


Reading Rec's, Resource Upload
Birth-year flu antibodies in 1952/3, re-visualized (with spreadsheet).


First, some recommended reading:
Interpreting spike protein in nucleus evidence
Every spike study discussed here used a variation of a method called “immunofluorescence,” which is also sometimes called “immunolabeling.”
This method usually includes a “fixation” step, which kills the cells and supposedly “freezes” all the cellular components in place, and a “permeabilization” step, which allows antibodies to get into the cells and organelles (the antibodies allow us to visualize our proteins of interest).
Unfortunately, there’s a whole body of literature that warns about artifacts arising from immunofluorescence/immunolabeling.
Just last week, I mentioned (in a footnote) shelving my own review of “The V(D)J Paper” — a fortunate decision, since it could not have but looked pitiful compared to the work done by Joomi here.
Still, I would not have been as generous to the paper as Joomi finally ends up being (see my remarks in the comments).
Oh, Sweet Schadenfreude
The patient [experiencing rapid progression of T Cell lymphoma after Pfizer/BioNTech Covid “booster”] isn’t just a throw on author. He is the corresponding author and doesn’t regret his decision nor wants to discourage any vax hesitancy?
What could cause someone to be this committed to a Darwin Award? I initially looked for Pfizer funding, Gates money, Fauci favors… but alas.. It was something far simpler.
Michel has been publishing papers that study anti-vaxers like they are denigrated lab rats.
(Emphasis added.)
Ed Yong Does a Good Job (lol)
I found “One of Long COVID’s Worst Symptoms Is Also Its Most Misunderstood” an excellent, if uncomfortable read. Yong, infamous Covid-catastrophist-extraordinaire of the infamous Pandemic-panic-porn-pedling Atlantic magazine, does commit my pet peeve of hyperlinking the same source ad infinitum (the Biobank Brain Change Study); but otherwise the collection of citations regarding neurological effects of infection is good.
