
Reversal
The Covid vaccines universally flunk a major UK myocarditis analysis for males 13-39.


An analysis of myocarditis-related codes for hospitalizations and deaths in the UK finds that the Moderna, Pfizer, and AstraZeneca Covid vaccines, by their respective second doses, all create a greater 28-day risk-increase than infection in males aged 13 to 39.1 Could it have come out any worse?

As seen in the upper left, males 13 to 39 (12 and under are excluded from the analysis) are more likely to experience myocarditis from the shots than from infection. Zooming in:

For this group, Covid-vaccination thus apparently increases the chance of myocarditis even if it prevents 100% of infections (which, of course, it does not), and if 100% of recipients would otherwise have been infected (a benchmark which, if it ever arrives, appears to still be several years away) - and effects are clearly compounded by multiple doses.
The results, posted online on Christmas day, are bad enough to have prompted the normally equivocal Vinay Prasad to come out swinging. From his most recent Substack post (emphasis added):
But regardless, these findings already clearly dispel the true misinformation online: Yes, sorry to break it to you, vaccines can have risks of myocarditis EXCEEDING risks of myocarditis from infection. Pls stop saying otherwise. […]
If it is revealed that [Covid vaccination of males 16-40] is not in their best interest, this administration will have dropped a nuclear bomb on vaccine confidence for 20 years. God help us all.2

Significantly, this is a loss on the home field. The study is an outgrowth of the University of Oxford-sponsored protocol earlier used to “determine” that the AstraZeneca vaccine increased risk of clotting less than infection with SARS-CoV-2.3 The myriad organizations and panels listed in the authors’ conflict of interest statements probably receive pro-vaccine funding. It is unlikely that these results will be dismissed as the work of researchers with an “axe to grind” who should “know better.”4 The only positive spin on the paper possible is to quote the “all recipients” results, though even these flunked the Moderna 2nd dose.5
As Prasad’s (relatively) outspoken review augers, the paper may in fact be the straw that breaks the Covid vaccines’ backs, in the realm of expert groupthink. Even the authors themselves seem intent on raising the alarm:
Furthermore, given the consistent observation that the risk of myocarditis is higher following the second dose of vaccine compared to the first dose, there is an urgent need to evaluate the risk associated with a third dose as booster programmes are accelerated internationally to combat the omicron variant.6
Nonetheless, I would note some limits to the findings. While the authors have access to a robust set of UK patient data, hospitalizations and deaths and the medical codes which accompany them are not a controlled setting. Reality may not correspond to data point; and the overall number of events being measured (2,539 myocarditis-coded entries, 552 of which were time-associated with a dose of a Covid vaccine) is low.
Further, the study used people registered as Covid-vaccinated or test-confirmed infected (or both) as their own “controls,” comparing rates of myocarditis in the 28 days after a given dose or infection with the rates before (or after?), for all individuals in that event category (or, all individuals in that category of the same sex or over/under 40 age group).
But since publicity of the myocarditis risk coincided with the uptake of the Covid vaccines among the young, younger Brits with prior myocarditis were, presumably, less likely to get the shots. Hence why the authors’ analysis finds that being “about to” get Covid-vaccinated “reduces” the chance of having myocarditis. For this very reason, the authors censored the 28 days preceding any dose from their calculation of the baseline event rate. This may not have been enough of a correction - it is likely that the decision to get a vaccine at all “reduces” the chance of having had myocarditis.7 Naturally, since infection is not a choice, this same selection bias advantage does not exist on the virus’s side (though, the confounders go on to strike in both directions from there8).
On the other hand, and as Prasad points out, infections are likely under-counted, and any evaluation of the myocarditis risk after infection therefor excludes 100% of the “not myocarditis getting” of everyone who isn’t a recorded infection.9 There is not actually any way for the analysis used by the authors to adjust for this, since unrecorded infections are also undated (thus, the beginning of the 28 day risk window after these infections is unknowable). Additionally, as he points out, an analysis that segmented recipients into more granular age groups would likely find even uglier trade-offs than the “Under 40” headline values (it seems the authors should have been able to provide these values, but they did not).
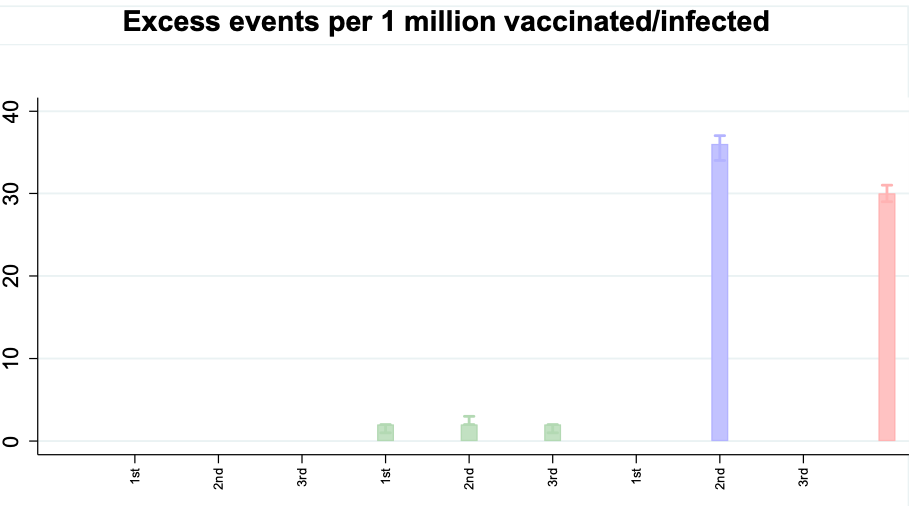
To this, I would add: The use of a “self-control” design may have distorted “baseline” and after-infection myocarditis rates for the over 40 groups, who received vaccines earlier. For many individuals in these groups, all events may in fact have been “post-vaccine.” It is difficult to decipher the study design on this point. Further, all risk-values and “extra events per million” for the 2nd and 3rd doses should be presented with the prior dose events included. And for the headline graphic above, extra events rates are left out for risk increases that did not meet meaningless standards for statistical significance, including for women under 40, even though these standards are met in the week-after-dosage results.10
Even with these limits and exclusions, the extra events results are grim. From the supplementary appendix:

