


The Polio Problem
A review of the disease and all the puzzles left therein.

Polio series table of contents:

Despite efforts to understand [polio virus] infection within the host, fundamental questions remain unanswered. These include the mechanisms determining the progression to viremia, the pathogenesis of neuronal infection and paralysis in only a minority of patients.1
—Andersen, et al. 2019.

As the second part of my critique of the polio toxin theory in Turtles All the Way Down will deal with the criticism of the “default” theory of polio, it is convenient to offer the reader a slightly more thorough stand-alone overview of the problem.
As simple as the following overview will hopefully seem, it required an expansive trawl of the research in the decade immediately after the Salk vaccine, to avoid accidentally mischaracterizing the understanding of the virus in the mid-Century by repeating to the reader the modern, somewhat inaccurate memory of the same.
Post contents:
i. Summary of the mystery.
ii. The role of the vaccines in freezing scientific progress before the mystery was solved.
iii. The “real-ness” of the mystery: A review of things that don’t explain away the problem.
It wasn’t “misdiagnosis” — polio virus confirmed in “polio” cases in 1951/2.
For Pt. 2:
It wasn’t genetic susceptibility.
It wasn’t hygiene.
It wasn’t transportation.
It wasn’t imagination / over-reporting.
Was it a change in the virus?
i. Summary
What is the “default” theory of polio? What mysteries does it pose, which still seem to have no convincing solution to this day?
The following answers the questions in overview:
There are three viruses termed “polio virus.” They are naturally (before vaccines) as common as any other childhood virus, and natural exposure leads to the generation of immunity (antibodies and resilience to viral replication and shedding) by adulthood in most individuals — often without even producing symptoms of illness.
In rare cases, infection in yet un-immune children or adults leads (mysteriously) to paralysis. Of the clinical features, the paralysis of individual limbs with rapid wasting of muscle tissue is most distinctive, though a lesser or sometimes equal portion of cases involve cerebral paralysis (coma and quadriparesis) and bulbar paralysis (respiratory failure and death). Descriptively, the cause is destruction of some portion of the motor neuron conduits in the spine or brainstem.
Post-infection paralysis thus indicates that something went “wrong” during polio infection. But what? And even more curiously, why would the rate of this mysterious “going wrong” change in different places at different times? So begins the mystery, in the late 1800s.
In the late 1800s, and especially after 1894, the precise meaning of “rare” changed in Continental Europe, the United States, Australia, and other industrialized nations. Paralysis was still rare individually, but not so rare as before.
In accordance with this unexplained increase in susceptibility, (previously unnoticed) seasonal infections with (previously harmless) polio viruses caused local outbreaks of multiple cases of polio paralysis, mostly in young children.
Everywhere this occurred, most older children and adults had all already developed immunity to the polio viruses — they were rarely affected. The virus had already been present without causing epidemics of paralysis.
Meanwhile other parts of the globe carried on harboring polio viruses without any recorded instances of paralysis epidemics. In 1949, Hammon writes:
So far the population of no region in the world has been found free from poliomyelitis antibody, although in some of these areas clinical poliomyelitis has [never] been observed […]2
But like any childhood virus, even though most individuals would acquire immunity by adulthood, not all did, and immunity lagged in particular in rural areas (whereas in crowded urban settings, polio viruses spread more frequently, and so children were infected at a younger age). Now that the “switch” had occurred, such un-immune adults might experience paralysis upon their belated infection with one of the polioviruses, as in the famous case of FDR, but also several cases which were observed from the earliest epidemics.3
And so finally, whatever “switched” the meaning of “rare” for post-infection paralysis in the West seemingly affected all ages at once, since adults often experienced paralysis during early rural polio epidemics as well, if they were not yet immune. Future emperor of America FDR experienced polio at age 39; this was not usual in the past. But (older children and) adults had presumably always been experiencing such belated encounters with polio viruses in cold, rural areas, throughout human history, without such usual observations of adult paralysis — sanitation is not a satisfactory explanation for the “switch,” since it seems to determine polio prevalence less than population density and climate.