More valuable, though, is the description of brain fog he synthesizes from his interview subjects, which I found quite apt (having dipped my toe in Brain Fog Lake for two days in January1):
And despite its nebulous name, brain fog is not an umbrella term for every possible mental problem. At its core, Hellmuth said, it is almost always a disorder of “executive function”—the set of mental abilities that includes focusing attention, holding information in mind, and blocking out distractions.
This captures what it suddenly felt like, as I was working on a review of ONS data2 — my consciousness was still there, but the “person” running it had just suddenly checked out.
Reading Yong’s essay, I found — as I have in other instances — that reading or thinking about brain fog makes me feel as if I am suddenly slipping back into it. At several points, my vision blurred, my thoughts froze in place, etc.
But this was a productive torture, as the previously dim realization finally dawned upon me that brain fog resembles a very specific feeling, one that has been an intermittent visitor throughout my whole life as it surely is for most souls:
Frustration.
“Brain fog” feels and operates exactly like frustration. And yet, the “f” word rarely seems attached to it; or treated only as an incidental side-effect.
That got me to thinking: What if, rather than all the biophysical mechanisms offered by Yong’s coterie of experts, the principle cause of post-SARS-CoV-2 brain fog is chemically induced frustration? And yet to my surprise, there doesn’t appear to be much, or anything, in the annals of biology or neurochemistry about what, on a chemical level, “frustration” is (instead, the term has been unfortunately assigned to physical conflicts in biochemical systems on a micro level).
What if there is simply a neurotransmitter for being frustrated?
What if this neurotransmitter, or its receptors, are being disrupted in those who experience brain fog?
