


The Thailand myocarditis study, briefly
3.5% of boys show evidence of pericarditis or myocarditis after the 2nd dose of the Pfizer/BioNTech Covid vaccine. (A belated recap.)

Update, 8/17/22: Additional comments have been added to the section on ECG abnormalities, thanks to Stephanie Brail’s remarks on the study over at Wholistic.
Update, 9/20/22: Discussion of the potential for a more widespread subclinical myocarditis rate has been updated as noted below, thanks to raw data acquired by Jonathan Engler, who writes at PANDA Uncut.

Although Vinay Prasad has already provided a somewhat-punch-pulling recap of the preprint study from Thailand,1 it hadn’t received a lot of attention in the more anti-mainstream edges of the substack ecosystem. This changed a few hours ago with a somewhat-too-sensational Steve Kirsch post.2 My overview is at best a “middle-chair” summary at this point.
Still, it would be odd not to offer a take here, given that this journal keeps the myocarditis issue on the radar generally,3 and this study is groundbreaking in that it shows rates of post-mRNA-injection myocarditis in teens captured by actual screening, eliminating under-reporting and capturing subclinical (non-symptomatic) heart damage. And so here goes.
The Set-Up
The study:4

314 teens already first-dosed with the Pfizer/BioNTech Covid vaccine (BNT162b2), and without prior cardiac issues or adverse reactions, were tested for cardiac markers before and then 3 and 7 days after receipt of the 2nd dose (and again if presenting with cardiac symptoms). Emphasis added:
High-sensitivity cardiac troponin-T assay (HS-cTnT) and CK-MB isoenzyme levels were determined for all participants at baseline, and on Day 3, Day 7 and Day 14 (optional) after the second dose vaccination. HS-cTnT was measured using the Elecsys troponin-T hs assay (Roche Diagnostics, Mann- heim, Germany); serum levels > 14 ng/L were considered elevated.
“Elevated” troponin, in the context of suspected myocarditis (i.e., not in the context of a heart attack or sepsis or other obvious trauma), clinches the diagnosis.
Not only does this study screen for myocarditis, to find cases in teens that would otherwise be missed in a clinical setting, it also collects a baseline measurement to observe the change driven by the mRNA injection. This makes it a first.
For context, previous estimates of post-Covid-vaccine-dose-2 myocarditis have been implausibly low. Even the values derived by Høeg, et al. - which set off a firestorm of MD-twitter criticism by almost doubling the CDC’s official rate5 - are minuscule when converted to percentage form.

