


The Germany "Impaired Immunity" Study
Over half of volunteers in Germany's largest state appear to... still not have been infected yet.

Study Review: Dewald, F. et al. (2023)
A pre-print from North Rhine-Westphalia presents results from 1,411 adult donors surveyed during emergency room visits in the early part of Germany’s recent BA.5 wave (but regardless of current infection status).
The study:1

Key takeaways:
The title is completely misleading. Immunity is “impaired” because none of the participants would yet have encountered BQ.1.1; and only a very few BA.5 (and those individuals are not examined separately).
Less than half of volunteers self-report previous infections. In August, 2022! Talk about flattening the curve(s).
The interesting results are not broken down by vaccine status. But, the group as a whole can be taken to generally represent antibody status among the Covid-vaccinated since only 5% of donors are unvaccinated.
Among infection-reporters, no sign of Nucleocapsid antibody deficiencies.
Still no support for everyone else’s claim of negative efficacy from multiple shots, which thus supports my claim that the Cleveland Clinic boosters study is just showing a catch-up effect.

The Set-Up
Dewald, et al. “measured SARS-CoV-2 Spike/Nucleocapsid seroprevalence and serum neutralizing activity against [ie., in vitro cell protection by donor samples vs. a pseudovirus with spikes for] Wu01, BA.4/5 and BQ.1.1 in 1,411 individuals who received medical treatment in five emergency departments in North Rhine-Westphalia, Germany [between August and September].”
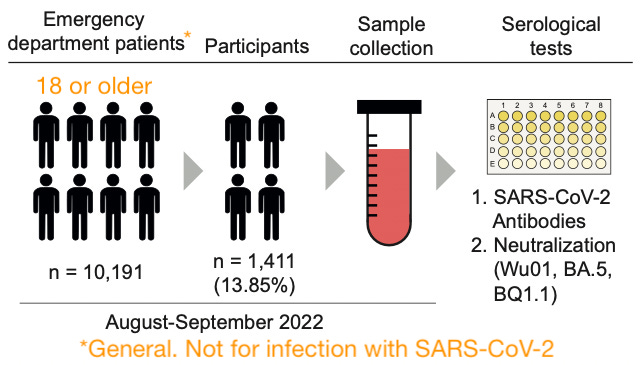
You would think (given the title) the authors might have focused on the contemporarily infected; you would be wrong. It’s just people in the emergency room “for whatever.”
Only ~320 (i.e. 23%) of the 1,411 volunteers report infections within the last 5 months.2 The results are thus more a survey of the past than of outcomes for the currently infected.
Most of what the study reports is not interesting.
So why highlight it? Just to save the reader time in case someone else later turns the study into click-bait (including by not even realizing the subjects are mostly never-infected).
Results
i. Less than half of volunteers self-report previous infections.

In fact, it turns out that Dewald, et al.’s emergency-room visiting volunteer donors astonishingly mirror overall official case counts in Germany almost exactly (case counts equal 45% of the population).
Since there will be biases in multiple directions at once — and overall cases and rates of individuals having at least one case are not even the same thing — this is mostly just a curious accident.
However, it appears to affirm that Germany, like other lockdown-conformist countries, really is quite far behind on natural immunity:

The above splash also shows there are still extreme limits to inferring whether constant, unending waves reflect “negative efficacy.” What is really happening is that the cases keep reversing well before any given wave has substantially reduced the natural immunity gap.
These perturbations to what we might call “natural” seasonal wave patterns, the first of which was observed in the UK starting in summer, 2021, may still simply result from the hyper-vaccinated offering the virus a “slow drip” of susceptibles as temporary infection efficacy wanes and then is re-upped by boosters on an individual basis.
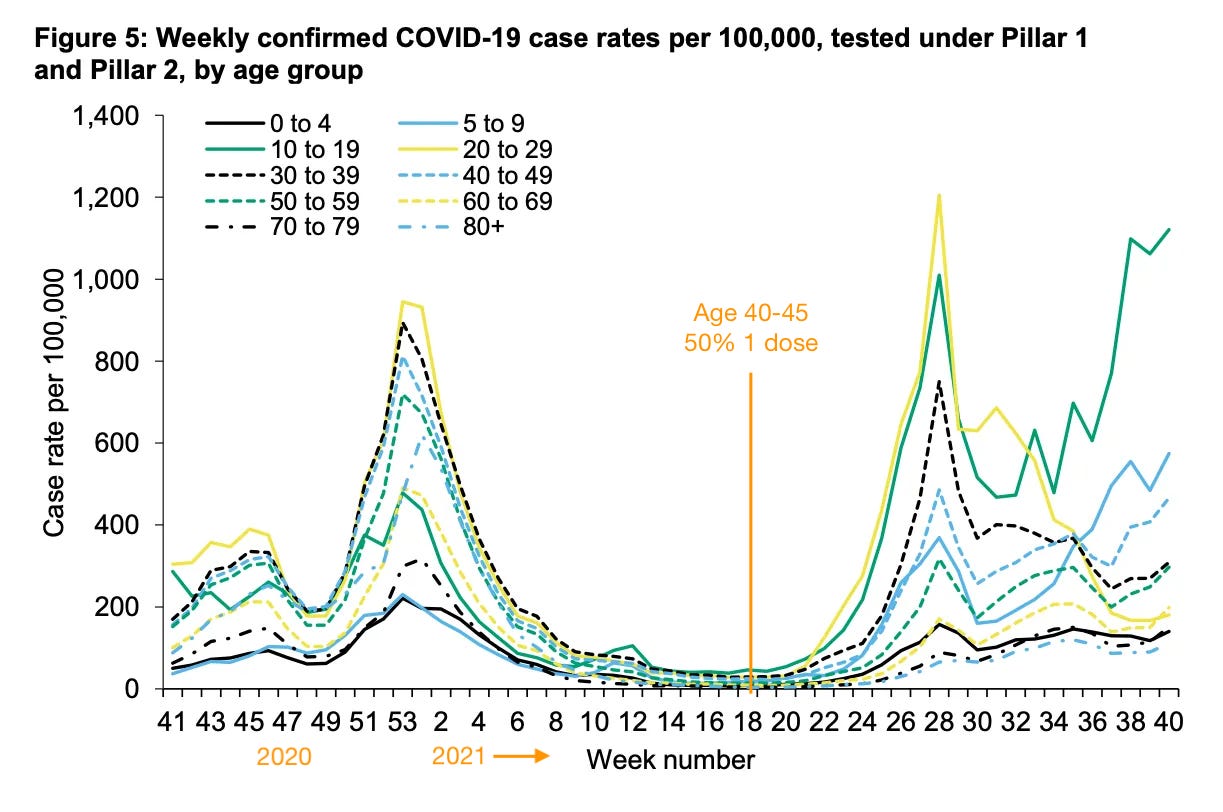
A revisit of my assets from late 2021 finds easy support for this explanation. Before the Covid vaccines, case rates in different age groups were in sync. Afterward, they fluctuate wildly, as the old and young trade places being more and less susceptible to the virus:
Dry tinder? The paradox of Germany (and other natural-immunity-poor countries).
The paradox that arises here, just as in the Cleveland Clinic boosters study, is that Germany is having more cases because it has had less. (The 74 unvaccinated appear to be 81% spike-seropositive;3 this likely reflects a bias for previously naturally immune to forgo and seek exemptions to vaccine requirements.)
This suggests a deficiency of natural immunity (i.e. immune debt); but it also begs the question of whether what is actually happening is that Germany has more innate immunity. Like other regions (e.g. California), it has seemed resistant to the virus in ways not explained by policy, demographics, etc.
The question thus arises if, eventually, SARS-CoV-2 becomes resilient enough against temporary post-infection efficacy that all of this immune debt must be paid up at once — Germany must have a super-wave. It keeps seeming like hyper-vaccinated countries are on the verge of such an event (as Japan has been several times, including now), only for cases to reverse once again well before most people have natural immunity.
One can only speculate. Whatever happens will happen.
All that is really necessary to say here is that it is still possible that negative efficacy is true (the Covid vaccines are eroding innate immunity, leading those who would never have been infected to eventually become infected, and driving forever-waves), but that these kinds of paradoxes work at cross-purposes so that there is no evidence for negative efficacy (the Covid vaccinated have less cumulative infections than other groups).
Moving on.
ii. In accordance with low infection rates, N antibodies are low; but not in a way that suggests inability to make N antibodies.
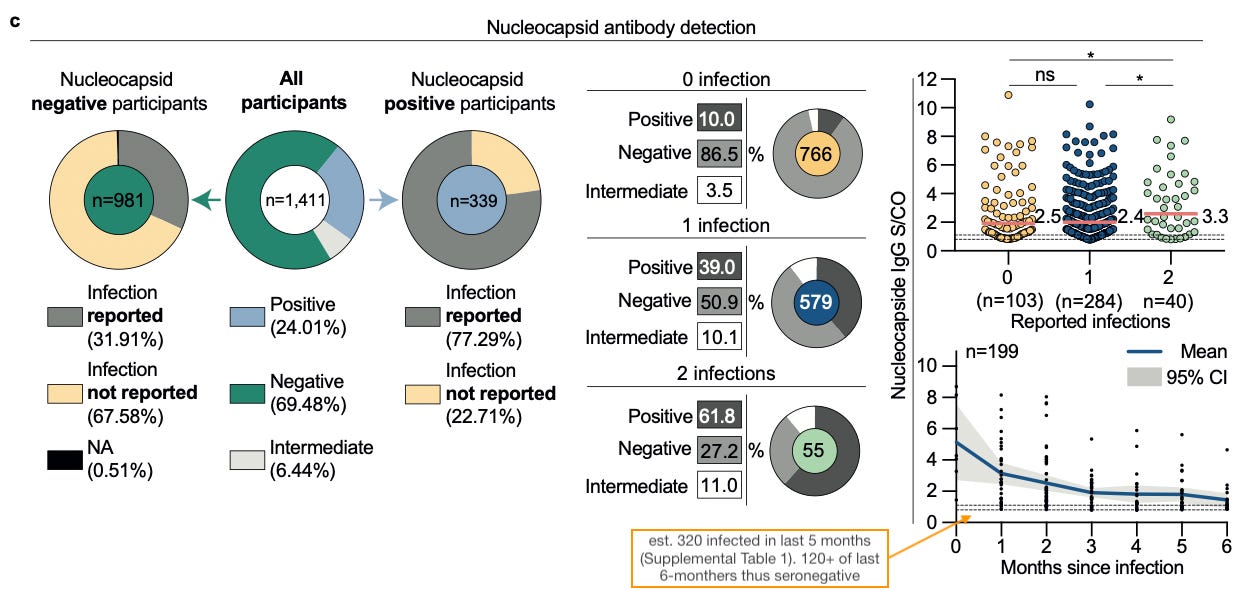
Most importantly, in considering the Nucleocapsid-negative in either the by-N or by-infection pies (left and middle), months since reported infection (bottom right) seem to depress N-seropositivity.
This suggests, first, that N antibodies are simply fading out, rather than never being generated in the first place (antibodies fading out is normal); and second, that successive increases of Covid-vaccine-injection has not depressed N seroconversion (which would be expected if the vaccines were somehow magically able to make the immune system indifferent to the Nucleocapsid protein).
Of course, one could still try to rescue the trope that the Covid-vaccinated can’t make N antibodies by claiming that Omicron is the exception that proves the rule (thus explaining the months since infection trend). As always, I refute this.

