


IgG4 passed to newborns in Covid-vaccinated mothers
Preprint confirms an unsurprising potential problem for humanity.

Summary (click to expand):
The preprint, just uploaded:1

The “protein,” as they say on Succession:
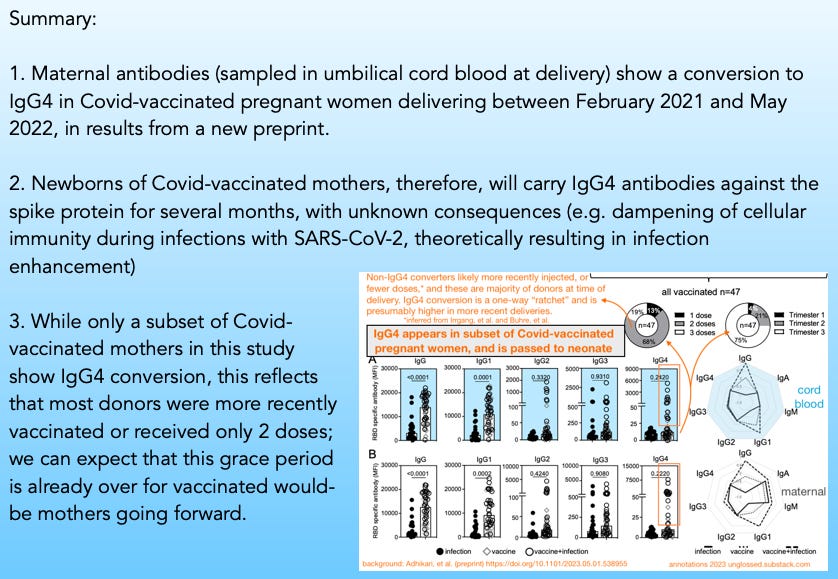
Among 47 Covid-vaccinated mothers delivering and sampled between February, 2021 and May, 2022, a subset score for IgG4 antibodies for the SARS-CoV-2 spike protein, unlike any of the naturally infected mothers. These antibodies are also present in cord blood, indicating they were transferred to the newborns, and will persist for some months after birth.

Background on IgG4
IgG4 conversion after mRNA vaccination was first reported and discussed here, almost a year ago. See the original post for background on what IgG4 is, and why IgG4 “tolerance” may suppress cellular immunity during infection:
A more full-fledged discussion of IgG4 and a potential role in severe disease, going forward, is here:


Background on the study
Women who, during pregnancy, were either infected with SARS-CoV-2 (22), Covid-vaccinated (19), or both of the above (28), and went on to deliver between February 2021 and May 2022 had maternal and umbilical cord blood sampled at delivery.
The resulting study predominantly focuses on modifications made to a sugar attached to antibodies that influence their functions, and whether antibodies for the SARS-CoV-2 spike protein have different levels of these modifications compared to overall antibodies, and in cord blood (the source of maternal antibodies in infants) vs. maternal blood. However, our interest is just in the IgG4 results.2

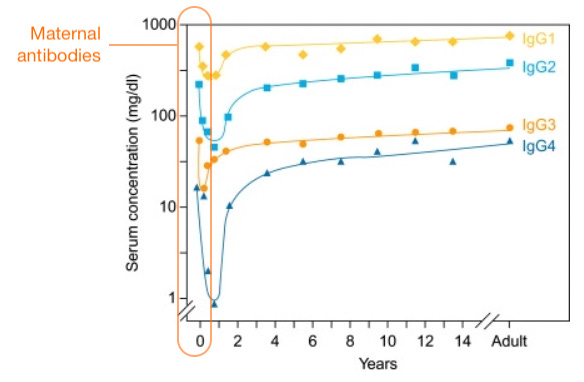
Maternal antibodies, fortunately, rapidly fade
The theoretical danger of IgG4 antibodies for newborns infected with SARS-CoV-2 is obvious — it is at least a known unknown risk. Circulating IgG4 might suppress clearance of infected cells that are displaying spike protein, and this might lead to enhanced infection and severe disease, or viral persistence; so far there is no direct evidence to inform one way or the other.
If there is a direct risk, however, it will presumably only apply for as long as maternal antibodies persist in infants, which is only a few months.
As long as IgG1 for spike protein outnumbers IgG4 at birth, it still will do so as antibodies fade out.
However, even a minority of IgG4 can still sabotage IgG1 function where it “really matters,” which is on particular spike proteins attached to particular infected cells — IgG4 has been understood for decades to be able to defuse IgG1 complexes that activate “auto-destruct” functions on infected cells via complement proteins.3 This is consistent with IgG4's role in tolerance to begin with — it exists to defuse immune response after persistent antigen exposure.
While it is normal to get “a little” IgG4 among all maternal antibodies in general, this is not the same as getting “a little” IgG4 for a coronavirus that wants to use all your baby’s cells as its own birthing ward.
Again and in summary, the theoretical risk of infection enhancement for newborns is obvious; but at least it should only last for the window in which maternal antibodies stick around.
Only a glimpse of the future
That only a “subset” of vaccinated mothers convert to IgG4 in Adhikari, et al. is no cause for relief — it simply reflects that most would have only been recently-injected, and are in delivery before IgG4 conversion has had time to take place. We can infer from Irrgang, et al.,4 Buhre, et al.,5 and a newly-uploaded fourth IgG4 study6 (hat-tip to reader OhioPatriot) that the outliers who convert to IgG4 are the same mothers injected earlier in pregnancy and/or who receive a third dose.
Reminder: IgG4 conversion is a one-way “ratchet”
B Cells change what class of antibody they pump out by deleting their own genes. Once a B Cell has reached IgG4, there are no more deletions left to make corresponding to other IgG classes, and this B Cell and its clones will only make IgG4. Today’s IgG4 B Cells are yesterday’s IgG1 B Cells; but will only be tomorrow’s IgG4 B Cells. They cannot go back. Additional exposure to spike can only increase tolerance.
Newborns, fortunately, aren’t getting the B Cells; only the temporary antibodies that they were producing inside the mother. But mRNA-vaccinated mothers who were capable of making only normal, IgG1-dominant antibodies in 2021 and early 2022 stop being able to do so going forward. Women who are mRNA-vaccinated (per the results of three different studies looking at general immune responses) only have a short grace period before IgG4 conversion resulting (per Adhikari, et al., this new study) in transfer of IgG4 anti-spike antibodies to any offspring they have later in life.
Thus, the “outliers” with IgG4 conversion in Adhikari, et al. were a glimpse of the future for Covid-vaccinated would-be mothers; and now likely represent the norm.