Perhaps the most notable finding is how wildly the Covid vaccines skew the age-distribution of myocarditis events to the young compared to infection. However, this comes with caveats: The distribution is affected by different rates of uptake of the different brands, particularly for Moderna which did not deploy in the UK until April. The results for Pfizer 1st and 2nd doses are possibly the most representative of equal distribution between under and over 40 year-olds. And for total event counts, bear in mind that the Covid vaccines represent more stones thrown at more bushes than do positive tests:

Related: OCARDITIS! (Expert cherry-picking of favorable myocarditis signals; possible under-diagnosis of Covid vaccine-induced myocarditis in women)

Patone, M. et al. “Risk of myocarditis following sequential COVID-19 vaccinations by age and sex.”
Prasad, Vinay. “UK Now Reports Myocarditis stratified by Age & Sex After Vaccine Or Sars-cov-2.” (2021, December 26.)
As followed the analysis by Høeg, T. et al. which reached similar conclusions, but used VAERS data. See “Myo-Card Me a River.”
For all recipients:
(Patone, M. et al.)
In other words, the values for “expected cases of myocarditis in a 28 day window” would be lower than it should, because prior rates of myocarditis hospitalizations of the observed Covid vaccine recipients are the “control” used to define that rate. (Obviously, prior deaths are excluded from the baseline rate by default, but this discount equally applies to infection).
Some infections were among the previously Covid-vaccinated. Some were from early 2020, when only severe cases would be recorded as a positive due to low availability tests.
The authors exclude same-day “cases” and myocarditis events from their main analysis, as these may reflect myocarditis inpatients coincidentally screened for infection.
Weekly results are provided in the supplementary appendix:

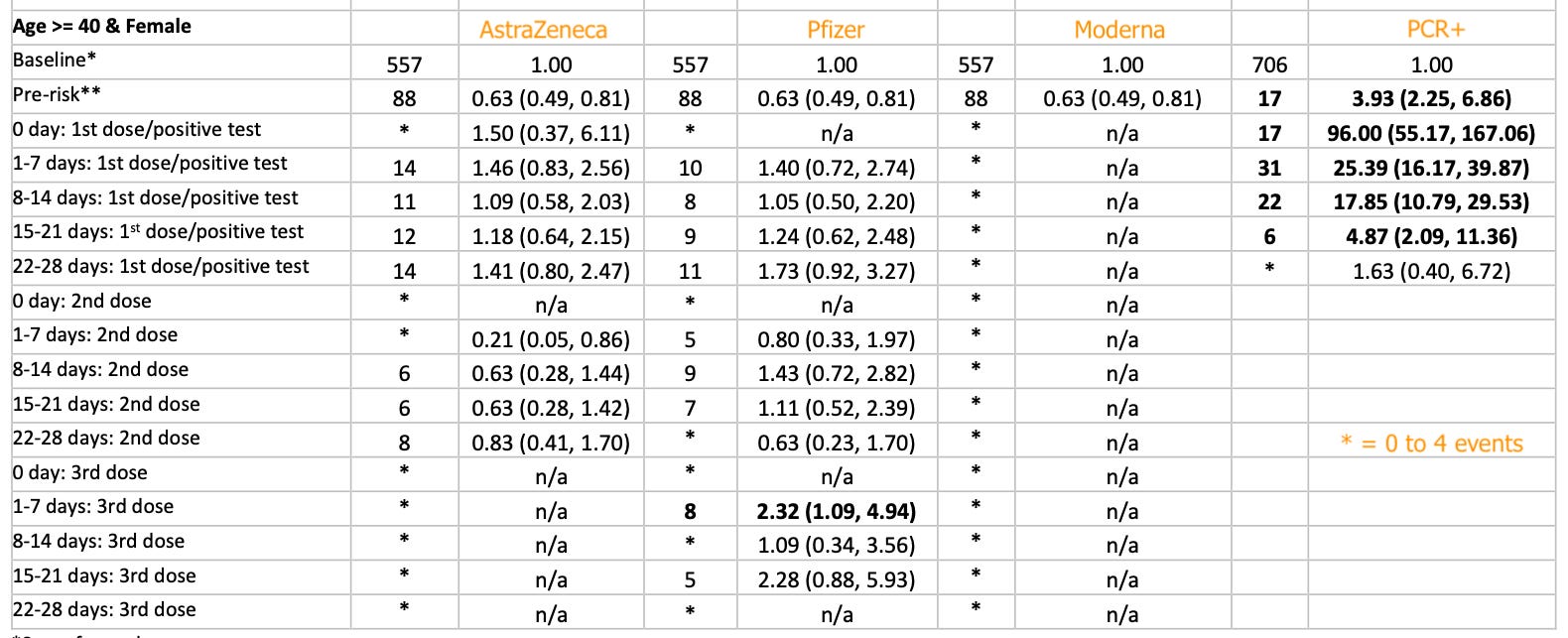
Back to 28-day relative risk results in the main paper, these are displayed on a separate set of graphs, with the corresponding values listed in Table 1:

Gotta get everyone waxxed so you eliminate the control group.
Could it be that myocarditis is pronounced in the vaccinated 13-39 group because it’s that group who are running around and pushing themselves physically. Someone who is vaccinated and 45 might be equally susceptible it’s just that middle aged men don’t run up and down football fields. But if they did…
I mean to imply that it’s possibly vaccination plus exertion that’s the factor and not vaccination plus age.