Regarding the plot on the top right, it shows that not much difference exists between N-positivity in the 50% of 1-infection-reporters who are near or above the cutoff as for the 13.5% of no-infection-reporters who are near or above cutoff. All that this shows is that asymptomatic infection probably does not drive low N positivity rates (since one would expect a difference between these two groups if that were the case). However, this is not important, since it already appears that low N positivity rates are driven by antibody fadeout over time.
iii. Dry Tinder Pt. 2: Hyper-Wuhan-injected, mostly uninfected Germans do not magically have high anti-BA.5 or -B.Q.1.1 immunity.
Incredibly, given that only 320 or about 23% of the volunteers in this study report being infected in the last 5 months,4 rates of immunity to current strains are low.
Ah!!! It’s OAS!!! (OAS is not real.)
Uncovering this fact is essentially the entire purpose of Dewal, et al.’s antibody survey: “Look at German antibody rates; no one has immunity for the variant that is coming in the next wave.”
But this doesn’t make the fact surprising (or unobtainable with a simple Google case rates search), given that (injected) exposure to the Wuhan spike has been abundant, whereas exposure to BA.5 has been limited to a single wave (which was still only gaining steam during the study period).
Hence why they report in no uncertain terms (emphasis added):
We could not differentiate the immune escape to infection-induced antibody response and/or antibodies induced by mono- or bivalent vaccinations.
And so once again it could be the case that a “super-wave” is imminent, if the previous ability of the Covid vaccines to stave off infection suddenly evaporates overnight thanks to B.Q.1.1. or whatever new scrabble variant shows up instead.
But in that case, both Germany’s natural immunity debt and “Omicron variant immunity debt” would solve themselves.
At all events, the authors, despite being employed in the wrong end of Deutschland (perhaps some were patriotic transplants), produce this impressive, traditional Bavarian Boy Camouflage Device to show that BA.5 immunity lags far behind Wuhan-variety.

If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Dewald, F. et al. “Impaired humoral immunity to BQ.1.1 in convalescent and vaccinated patients.” medrxiv.org
Based on the median time since infection being about 5 months regardless of total infection count, per Supplementary Table 1. So, I simply multiplied the total number of previously infected by .5.

Fig 2a implies that only .32 x 44, or 14, of the (not immune-suppressed) spike seronegative report 0 previous antigen encounters. Since Covid-vaccination counts as a reported antigen encounter, this implies that around 60 of the 74 self-reported unvaccinated (Fig 1f) are spike-positive, i.e. previously infected. This means the unvaccinated have a 81.1% prior infection rate vs. 44% of the Covid vaccinated.
See footnote 2.
I find this study to be difficult to believe. The only people I know who did not have Covid yet are my parents who are Covid conscious and stay home a lot.
Literally everyone else I know had Covid.
And they are telling me that half of a German region did not have Covid?
"Never infected"
Are these numbers accurate? By Nov 2022, 94% of Americans were infected by SARS-CoV-2: https://doi.org/10.1101/2022.11.19.22282525
Infected with SARS-CoV-2 isn't the same as "had Covid-19" right? Personally, I don't think I ever had Covid-19. I'm late 20s and every time I was around someone sick that tested positive I took a lot of vitamins and hoped for the best. Aren't most infections asymptomatic? In which case, these people are [at least someone] immune already, or developed it without getting sick?
Or are these high infection estimates inaccurately inflated?