With similar emphasis on the early occurrence of adult cases, John R Paul summarizes the whole transition just described, in 1958:4
It is now fairly well recognized that during the past half century or more the epidemiological behaviour of poliomyelitis has been undergoing a certain amount of evolution, from a sporadic disease of infants to an epidemic disease of older children and even adults.
This transition, which seems to be linked to local “ways of living”, was apparently first noticed in Scandinavia, in the 1880’s; it was observed in other parts of Europe at almost the same time, and in North America shortly afterwards, i.e., in the early years of the twentieth century.
The first epidemics of poliomyelitis in a given area were often, but by no means always, sudden and large—so-called “primary outbreaks”—and they were usually followed by a gradual rise in the 5-year case rate, which might reach a level of from 5 to 10 times greater than that recorded in pre-epidemic days. What the story has been in the USA is illustrated in Fig. 1. However, evolutional experiences of this kind have not been universal, for in many parts of the world—notably in North and South Africa, Egypt and the Middle East, and in certain countries in Latin America—the transition from sporadic “infantile paralysis” to epidemic poliomyelitis has apparently not yet begun.
One clarification to add is that the designation of paralysis as a “sporadic disease of infants” was established by the retroactive identification of rare early reports of individual cases from back in the 1800s. The developing world, before the “switch,” preserved a vision of the disease in the pre-epidemic era as it probably had looked in the West. In 1943 in El Salvador,
It might be noted that the physicians of this country have considered poliomyelitis a rare disease and the great majority of them acknowledge that they have never seen a case, but there is no doubt that the disease has occurred here because occasional individuals of various ages are seen at times who exhibit the typical [signs of prior polio]5
Summary model, and a few other details of the problem
Here I leave the “default” model in certain points, which will be noted individually. In all cases, my personal corrections to the “default” model result from restoring a number of pre-vaccine-era insights that have since been discarded.
First I dispense with the hygiene hypothesis, as it is rather useless for the particular problem of polio (default model variance 16), and offer a crude model for a colder, not-too-remote, rural Northern area in which polio was always a bit sporadic, at least until the 1940s. Mostly the incidence of polio (shaded areas) is spaced arbitrarily, but note the (made-up) increase during the Civil War, reflecting a presumption of increased exposure to the virus from the South — and yet no paralysis epidemics were observed. Thus the change at all times after 1883 is not sanitation, nor decreased incidence of the virus, but the (mysterious) perpetual gain in overall susceptibility, which approaches 1/200 by the 1950s7:

Some final elements of the mystery, not at all comprehensive:
The “switch” or transition then began to take place in the (previously protected) developing world in the early 1950s, where only a few years earlier it had just been shown that polio virus immunity (and therefore infection) was widespread without any epidemics. Disentangling this transition from improvements in reporting is of course difficult; but examples such as Jamaica, where 752 cases in 1954 were recorded vs. a previous, long-standing trend of 2 to 13 per year,8 suggest the mid-century “switch” in paralysis susceptibility was real.9
The polio vaccines (injected or oral) meanwhile eliminated the “wild” viruses in most of the West, ending the possibility of further studying the natural behavior of the virus for example in America.
So what “switched”? Why did polio paralysis go from being so rare that if it happened at all, no one could be aware that a seasonal virus was involved, to (rare but still) common enough that the seasonal pattern was immediately noticed? What was actually causing this gradual gain in future susceptibility to a previously unnoticed virus among those who, at any moment, had not yet been naturally infected?
For that matter, why does paralysis during polio infection happen to begin with? As the opening quote from 2019 reveals, science still has little clue.
This is to say, is it in fact a problem of viral dissemination — through the bloodstream to the nervous system — after acute infection? This model is itself uncertain, as it is only supported by a limited amount of research, and not entirely consistent with the classic finding that paralysis accompanies the presence of antibodies, suggesting an immune reaction (default model variance 210).
Why were recent injections of various sorts eventually found to increase polio incidence in recipients? This was especially notable in two outbreaks in remote islands — Western Samoa in 1932 and Tahiti in 1951 — in which 1/12 of native children receiving recent injections experienced polio.11
Why did polio nonetheless still happen, predominantly, in those who were not recently injected (as far as was known)?
