
The (Not-An) "Imprinting" Study
Why Reynolds, et al. doesn't say that much about post-Omicron immunity for the Covid vaccinated.

A bewildering paper published in June turned “imprinting” into the phrase of the summer, igniting a yet another round of claims that the Covid-vaccinated cannot develop memory to new variants of SARS-CoV-2.
However, nothing in the study design supports the conclusions offered by the authors or others who echo them.
The following post attempts to demonstrate the paper’s fundamental limitations, as a reader service. To save time, just don’t pay attention to the paper or listen to anyone representing its findings as significant, because the whole thing is a dog’s breakfast.

Background
For readers who missed it, I have given my thoughts on a different paper, one that actually does show a relevance to “imprinting,” in a previous post. The hyper-cross-immunity generated by the mRNA injections appears to leave recipients stuck with their original memory B Cell pool (even if re-shuffling that pool effectively neutralizes new variants). This is the same B Cell pool seemingly trapped on the “raft” toward IgG4 tolerance:

So the following post, reviewing the “not-an-imprinting” study, is not merely an attempt to always be as contrarian as possible when it comes to “Original Antigenic Sin” and all its rebrandings. Rather, one of the fundamental aims of this journal is to offer the reader demonstrations of when published research is just as willing to deceive via half-truths and montage as a Soviet propaganda film, or even the mainstream media.
Whether upholding the “safety and efficacy” of vaccines one day or suggesting dire, mythical negative consequences to them the next, publication bias and self-deception render the conclusions declared by authors a gross misrepresentation of their own findings just as often as not. Meanwhile, said actual findings are often semi-impossible to evaluate except in the highly processed and curated form offered by the same authors.
Such is the case with Reynolds, et al., where the deception starts right in the title.
Here, the paper:1