“.016%” is not what the Thailand study found.
3.5% Peri/Myocarditis in teen boys
Minus 13 subjects lost to follow-up, there were 99 girls and 202 boys tested this way overall. No girls presented with cardiac complications or threshold-defined “elevated” troponin-T findings. 3 boys presented with symptoms and an additional 4 were flagged for elevated troponin-T (following a normal baseline).
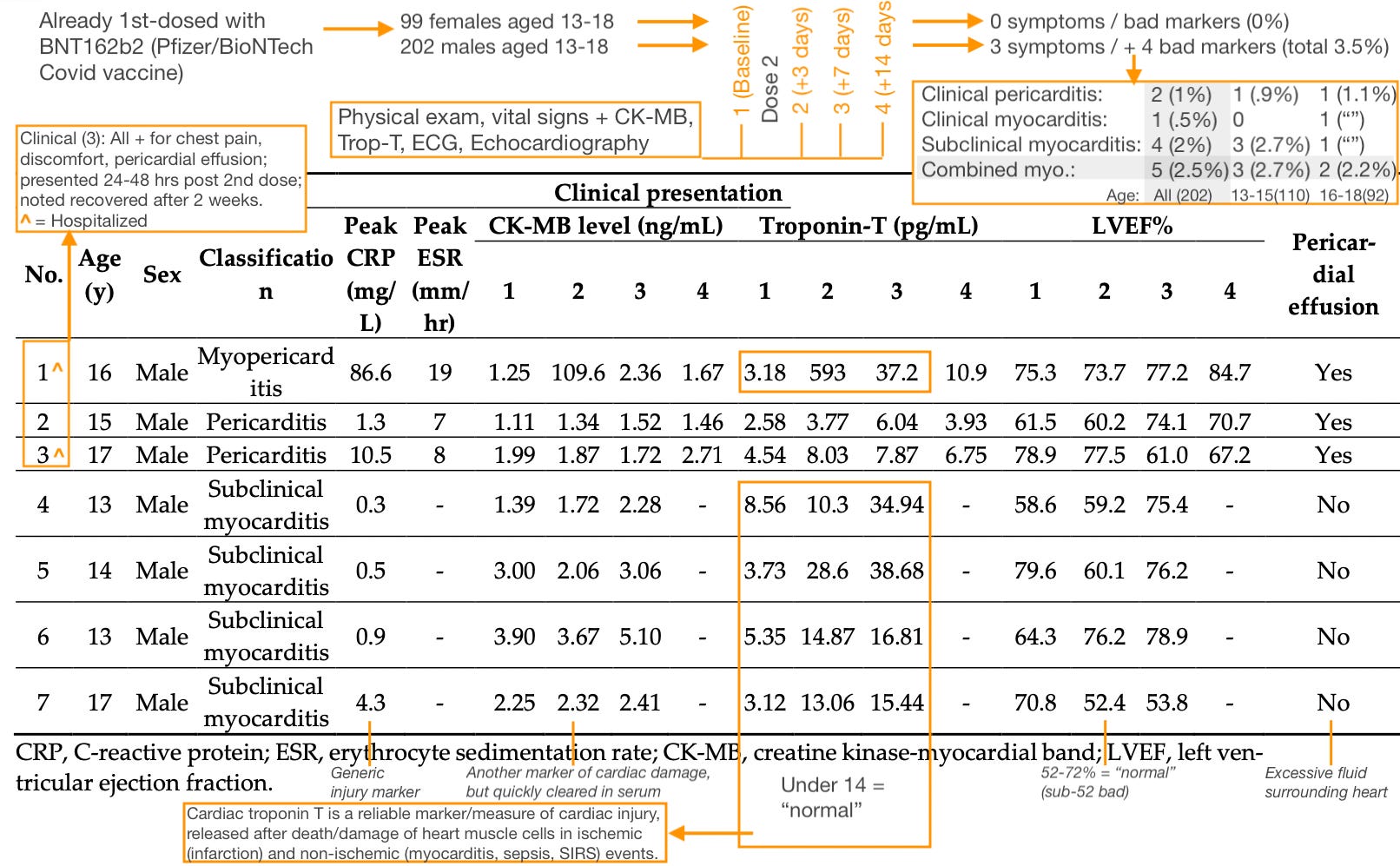
Using the 14 pg/mL threshold, the combined (clinical and subclinical) rate of myocarditis is 2.5% for all boys observed. This rate is similar in both the 13-15 and 16-18 age groups. Separately, the pericarditis rate is similar in both age groups as well. This consistency is impressive, despite the hazard of extrapolating from only a handful of events.
Expected background rate?
Of course, studies which do not include controls burden the reader with having to bring their own knowledge of the expected background rate of whatever is being measured; in this case subclinical myocarditis in teen boys in Thailand. Naturally, each subject’s visit 1 (baseline) value serves as a self-control: They are not showing elevated troponin-T before the 2nd dose; and near-or-above-14 results are returned on both post-dose visits for each boy afterward.
Additionally, the lack of any over-threshold results among the 99 girls serves as a control in the context of this specific study’s assay (Roche Elecsys6) and method. By definition, "background rates" for any threshold on a given assay vary with the population being tested - but the results among girls demonstrate that a return of 0 is possible (even after mRNA injection). In a population of healthy7 boys with sub-14 baseline values, it seems safe to treat the expected background rate as 0.
Un-measured 1st dose effects
Because the study intervenes on subjects who have already received 1 dose, “baseline” values provide a muddy picture of true before-mRNA-injection levels vs. already-fading cTnT release from dose-1-induced cardiac damage. As illustrated by subject 1 in Table 3 above, cTnT tends to linger in serum for over a week, due to slow breakdown (proteolysis).8 Depending on the duration of cell damage induced by mRNA-vaccination, cTnT elevations after the 1st dose may be sustained for longer than after an acute event (due to continual release).
It could thus certainly be the case that the baseline values in Table 3 offer a glimpse of post-dose-1 subclinical myocarditis (implying that immune sensitization is not the primary etiology for myocarditis, which is what I am inclined to believe; instead, damage during dose 1 merely raises the baseline of damage and patient awareness so that additional damage is more likely to advance from a subclinical to a clinical level).
In Table 3, subject 4 may be an example of lingering high troponin-T from the first dose (some sources cite anything above 4 pg/mL as being above-normal, which would throw in subjects 3 and 69). However, accuracy thresholds for high sensitivity assays cut off at these lower levels, as will be discussed below.
Russian Roulette: Support for tissue-uptake-dependent toxicity
This section has been edited in light of raw data provided to Jonathan Engler by the study's corresponding author. The original text is in the footnotes.10
Were the identified subclinical cases true outliers, or merely the tip of an iceberg of elevated troponin-T reflecting damaged heart muscle cells? Although Elecsys results below 13 ng/L are considered normal, they might still describe damage. The threshold is more useful for ruling out myocarditis in the context of acute cardiac symptoms than in the context of long-term impacts on health. And while the threshold also describes the limit of the assay’s accuracy for individual results — values lower than 13 may be the product of “noise” — a pattern of post-2nd-dose elevation across the entire group of injected teens would correct for this limit.
However, no such overall rise is apparent in the raw data. Values appear to merely drift around, consistent with the lower accuracy of the assay below 13.
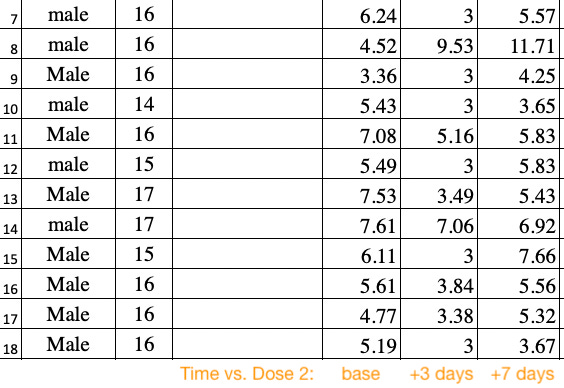
More revealingly, the most “high baseline” subjects often go on to score lower values after the second dose.

