected individuals) gives the reader nothing on which to base a rough conjecture of the effective lower-limit of sensitivity for antibody inhibition potential of these tests.
(the (suspiciously form-fit-for-SARS-CoV-2) S-Fuse design)
I would add one more perceivable potential flaw, which is that by not performing their sera S-Fuse challenges in “real-time” - as in, when the samples are taken - the authors may be introducing novel distinctions in antibody efficacy due to sample storage, which might not be relevant in a regular antibody binding assay but could be relevant when dealing with live viral-cellular infection.
(jump anchor)
One may go further, and observe that the inhibition 6-months post-infection was found to score “higher” (still occur at greater dilutions) than the inhibition 3-months post-vaccine - so much so, that the author’s had to use a chart with a higher ceiling! However, this conclusion must be tempered by the fact that the 6-months donor sample was disproportionately inclusive of more severe original infections than one would observe in a general population:

(index link anchor)
(index link anchor)
Quite possibly, for very good reasons. One may theorize without much effort that antibody fade-out functions as the braking system for auto-immune antibody production; saves on metabolic costs; constitutes a bid by individual immune systems against creating “herd” evolutionary pressure on viruses to defeat currently-functioning antibodies.
Which is not to be confused with the opposite construction. “Herd immunity” needs natural (even if traditional-vaccine-calibrated) immunity.
Hi Brian, I enjoyed reading not only your Natural Immunity 1 & 2, but also like the Rock Bottom as well. I wanted to reach out to you regarding a study that the CDC just published stating the people with NI who also get vaccinated are 2.34x less susceptible to reinfection vs. just those who have gotten NI from a previous infection. I simply can't believe their claims to be true other than yet another attempt to help justify jabbing everyone. Here's some of their claim:
"Among Kentucky residents infected with SARS-CoV-2 in 2020, vaccination status of those reinfected during May–June 2021 was compared with that of residents who were not reinfected. In this case-control study, being unvaccinated was associated with 2.34 times the odds of reinfection compared with being fully vaccinated.
What are the implications for public health practice?
To reduce their likelihood for future infection, all eligible persons should be offered COVID-19 vaccine, even those with previous SARS-CoV-2 infection."
https://www.cdc.gov/mmwr/volumes/70/wr/mm7032e1.htm?s_cid=mm7032e1_w
Curious to see if you spot anything obviously false or misleading since it's complete counter to the data you analyzed in NI Ilusion Ilusion?