The study mostly involves healthcare works (HCWs) in London immediately before and then during the BA.1 “Omicron” wave. Serum samples are taken at myriad time points, and subjected to tests for antibody or cellular responses against different SARS-CoV-2 variants.
Here, the design. There are 6 major “modules” deployed and reported:
The reader is encouraged to observe the following quirks:
Not a whole lot of ‘Cron
Of the 6 study modules, only 3 pertain to actual (possible) Omicron (BA.1) infections, and for these, a mere 17 infections are observed. But the title, “boosting by Omicron,” obviously sets even an experienced reader up to expect that all results will pertain to Omicron infections. Additionally, the only method of ascertaining that these were “Omicron” (BA.1) infections to begin with is date of positive PCR.
No unvaccinated controls
What’s more, there are no unvaccinated control subjects in any module, and yet the study claims to be measuring the impact, primarily, of the “previous SARS-CoV-2 exposure” of Covid-vaccination (with or without additional exposures via infection).
Tiny sample set
Lastly, in so far as the paper will compare “exposure combinations” with each-other, the small sample size and likelihood of presenting coincidental findings as significant (“false discovery”) jumps off the page.
The Non-’Cron Parts
And so, if you have already been exposed to a review of this paper (unless by Modern Discontent’s excellent post), it was likely one that incorrectly interpreted modules 1 and 2 as reflecting Omicron infection results.
This includes, for example, the review by Robert Malone, which begins immediately with the (understandable) misapprehension that module 1 concerns post-Omicron-infection responses:2
B cell immunity after three vaccine doses
Health care workers (HCW) were identified with mild and asymptomatic SARS-CoV-2 infection by ancestral Wuhan Hu-1, B.1.1.7 (Alpha VOC), B.1.617.2 (Delta VOC) and then B.1.1.529 (Omicron VOC) during successive waves of infection and after first, second and third mRNA (BioNTech BNT162b2) vaccine doses. By three vaccine doses antibody responses had plateaued, regardless of infection history. We found differences in immune imprinting indicating that those who were infected during the ancestral Wuhan Hu-1 wave showed a significantly reduced anti-RBD (receptor binding domain) titer against B.1.351 (Beta), P.1 (Gamma) and B.1.1.529 (Omicron) compared to infection-naïve HCW.
Simplifying, if you were first infected with Wuhan Hu-1, then vaccinated, then infected with Omicron, your antibody levels against the important part of Spike (the receptor binding domain) were lower than those who had not been infected.
Again, an understandable misapprehension, because like so many papers the seeming intention with Reynolds, et al. is to be misapprehended. In the quoted wall of text from the study itself, no effort is levied to make it clear that the “boosting by Omicron” just referenced in the title is not being considered in these first-discussed results. Instead, the authors are bizarrely looking at anti-Omicron immunity at various time-points after mRNA vaccination for individuals who haven’t been exposed to Omicron yet (because it didn’t even exist at the time).3
And so if the question is, will the Covid-vaccinated develop an immune response to new variants, including the Omicron siblings? - no aspect of modules 1-2 can be taken as instructive save for the following: Was infection with Delta followed by higher anti-Delta response than “back-boost” of anti-Wuhan response (since the timing for Alpha infections is inscrutable)?
Here, S1 binding, neutralization assays (Fig 1), and T Cell responses (Fig 2) return results in favor of both yes and no. The sample size is only 6.
As for the mouse results in module 3, not much needs to be said. T Cells sensitized to Wuhan peptides react to Wuhan peptides; those sensitized to BA.1 react to BA.1. No surprise - and not even the authors seem to be able to spin this into any implications for immunity against future variants.
The ‘Cron Parts
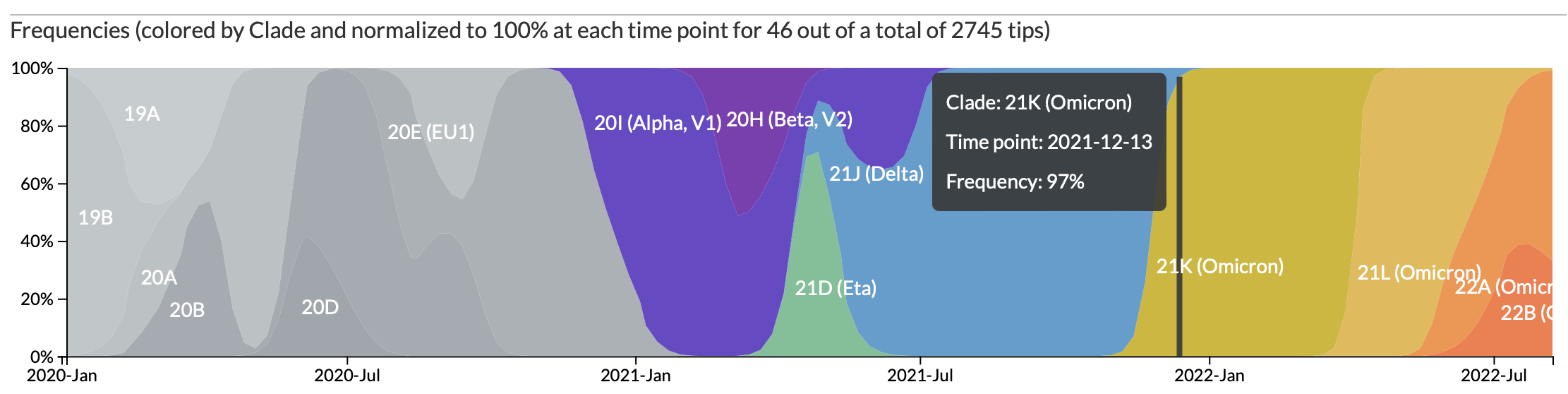
39 London healthcare workers were recruited again in January, in the middle of the UK’s BA.1 wave. The earliest PCR-positive for “B.1.1.529 wave PCR positives” in this group is December 13, when Delta was all but extinct in England:
8 of these healthcare workers, including 7 PCR-positive during the “Omicron wave,” are excluded for not being triple-Pfizer-dosed (3) or otherwise unclear reasons (5; perhaps prior Alpha or Delta infection).
This leaves 17 presumed-Omicron-infected 3-dosed healthcare workers being compared with 15 presumed-not-Omicron-infected. If the question were, “How does the immune response to Omicron depend on prior exposure to the Covid vaccines?” -
- Uninfected, but Covid-vaccinated subjects cannot shed light on the answer. Just as how the response to “being punched on the nose” “depends” on “being rich” requires comparing how the poor react when punched on the nose, not how the rich react when not punched on the nose.
As the latter is what this study offers, the Covid vaccines themselves are not being evaluated in any sense, and do not count as a “previous SARS-CoV-2 exposure;” only the supposed influence of infection on the triple-injected is being measured. Who asked for this? Could the authors really imagine their study would not be read and quoted more broadly?
Anyway.
The authors find:
For Covid-vaccinated who were not previously infected, presumed Omicron infection appears to boost anti-Wuhan antibody responses more than anti-Omicron responses, although the latter is higher among the non-Omicron-infected; T Cell responses against Omicron don’t appear to expand at all.
Meanwhile, Covid-vaccinated previously-infected in March or April of 2020 show almost no increase in Omicron-specific response.
Both these conclusions are strongly limited by early sampling post-infection, with “Week 94-96” recruitments striking at arbitrary post-PCR-positivity intervals; and again the lack of comparison with unvaccinated Omicron infection responses. Whether for antibody, B Cell, or T Cell dynamics, later sampling would provide a more accurate view of novel immune response.
The former point would count as a fairly classical “demonstration” of “OAS.” However, as with another recent study,4 the results are potentially misleading due to early serum collection that predates any possible generation of novel B Cell / IgG antibody responses.5
Moreover, the exclusive examination of (not-too-recently) triple-dosed subjects in Reynolds, et al. leaves no way to distinguish between antibody results driven by lifetime quantity of exposure to the Wuhan spike, rather than sequence of exposure. And once again all conclusions regarding how the Omicron response “depends” on prior Covid triple-vaccination are wild speculations at best, in the absence of an unvaccinated control group.
As for the second bullet, it is here where the paper’s results really do turn striking: Among subjects who were recorded as being infected in March or April, 2020 and went on to be triple-injected with the Pfizer Covid vaccines, post-Omicron infection responses against Omicron appear abysmal.
Of course, the small sample size of 6 leaves this result even more vulnerable to flaws in how infection is classified - but as N antibody levels jump on week 94-96 vs. 83-84, it would seem that these are authentic reinfections with Omicron. But even if N antibodies betray the “failure” of natural immunity to prevent infection with presumed Omicron outright, the protection against reported symptoms seems robust:

And once again, given a more reasonable period between infection and sample collection, the “Wuhan”-infected + triple-vaccinated may show a more robust anti-BA.1 response.
If I had to speculate, what is actually being observed by Reynold’s et al. in this portion, is that natural infection before mRNA vaccination reduces the immune response to vaccination itself, including the “front-loading” of B Cells that bind to future variants observed by Röltgen, et al. (once again mentioned in the previous “imprinting” post).
For this reason, an early sampling of “Omicron breakthrough” infections will find memory immunity expansion against Omicron to be low, but substantial in the not-previously-infected-mRNA-vaccinated, and non-apparent in the natural-infected-mRNA-vaccinated (who either need time to develop new B Cells and antibodies against BA.1, or are so well-covered by non-spike and cellular-directed responses from their natural infection that no new immune response is required).
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Reynolds, CJ. et al. “Immune boosting by B.1.1.529 (Omicron) depends on previous SARS-CoV-2 exposure.” Science. 377, 275 (2022) 15 July 2022.
Malone, Robert. “Immune Imprinting, Comirnaty and Omicron (part 2).” (2022, June 25.) Who Is Robert Malone.
Why? Well, you could answer, because “exposure” histories are taken to shape immune response, and binding against a future variant is if nothing else a way of measuring those shaping effects.
Except, this would simply be a straight-forward restatement of how memory immunity is understood to work: By remembering things (that resemble other related forms of things). As always in “OAS world” the goal of parading out the archeology of this immune memory is to then insinuate a “stain” (“imprint”) that will hinder the immune response to future variants. So it is here, even if the “O” phrase is never dropped (an earlier paper in the series does use “OAS”). The logical structure of the text is unmistakeable: These individuals are in some way being limited by their “imprinting.” They are experiencing “Hybrid immune damping.”