Why did polio affect the most energetic and stoic? It was observed consistently for 60 years that paralysis appeared more severely and permanently in those who were inclined to push through discomfort.12
Of course, I have already proposed my own answer to these questions, i.e. that the expansion of needle injections as medicine in the late 1800s was the “seed” of the mystery susceptibility factor. However note that I intend to rework the model of pathology, add more notes, etc., and as such will be publishing a new edition of the post shortly. But it is useful perhaps for the reader to consider this proposed solution while reading about the problem.
Finally, how does polio (naturally) spread?13 This mystery, however, is not particularly unique to polio viruses — similar gaps in our understanding still pertain to influenza and everything under the sun (default model variance 314). And so polio virus spreads by spontaneous teleportation from the void during nice weather, if you want.
ii. The Monster Slain Before It Could Be Understood
1931
One of the members of the colony [at Warm Springs] is a physician, a specialist in children’s diseases, who became ill in Rome and came back to the United States unable to walk. Another of the patients who is taking treatment this summer had infantile paralysis in Paris. […]
There is a youngster of eight with a brace on one leg who does a hop, skip and a jump every once in a while, telling the world he is getting better. A large delegation between 10 and 15 are just plain boy-roughish and sizzling with energy.15
Nothing about identifying the responsible virus, nor growing vaccines with it, changed the fact that polio was a mystery disease. How did it so selectively maim — leaving the majority of even overt patients otherwise unharmed, only robbing them of the power of their limbs?
Substantial advances were made in the understanding of polio immediately before the vaccines. And yet it would seem that nothing even like a glimpse of the solution to the great mystery had been achieved.
One looking back from today would tend to say that the research at the time, at least in the US, was seemingly focused on unleashing new technologies to learn precisely as many things as were needed to develop a vaccine that might be expected to work, and not one thing more.16 No one could even take pause to attempt explanation of why polio paralysis was suddenly appearing, in the 1950s, to get more out of hand than ever.
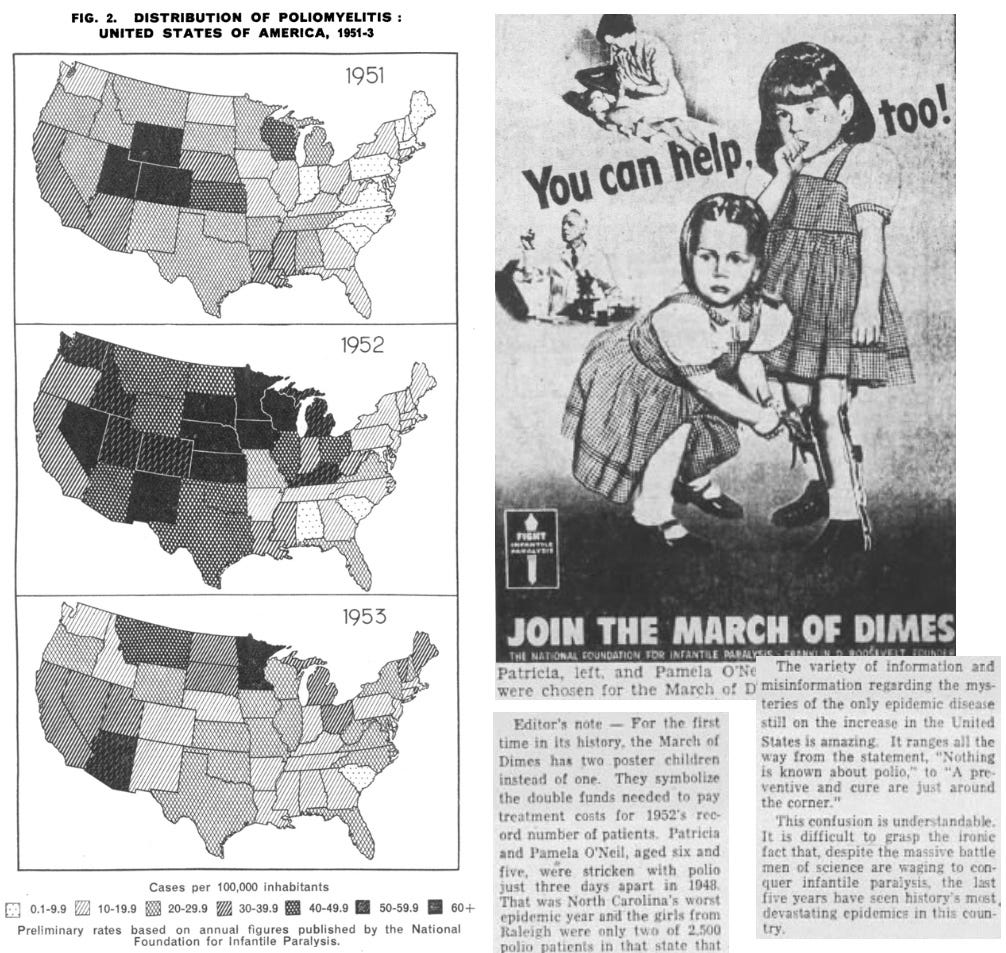
America saw a succession of the highest case rates on record after WWII, a trend observed at the same time in the United Kingdom and elsewhere.