Again, “baseline” draws are already after the 1st dose — they may or may not reflect the impact of dose 1, but since there is no true baseline draw (before dose 1), this is impossible to determine for sure.
Rapid reductions, as seen for subjects 278 - 281, would seem to suggest that the high baseline values were either noise in the assay or the result of a more recent insult than the first dose, such as exertion (followed perhaps by inactivity, i.e. rest, induced by non-cardiac reactions to the second dose, including fatigue). Once again, this is impossible to determine for sure.
What is most significant is that:
Injection-induced troponin-T elevation / myocarditis is a true “Russian Roulette” effect.
Teens not highlighted in the main study results don’t seem to be showing any “sub-subclinical” elevations in troponin-T after Dose 2.
“Prior sensitization” appears not determinative. If any teens have lingering myocardial damage from Dose 1, this does not guarantee an increase in markers after Dose 2. There is yet a random element in play.
Thus, auto-immune sensitization does not appear to be the etiology for myocarditis, as there is no clear “prime - dose” response.
Thus, myocarditis is likely the result of transfection (uptake of Covid vaccine Lipid Nanoparticles) of heart muscle cells (cardiomyocytes) or of local endothelium. Uptake of LNPs is followed by direct or indirect (immune-mediated) toxicity from spike protein; i.e. disruption of vascular integrity or immune reaction against displayed spike protein, either of which results in inflammation and immune cell infiltration of the myocardium.
This is still consistent with a sex / age disparity in myocarditis for teen boys, per a simplistic “they have more heart cells per overall cells” theory as I have offered previously.11 If teen boys “buy more tickets” in the lottery of LNP-uptake in the heart, they will “win” more often.
Random transfection of cardiomyocytes might be the result of inadvertent intravenous injection, random LNP escape from the injection site after intramuscular injection, or both (I favor “both,” in light of the famous “Japan biodistribution” results12).
18% Abnormal ECG?
Edit note for this section in the footnotes.13
The “Russian Roulette” pattern for troponin-T stands in contrast to the ECG results, which appear far more widespread.
After vaccination, ECG revealed that of the 301 patients, 247 (82.06%) had normal sinus rhythm, while an abnormal ECG finding was noted in 54 patients (17.94%)

While the text of the preprint is unclear on this point, Høeg (of the earlier controversial myocarditis study) reports that the authors describe a baseline rate of <1% for abnormalities before the injections, apparently ruling out that these results are driven by any weirdness in the setting. In a tweet highlighted by Stephanie Brail’s review of the Thailand study:

So it would seem that these cardiac abnormalities are induced by BNT162b2, but I hesitated at first to rule out that this is not via some more indirect and innocuous etiology. For example, fever (recorded for 50 patients) leading to disruption of the autonomic nervous system (though here Brail makes a convincing counter-argument in her post).
After further review, I would call the ECG results a separate warning sign for abnormal cardiac disruption, even if it is still indirect. It may, for example, be a traumatic response to vascular-endothelial or coagulation harms — a signal that the engine is suffering due to problems with the fuel system, in other words.
This both supplements the alarming findings regarding troponin-T and may supersede them — suggesting, for example, that either LNP escape from the injection site is widespread or not required for post-Covid-vaccine cardiac trauma.
But, again, I don’t wish to rule out a more innocuous explanation completely.
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