And so for:
Triple vaccinated [healthcare workers] with different SARS-CoV-2 infection histories show boosted cross-reactive immunity against VOCs, less so against Omicron.
- Is it really an “accident” if the reader mistakenly believes that the results summarized in (A) are also for “different” infection histories that include Omicron infection? Again, a headline immediately precedes the results that is only applicable to the (explicitly) post-Omicron-breakthrough results in (B) alone. The only reason I have been able to make any sense of the design at all is my superhuman hatred of all things OAS.
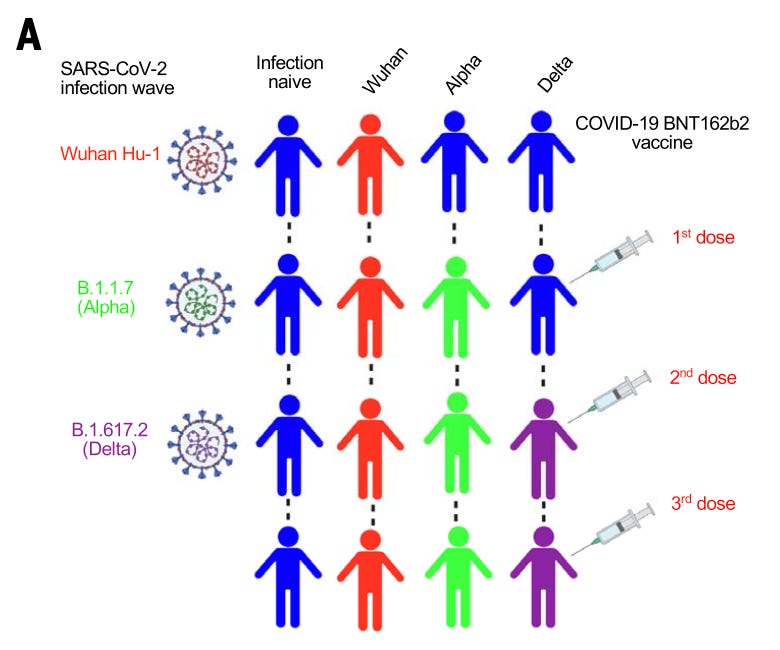
Deception via absence is compounded by confusion via abundance. Instead of a simple, text based flow diagram as I have produced above, the authors produce the following monstrosity in which it is impossible to tell whether injections precede or follow Alpha and Delta infections:
Finally, this ostensible comparison of inter-exposure cross-immunity against (the future variant) BA.1 is unnecessarily and confusingly described in relation to the variants being encountered, leading to abundant and misleading use of “reduced” to describe antibodies or cellular responses against Omicron in individuals who haven’t even encountered it yet.
Furthermore, immune imprinting after B.1.1.7 (Alpha) infection resulted in reduced [compared to what?] durability of antibody binding against B.1.1.529 (Omicron), and S1 RBD and whole spike VOC binding correlated poorly with live virus nAb potency. Half of triple-vaccinated HCWs showed no T cell response to B.1.1.529 (Omicron) S1 processed antigen, and all showed reduced [compared to what?] responses to the B.1.1.529 (Omicron) peptide pool, irrespective of SARS-CoV-2 infection history. […]
We found differences in immune imprinting indicating that those who were infected during the ancestral Wuhan Hu-1 wave showed a significantly reduced [compared to what?] anti-RBD titer against B.1.351 (Beta), P.1 (Gamma), and B.1.1.529 (Omicron) compared with infection-naïve HCWs [oh!] […] However, cross-reactive S1 RBD immunoglobulin G (IgG) antibody and nAb IC50 against B.1.1.529 (Omicron) were significantly reduced compared with the other VOCs, irrespective of previous SARS-CoV-2 infection history [Great! Now just give me nine hours to “redu” all your work to understand why these two back-to-back but non-parallel ‘reductions’ are anything more than publisher-bait!]
Intervals, PCR+ to sampling for not-previously infected “Omicron” wavers; Wuhan/BA.1 titer
ID011 Dec 27 PCR+, Jan 7 sample: 11 days; 290179/75464
ID013 Dec 29 PCR+, Jan 6 sample: 8 days; 430958/117978
ID019 Dec 20 PCR+, Jan 7 sample: 18 days; 324762/75579
ID023 Dec 29 PCR+, Jan 12 sample: 14 days; 553981/131700
ID025 Dec 22 PCR+, Jan 10 sample: 19 days; 476124/125510
ID036 Dec 19 PCR+, Jan 10 sample: 22 days; 1602307/185163
ID038 Dec 18 PCR+, Jan 24 sample: 39 days; 834921/186899
ID064 Jan 8 PCR+, Jan 21 sample: 13 days; 440358/105935
ID072 Dec 21 PCR+, Jan 6 sample: 16 days; 1066535/240809
ID077 Dec 22 PCR+, Jan 12 sample: 21 days; 449839/92170
ID085 Dec 29 PCR+, Jan 10 sample: 12 days; 419348/110253
This can be contrasted with the “imprinting” study conducted in-house by BioNTech: All samples were taken 44 - 46 days post-infection, and neutralization vs. BA.1 was just as high as vs. Wuhan.

In general it really is strange how such studies are being used almost like reading tea leaves and predicting. Yeah, Wuhan spike vaccines will boost Wuhan more than Omicron, which we know is already a pretty big escape variant and yet we are shocked. I think the biggest problem with these types of studies is that it muddies the waters even further. It's another example of trying to extrapolate and argue in favor of OAS but in a manner that's super messy, and in the end just makes you scratch your head more than understand how the researchers came to such conclusions.
Thanks once again Brian! I hate bullshit, whether it comes from the pro mRNA vax side or from the opponents. It's so destructive. It's actually stunning how shoddy is the thinking on so many publications.