And so just as medical experts sought to calm a panicked, post-War public with the reassuring information that polio virus infection is for most people a trivial event, which only very rarely results in paralysis, the information worsened. So much so that in 1953, the National Foundation added for the first time ever a second poster child, to advertise a need for twice as much funding.
Just another mystery. One that was easier, at the time, to quash rather than decipher — polio virus was killed before it (and the human factor) could be understood.
New advances in studying, but no time to wait and study
Along with several associates, three researchers in the 1940s had jolted polio research forward from the preceding decades of stasis. David Bodian had demonstrated that there were three types of polio virus. He, separately from and along with Dorothy Horstmann, demonstrated that the virus had a viremic phase (appearing in the blood) after it was fed to chimps by mouth, a feature that had eluded previous researchers because it likely takes place in humans before symptoms even appear. Meanwhile, antibiotics had ushered in the era of culturing viruses in cell tissue, and were especially helpful for more accurately recovering virus from feces and sewage — the home of polio. In 1948, John Enders demonstrated that polio viruses could be grown with this method, utterly revolutionizing polio research methods and quickly earning himself a Noble Prize.
All of these findings together were enough to create at least an argument, if not the wholesale expectation, that an injected, inactivated vaccine, the type being developed by Salk, would stop polio paralysis. The field test was launched a few years later in 1954, half a decade more quickly than was being predicted in 1950.
But what did this revolution do for actually understanding the same disease? Again, the answer would seem: Not much.
But we will see, in the upcoming revised edition of my own theory of the etiology, that a great deal of additional clues were collected with these new technologies in the few years immediately before the eras of Salk and Sabin.
In the meanwhile, what prevails is a rather sorry situation in which almost the whole of the “default” understanding of polio is a Frankenstein’s monster of inferences derived from the fact that the injected Salk vaccine appeared to work.
Some of the inferences based on the success of the vaccine affirmed things that had already been inferred based on the age and rareness of paralysis, and on widespread antibodies (most people’s blood protected monkeys from being infected by otherwise infective samples).
Some of these inferences sealed in quite recent reversals to long-standing understandings — and in this, the “default” model encodes errors that render it unable to solve the final questions.
But none of these inferences solved the biggest mystery. What was going wrong during infection? Why did the rate of going wrong increase in the late 1800s? The key to these questions — the monster itself — was now dead.
Given that the Virus Theory as stands is itself a lumbering monster scraped together from inferences about a corpse, one that still leaves so much unanswered, it is no wonder that outside thinkers might want to kill it with fire — scrap the whole model, and ascribe polio to some other secret cause.
And so, to sum up what the “default model” understands of the cause of paralysis in polio infection:
The virus enters the body and gets its first foothold somewhere. We aren’t sure. It is nonetheless considered an “enteric” virus, because the largest quantity of virus that comes back out does so in fecal matter.
For most people, the virus is eventually cleared without further complication.