(Cover image: Flag of Bangkok (study location). Public domain.)
Prasad, Vinay. “What does the Thailand Myocarditis Study Teach Us?” (2022, August 13.) Vinay Prasad's Observations and Thoughts.
Kirsch, Steve. “Thailand study of young adults post jab showed nearly 30% with cardiovascular injuries.” (2022, August 16.) Steve Kirsch's newsletter.
Kirsch uses a reference in the abstract to “cardiovascular effects” being found in 29.24% of patients to support his headline. As noted in my analysis of the EGC-abnormalities section, most of these “effects” might not reflect injury, though the raw data would help make that clear.
Mansanguan, S. et al. “Cardiovascular Effects of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents.” Trop Med Infect Dis. 2022 Aug 19;7(8):196.
See “Myo-Card Me a River.”
As in, not being examined in the context of known cardiac issues, and those with such issues being excluded. Pre-existing conditions are listed in table 1.

While “Patients who had a history of cardiomyopathy, tuberculous pericarditis or constrictive pericarditis and severe allergic reaction to the COVID-19 vaccine were excluded from the study,” no value is given for how many (if any) met that criteria and were excluded.
Daněk, J. et al. “Troponin levels in patients with stable CAD.” Cor et Vasa. Volume 59, Issue 3, June 2017, Pages e229-e234
https://www.medicalnewstoday.com/articles/325415#normal-troponin-range
A further reference point is Høeg, TB. et al.’s review, which found sub-14 medians in reported post-vaccine myocarditis (Fig. 3).
Original text for this section:
Notably, the sub-14 troponin-T values for subjects 4 and 7, on day 3 (visit 2), are still above baseline. It would be irrational for an observer to not consider those results to be associated with and still reflect the release of troponin induced by the 2nd dose.
The numbers on Day 3 may not reach the chosen threshold, but they still reflect damage and destruction of heart cells.
Likewise, all sub-threshold elevations in the remaining 294 teens in this study, were these values presented (they aren’t), could appropriately be interpreted in the context of them having just received the same poison. While “14” serves as a proxy for the accuracy of the test (Roche pegs the “CV” for their assay at 13pg/mL; implying that results below that value are more likely to include noise), it doesn’t define how many killed cells in a teen’s heart it takes to induce the short- or medium-term risk of a cardiac event, or to shave years off their eventual lifespan.
Moreover, a general rise in troponin-T (if it were included in the presented data, which it isn’t) in a large sample would by definition indicate the effect of the 2nd dose beyond the noise of the assay at sub-14 values.
The following example recycles the baseline values from Table 3. This allows for the semi-arbitrary designation of a new “above-normal” threshold (in these teen boys, in this assay) of 8. The rate of induced-high-ness is simply the number of 8-or-highers after minus the number before:

A similar evaluation of the raw data for the Thailand study should make it possible to judge the true rate of subclinical (and clinical) myocarditis - and it may be well over the 2.5% value derived here, for both male and female teens. (Additionally, if any subjects were excluded because of cardiac issues arising after the first dose, or if any were lost to follow-up due to issues after the second, these should also be factored in.)
See “Ocarditis!”
See Modern Discontent, “More on BioNTech's Lipid Nanoparticle Data.” (2022, March 6.) Modern Discontent.
Thanks to Stephanie Brail’s remarks in her review of the study at Wholistic, I have revised my report to be less skeptical of the ECG results. The original text is preserved below:
Otherwise, it is difficult to put too much stock into the ECG results. They seem alarming, but may not reflect the effect of the BNT162b2 injection as opposed to background noise or something about the setting of the tests:
After vaccination, ECG revealed that of the 301 patients, 247 (82.06%) had normal sinus rhythm, while an abnormal ECG finding was noted in 54 patients (17.94%)
Even if these cardiac abnormalities are induced by BNT162b2, it could be via some more indirect and innocuous etiology. For example, fever (recorded for 50 patients) leading to disruption of the autonomic nervous system. Again, if this could be shown to match the “true” sex-dependent myocarditis rate in the raw data, it would have more weight as an indicator of cardiac harms over just “nerves.”
For now, the 2.5% rate for boys exceeding the troponin threshold is horrifying enough.
They knew about the risk of myocarditis in young males before they issued the EUA for 12-17 and before they finished clinical trials 5-11 or started them for 6 month-4 yrs.
Yet FDA did not require them to test trial participants for Troponin levels (trial sizes were very small). It may have been too late for 12-17 primary series trial but not the booster trial.
Why is this? Because they no doubt knew what the results would be. Justice will not be served unless these people are prosecuted
Billions of shots given, but they could only produce one reasonably good study on myocarditis now- 1.75 years later.... and worse, myocarditis was pretty obviously a concern very early on. This study could also be improved if they did not only before and after the first dose, but also 14 and 28 days post 2nd dose.