Per additional studies on responses following infection after vaccination, these IgG4 antibodies will likely cross-react to any variants encountered after the original vaccination.7 In other words, they will not be strictly “Wuhan”-directed, but will bind to spike from currently-circulating versions of the virus.
Needless to say, this is uncharted territory. By-and-large, humans have never front-loaded newborns with (temporary) IgG4 for a common respiratory virus, and no one can say what the result will be. All that is certain is that nature doesn’t do this.
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Adhikari, EH. et al. “Diverging maternal and infant cord antibody functions from SARS-CoV-2 infection and vaccination in pregnancy.” biorxiv.org
Generally, the vaccine-induced antibodies are found to be “loaded up” with presumably useful functions vs. natural infection, and score more highly for neutralization. However, as with real-life results among vaccinees, this is no proof of superior immune protection vs. the natural infection immune response — even regarding severe disease alone, it may all be “overkill.” And since it is presumably the outcome of heavy and prolonged spike expression resulting from mRNA transfection, it is double “overkill” in the sense of pushing recipients toward IgG4 conversion and tolerance.
As an interesting exception to the lower scores for presumably useful functions in the naturally infected, results in cord blood for antibody-mediated phagocytosis are comparable than those in the vaccinated group. As this result is largely driven by poor performers in the vaccinated group, it may be a result of the IgG4-heavy vaccinated samples blunting cellular immunity in vitro, similar to the confirmatory results in Irrgang, et al. (however, this would require raw data to confirm).

Van der Zee, JS. Van Swieten, P. Aalberse, RC. “Inhibition of complement activation by IgG4 antibodies.” Clin Exp Immunol. 1986 May; 64(2): 415–422.
Irrgang, P. et al. “Class switch towards non-inflammatory IgG isotypes after repeated SARS-CoV-2 mRNA vaccination.” Sci Immunol. 2023 Jan 27;8(79):eade2798.
Buhre, JS. et al. “mRNA vaccines against SARS-CoV-2 induce comparably low long-term IgG Fc galactosylation and sialylation levels but increasing long-term IgG4 responses compared to an adenovirus-based vaccine.” Front Immunol. 2023 Jan 12;13:1020844.
Rastawicki, W. Gierczyński, R. Zasada, AA. “Comparison of Kinetics of Antibody Avidity and IgG Subclasses’ Response in Patients with COVID-19 and Healthy Individuals Vaccinated with the BNT162B2 (Comirnaty, Pfizer/BioNTech) mRNA Vaccine.” Viruses 2023, 15(4), 970
Thank you for staying on top of the IgG4 learnings Brian. Two words: Unintended consequences.
Here's more new coverage, albeit general;
https://www.nature.com/articles/s41577-023-00871-z
Review Article
Published: 24 April 2023
The unique properties of IgG4 and its roles in health and disease
IgG4 against bovine folate receptor alpha (FRA) crosses the placenta to cause autism in the fetus.
https://www.bmj.com/content/361/bmj.k1674/rr-2
https://vinuarumugham.substack.com/p/cows-milk-protein-contaminated-vaccines