The virus however tends to enter the blood before then, at least sometimes.
The virus infects (somehow) motor neurons in the spinal cord and brainstem, as these express the receptor for the virus. The ensuing destruction of these neurons, sometimes on a mass scale, severs the nerves responsible for sending signals to muscles of all sorts, including abdominal muscles and muscles of the respiratory system.
No explanation exists for why certain individuals are susceptible to this complication. (Or, it is because hygiene delays infections, although evidence does not in fact support this model of the etiology.)
All of this happens without substantial collateral viral destruction. For example, myocarditis was only a rare outcome of infection recognized very late into the polio era — but why rare? Why are not the heart and vascular system just as vulnerable to the virus as the nervous system, if neural invasion follows viremia but precedes antibody neutralization of the virus?
In conclusion, the default understanding of the pathology of polio is unsatisfactory.
iii. What polio wasn’t
1947
Case 9.—A paratrooper aged 19.
Day 1: From 11 p.m. the previous evening to 2 a.m. there was severe lumbar pain which kept him awake; he kept moving restlessly to change his position.
On getting up in the morning he felt shivery and had little appetite. Heavy training manoeuvres as usual during the day.
Slept well that night—no return of lumbar pain was noticed.
Day 2: He does not remember pain, but had some difficulty in getting down to fasten his boots in the morning. He still had little appetite and felt shivery. During the morning he took part in heavy infantry manoeuvres and carried machine-guns up a hill.
By 2.30 p.m. his legs began to feel weak and he noticed lumbar pain.
By evening both lower limbs and right arm were completely paralysed.
Day 3: The paralysis spread to his trunk muscles; there was some vomiting.
Day 4: Respiration failed—respirator required.17
But if I have proposed that polio was really so enigmatic, the reader may suppose instead that the same enigma is all based on some little misunderstanding; a statistical fabrication, or a simple historical force akin to Paul’s “ways of living” that demands no explanation. In other words, polio was not the mystery I say it was, but was just a trivial anomaly inflated by panic.
In this regard it is helpful to review things the polio mystery wasn’t.
It wasn’t misdiagnosis
This is the first thing to tackle, since anxiety over whether this issue has been taken into consideration seems often to make the reader hesitant to even consider any claim about a given disease. The short version of the answer is that in a study which will be discussed below, 84% of a sample of clinically-determined polio cases were found to be laboratory confirmed in 1954, suggesting misdiagnosis was not responsible for most recorded cases.
Researchers throughout the polio era were aware that not all polio cases were probably caused by the polio viruses specifically. Since paralysis had a million other causes, of course there was no way (from top-down, as a researcher) to exclude paralysis of other causes from being reported as “polio” in any data being examined and discussed.
The evident success of the vaccines is, of course, the default model’s closing argument that the killed monster — the three polio viruses to which the vaccines grant varying degrees of immunity — was in fact responsible for most cases.
We still might want for some kind of investigation of the question in the pre-vaccine era, and a few of these did take place, again as a result of the advent of cell culturing in the early 1950s.
A good example comes from the National Foundation’s18 field test of prophylactic “gamma globulin” in 1951 and 1952. After the initial run, all the “cases” in trial regions that had been counted and confirmed by normal standards, but exclusive of any non-paralytic patients, were double-checked using the newly available cell culture methods as well as newly improved serology (antibody measurement).19 The goal was to improve the accuracy of the reported trial results; but in so doing the accuracy of the clinical standard was also given close measurement. Again, the clinical standard in question was normal for the time. Physicians reported all cases of the age group in question to the trial operators, and the numbers listed in the trial reflect their tallying of this reporting. This is similar to how public health statistics on polio were typically collected (American statistics had separately tallied paralytic cases for some time_.
Previously clinically-defined cases would be considered laboratory-double-check-confirmed if either the patient were positive or a sibling was — i.e., if a paralyzed patient with a negative cell culture and serology’s sibling were positive for the virus, chances were good that the paralysis was from polio, and the cell culture for the patient was a false negative.
On grounds of isolation alone,20 control patients were positive for polio 68.8% of the time — and this was 93% of all “some type of virus” positive isolations.