I will look into this subject, as time permits.
Resource Upload: Birth Year Pooled Antibodies
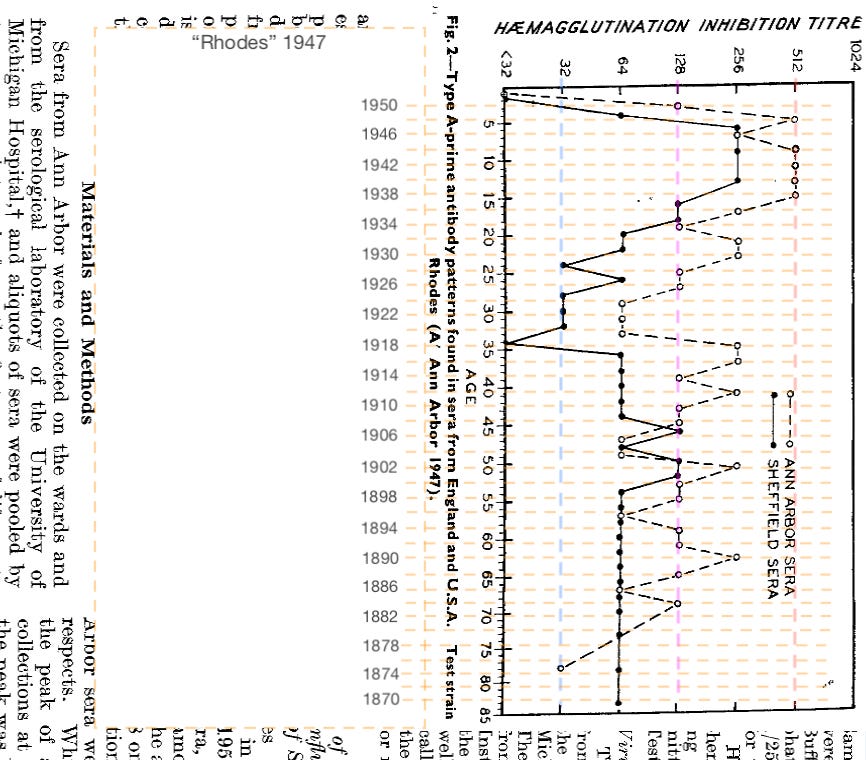
I recently discovered a little-referenced, follow-up study to the seminal paper used as the foundation of the myth of “Original Antigenic Sin” (previously discussed in “What Francis Saw”).
In this obscure, but illuminating follow-up, the Ann Arbor school once again took pooled sera samples from a hospital in Michigan, but also compared them with sera collected in Sheffield, England — and more importantly, used a different reference strain for “A prime” immunity.
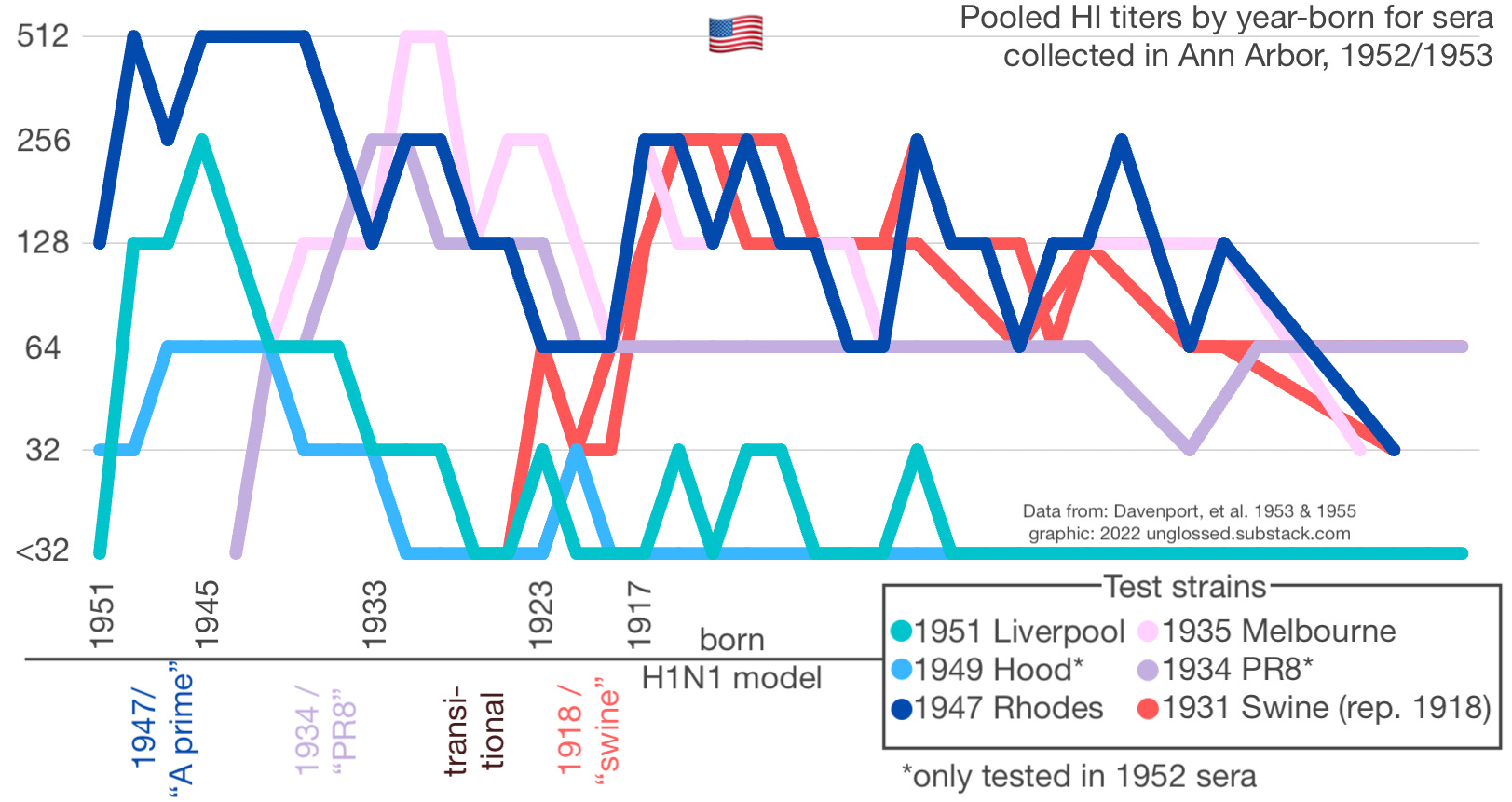
Whereas the 1953 paper (using 1952 sera) tests a 1949 strain; the follow-up paper tests a 1947 strain. The results are dramatically different: Adults of almost every age show robust antibody response to the 1947 strain in Ann Arbor; and less so in Sheffield, but still more than was apparent when using a non-representative 1949 model as before (see “focus: A Prime” below; dark blue is the 1947 strain, sky blue the 1949 strain).
I thought this discovery was a good opportunity to synthesize the results across all the relevant H1N1 strains (1918 - 1951), so I spent this morning rebuilding the raw values from pixel placement for both the 1953 (Davenport, et al.) and 1955 (Davenport, et al.) paper. The result is here:
https://docs.google.com/spreadsheets/d/1ibDDKkwZLdMuG5fa3AujU4kmSXDPyDG7f9EWR0ThVNM/edit?usp=sharing
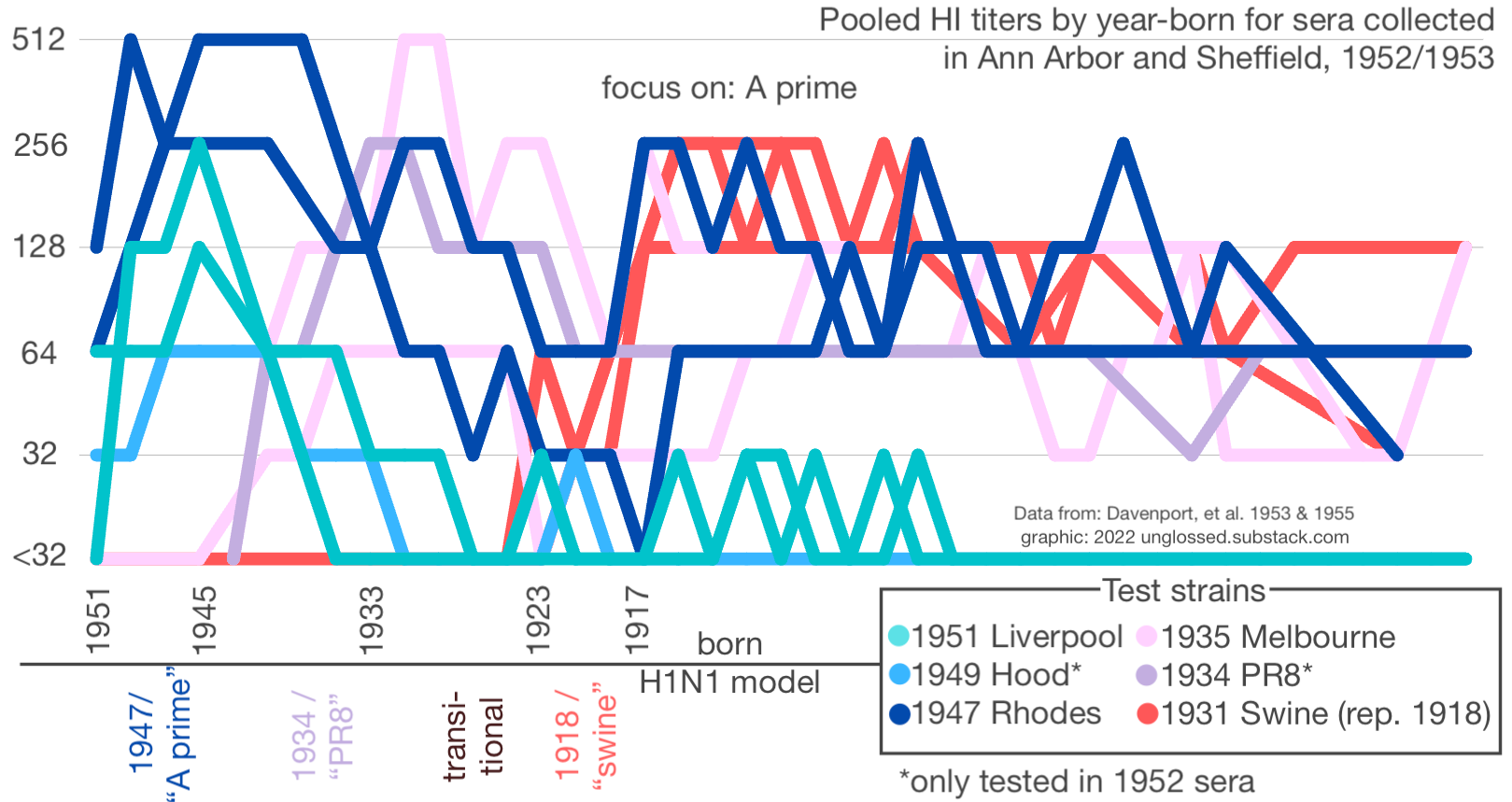
I then spent the rest of the day trying to “skill up” in data visualization, a long-needed endeavor. The results below are obviously remedial, but I like them — using big, fat line-widths, here are three different presentations of the all-age, all-strain. pooled titer results by Davenport, et al. (note that I subtracted -1 from the birth year compared to the spreadsheet, in light of likely mid-year collection effects on age):
A prime focus.
PR8 focus.