Again, all of the above cases were brought to the attention of the trial operators by local physicians; the operators followed up even when patients had not been recruited for the trial (the “none” group). Counting positives inferred from antibodies, or results from siblings of patients, in the gelatin control a final 58 of all 69 clinically-determined cases — 84% — were considered verified as polio.21
This percentage can be inferred to apply to epidemic “non-paralytic” polio, which made up around half of reported cases a given year, based on the fact that seasonal surges in non-paralytic polio were never in disagreement with paralytic cases. (Such non-paralytic cases were diagnosed based on related clinical features and cerebrospinal fluid parameters.)

This is mostly important so far as so-called non-paralytic cases do not conceptually “dilute” the implied accuracy of paralytic diagnosis for being caused by polio virus.
Not-misdiagnosis: Replication
For completeness, a far-flung survey was conducted in Czechoslovakia in 1958-1960 in conjunction with the Sabin OPV program.22
Because of the sharp reduction in reported paralytic cases due to the vaccine, we should expect a higher hazard of “misdiagnosis” — and yet polio viruses were successfully recovered from 64.7% of 623 paralytic cases, a similar rate as in the gamma globulin trial (implying that adding serology-based confirmation would find over 80% of cases to involve polio virus).
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Andersen, NSB. et al. “Host Genetics, Innate Immune Responses, and Cellular Death Pathways in Poliomyelitis Patients.” Front Microbiol. 2019; 10: 1495.
Hammon, WMcD. “Immunity in Poliomyelitis.” Bacteriol Rev. 1949 Sep; 13(3): 135–159.
FDR’s illness was a textbook example of polio paralysis, and if you have read otherwise, it’s because the news reports on garbage studies. The ret-con of FDR’s diagnosis was achieved by literally plugging words into a formula and asking the formula what it thought.
Paul, JR. “Endemic and epidemic trends of poliomyelitis in Central and South America.” Bull World Health Organ. 1958; 19(4): 747–758.
Allwood-Paredes, J. “An Epidemic of Acute Anterior Poliomyelitis in El Salvador, C. A.” Am J Public Health Nations Health. 1944 Sep; 34(9): 941–947.
The “default” model is not really wedded to the hygiene hypothesis in the present day, but one may still commonly encounter general remarks associating sanitation with the emergence of polio in an off-hand and incoherent sense. But there have always been polio cases in conditions of poor hygiene during outbreaks, at least in the US, from the earliest cases in New England to post-War epidemics affecting shanty-town settlements in the Rocky Mountain states and Southwest. Sanitation and associated changes in mortality in the 19th century describe a technological shift in urban settings, and have little relevance for how people lived in rural areas — yet polio appeared almost simultaneously in both. Obviously, earlier exposure to natural virus leads to earlier acquisition of immunity, but this was always observed in association with warmer climate and crowding rather than sanitation per se; and fails to explain why susceptibility is “acquired” by those who on the other hand do not encounter the virus very early.
A conservative figure. The susceptibility factor may have been as high as 1% by the late 1940s, and perhaps higher afterward, based on statistics from the last epidemics. e.g., Melnick and Ledinko’s (1953; doi: 10.1093/oxfordjournals.aje.a119602.) modeling of the 1948 epidemic in Winston-Salem estimates that 1.6% of infections resulted in paralytic polio cases in the 5 - 9 year old group; my own hash of their math puts it at 1.1 - 1.2%.
Payne, AM-M. Freyche, M-J. “Poliomyelitis in 1954.” Bull World Health Organ. 1956; 15(1-2): 43–121.
In another example, the sparsely populated island of St. Helena experienced a polio outbreak in late 1945 (southern summer), in which only the (far more numerous) natives were affected except for one mild case in a British child. Native cases by either the paralytic or “abortive” definition were uncommon in individuals over 29, suggesting that this strain of the virus had been absent from the island for several decades, but before that time had at least paid a visit. Nonetheless, the paralytic form had not been previously noted — it was “unknown on the island within the memory of its oldest inhabitants.” Thus, the “switch” had taken place here as well, sometime between 1915-1945.
Nissen, KI. “Poliomyelitis on St. Helena.” Proc R Soc Med. 1947 Dec; 40(14): 923–932.
The “default” model of polio adheres dogmatically to the notion that neural invasion results from viremia, in absence of solid evidence and physiological plausibility. This insistence makes it impossible to explain demographic patterns in susceptibility. It is also so tenuously substantiated that any modern paper commenting on viremia will still reference work from seventy years ago, and ignore the true implications of the same work while doing so. There is nothing much to say here other than the evidence for paralysis following an immune reaction has always suggested pre-existing neural invasion, and my injection theory supplies the correct solution for the sequence of events.
Rosen, L. Thooris, G. “Poliomyelitis in French Oceana: Epidemiologic Observations of an Outbreak with Notes on the Incidence of Paralysis Following Intramuscular Injections.” Am J Hyg. 1953 Mar;57(2):237-52. doi: 10.1093/oxfordjournals.aje.a119571.
There were finally in the post-War era two good investigations on the topic of pre-paralysis exertion, though I have lost one of them. The other is
Russell, WR. “Poliomyelitis.” Br Med J. 1947 Dec 27; 2(4538): 1023–1028.
It is quoted elsewhere in this post for anecdotal adult polio experiences.
No infected-susceptible contact model can really be constructed out of observed patterns of viral shedding that explains all observed infections; nor does any sewage model satisfy the same problem. The disease from the earliest days was observed to occur in children with no recent contact with society at large. The best fit for observations — transmission of fecal residue by insects such as house flies — was always controversial at best, and suffered in plausibility by the failure of DDT to reduce case rates.
There are two historical modes to the “default” model regarding spread. In the pre-vaccine era, it was an incredibly central topic of investigation and discussion, for the obvious reason that if transmission were understood, perhaps infection could be curtailed or disarmed without a vaccine. This was all completely fruitless in the end. The modern “default” model is less concerned with the precise details of transmission but may still make statements on the subject that are overly certain, and discard past counter-evidence pointing to an essential mysteriousness of viruses. This, too, is just like influenza transmission.
Donnelly, Reinette L. “Happy Colony Located at Warm Springs.” The Macon Telegraph. August 16, 1931. p. 16. newspapers.com
Obviously a simplification, even though this is the narrative employed by David Oshinsky in reviewing the research effort of the time in Polio. But this era of research certainly had a bimodal character in terms of practical application. The work on pathology by Bodian et al., Horstmann et al., and Elliott substantially corrected Flexner’s misconceptions without leading to any practical application, only reaching the cusp of a true understanding. The progress in brute “grow and kill polio viruses” methodology was far more rapid and tangible.
Russel, WR. “Poliomyelitis; the pre-paralytic stage, and the effect of physical activity on the severity of paralysis.” Br Med J. 1947 Dec 27; 2(4538): 1023–1028.
i.e. the National Foundation for Infantile Paralysis, which funded most research on polio outside of that undertaken at Rockefeller Institute.
Hammon WM, Coriell LL, Wehrle PF, Stokes J Jr. “Evaluation of Red Cross gamma globulin as a prophylactic agent for poliomyelitis. 5. Reanalysis of results based on laboratory-confirmed cases.” J Am Med Assoc.1954 Sep 4;156(1):21-7.
Secondary isolations were attempted in cell-culture negative cases, and these second attempts typically used monkey inoculation, which at the time was typically more sensitive than cell culture.
This is reinforced by the difference in “no virus” cases in the treatment group — these 9 fewer “no virus” cases were probably prevented polio virus cases. Assuming also that some “no virus” cases were non-prevented polio (because the treatment obviously wasn’t perfect in stopping culture-positive polio cases), the expected amount of false negatives matches what was classified as a case using serology and siblings.
Žáček, K. et al. “Mass Oral (Sabin) Poliomyelitis Vaccination in Czechoslovakia.” Br Med J. 1962 Apr 21; 1(5285): 1091–1098.
Thank you for this deep quality analysis!
Comments so far -- the mystery that inspired a million Clouseaus... brilliant...