Swine / 1918 focus.

(As always, please refer to “OAS Lit Review / Timeline Pt. 1” for a full user guide of the different strains of the A to A Prime era.)
What should stand out, I hope, is how weak the evidence for “the strain encountered in childhood dominating the response!” actually was for any adult age set. For individuals who encountered the 1918 flu as children, pooled HI titers against the novel A prime model, represented by “Rhodes,” were frequently just as high (256). In fact, both PR8/Melbourne (1934/5) and Rhodes (1947) HI titers are robust in these older adults.
Also of note is the more depressed of the two “Melbourne” paths; this corresponds to the young adult Sheffield donors. (Location-exclusive graphs in the footnotes.3) The 1933-43 births in Sheffield demonstrate anti-Melbourne HI results below their corresponding performance against the 1947 strain, despite being children in the late 30’s. This may be partially explained by antigenic drift after 1935 — but even so, demonstrates that defining the “original” strain for any individual is largely beyond human powers, and so any theories built upon supposed original strains will be built on corrupted data.
Overall, nothing in the all-strain view seems too astonishing in light of the fact that whenever individuals are born, actual flu infections are more common as children. So there is nothing in these pooled results to support a detriment to later immune responses to infection as opposed to less frequent infections.
Source material: Image annotations for reconstructed raw values:






For a hundred in twenties (and a small service fee) you could spend three dollars and sixty-three cents, on Diet Coca-Cola, and unglossed biology reviews.


See “Author has the thing: Ep 2.” Obviously, having just had cause to reference my first Omicron infection diary post yesterday, Yong’s brain fog exposé found me in a particularly receptive frame of mind.
I was writing “Into the Weeds: UK Deaths Data,” one of the most math-y posts I have done.
Per-location plots:

Thank you Brian. How does your ongoing debunking of OAS in the context of flu impact your view of contemporary flu shot campaigns? My employer is once again hosting "flu shot day" soon. Is this a good thing or not?