


RE IgG4 and cancer, autoimmunity
A brief look at the sobering musings of Uversky, et al. regarding mRNA Covid vaccine-induced IgG4

Summary (click to expand):
A look at a new paper proposing risks from Covid-vaccine induced IgG4 antibodies against the spike protein. As always, see “Tolerance Cometh” for an introduction into the problem:

The TL;DR recap of the problem
Is that the immune system operates like a “ratchet” under repeated antigen exposure, going only in one direction, with the final (irreversible) position on the ratchet being tolerance, the suppression of immune response. “IgG4” reflects that Memory B Cells in the mRNA-vaccinated have been shown in multiple studies to reach the end of the ratchet mere months after the second dose, and continue converting to tolerance-promoting and cellular immunity-suppressing IgG4 with further spike exposures (3rd doses, or breakthrough infections). Omicron infections do not offer relief from this problem, as anti-spike Memory B Cells can remodel their receptors and antibodies for Omicron, but will still derive from the original vaccine-induced pool of clones. Anti-spike IgG4 attached to infected cells will, in theory, fail to activate the immune system’s arsenal of cell-destroying tools; barring help from other antibodies (e.g. against non-spike proteins), the virus will replicate freely in those cells.

The great coin-toss: No one knows yet if IgG4 is going to harm
Let’s start with context. Or, skip this section to get straight to the main courses: Cancer risk; Enhanced infection; Autoimmunity. But if skipping, remember not to comment “as far as I can see, this IgG4 problem is overblown” afterward, since the question of putting the problem into perspective is addressed here.
In my treatise on IgG4 and future infection risks in February, I featured a freshly-published paper by venerated immunology professor Shiv Pillai which posed the IgG4 problem in fundamentally ambiguous terms: Is anti-spike IgG4 from Covid vaccines “bad,” or “good”?

Well, which is it? Pillai, despite decades of expertise, doesn’t know.
No one does: It is a perfect “known unknown.” As such, the going odds for “bad,” at this point, are basically 50/50. A coin-toss.
On which, on the longest time-frames, rides the survival and health of hundreds of millions of children and young adults who have been enlisted in the grand experiment with no possibility of an “undo” — anti-spike IgG4 antibody making-B-Cells are not going away.1
This is important context for interpreting the more sobering paper recently posted online by Uversky, et al., and highlighted and reviewed yesterday by Jessica Rose. The paper is here:

Rose’s review is here:

Both the paper and Rose’s review are excellent reads. However, it should be understood that there is no fundamental difference between Pillai’s sanguine assessment of the risks, and Uversky, et al.’s catalog of catastrophes, only a distinction of framing. IgG4 could be bad; we don’t know. But (which Pillai fails to acknowledge), that is tantamount to saying we don’t know if hundreds of millions of humans have been condemned to cancer, autoimmunity, future chronic infections or severe organ damage from the virus.
That, itself, is a very “bad” problem — an unfortunate and also totally unforeseeable consequence of the fact that there was no way to avoid subjecting a fraction of the entire human species to an unproven, rush-developed genetic therapy with intentionally high dosages and multiples of doses, because maybe it would make an extremely marginal mortality risk2 become lower (sarcasm).
With that introduction out of the way, I would mostly like to highlight portions of Uversky, et al. that I found the most thought-provoking. However, I will start with an overview of the comments on cancer, even though I cannot improve on Rose’s review in that respect. Then I will move on to the topics of chronic infection and disease enhancement, and finally autoimmunity.
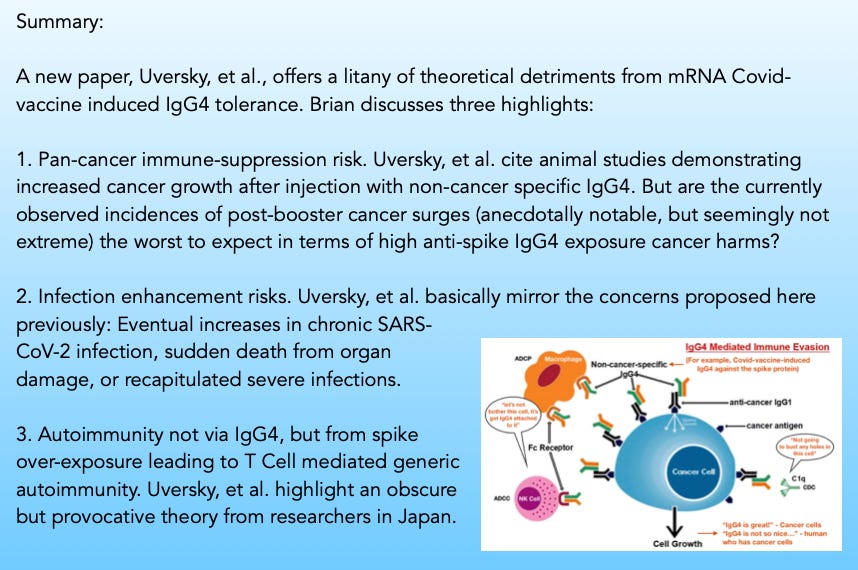
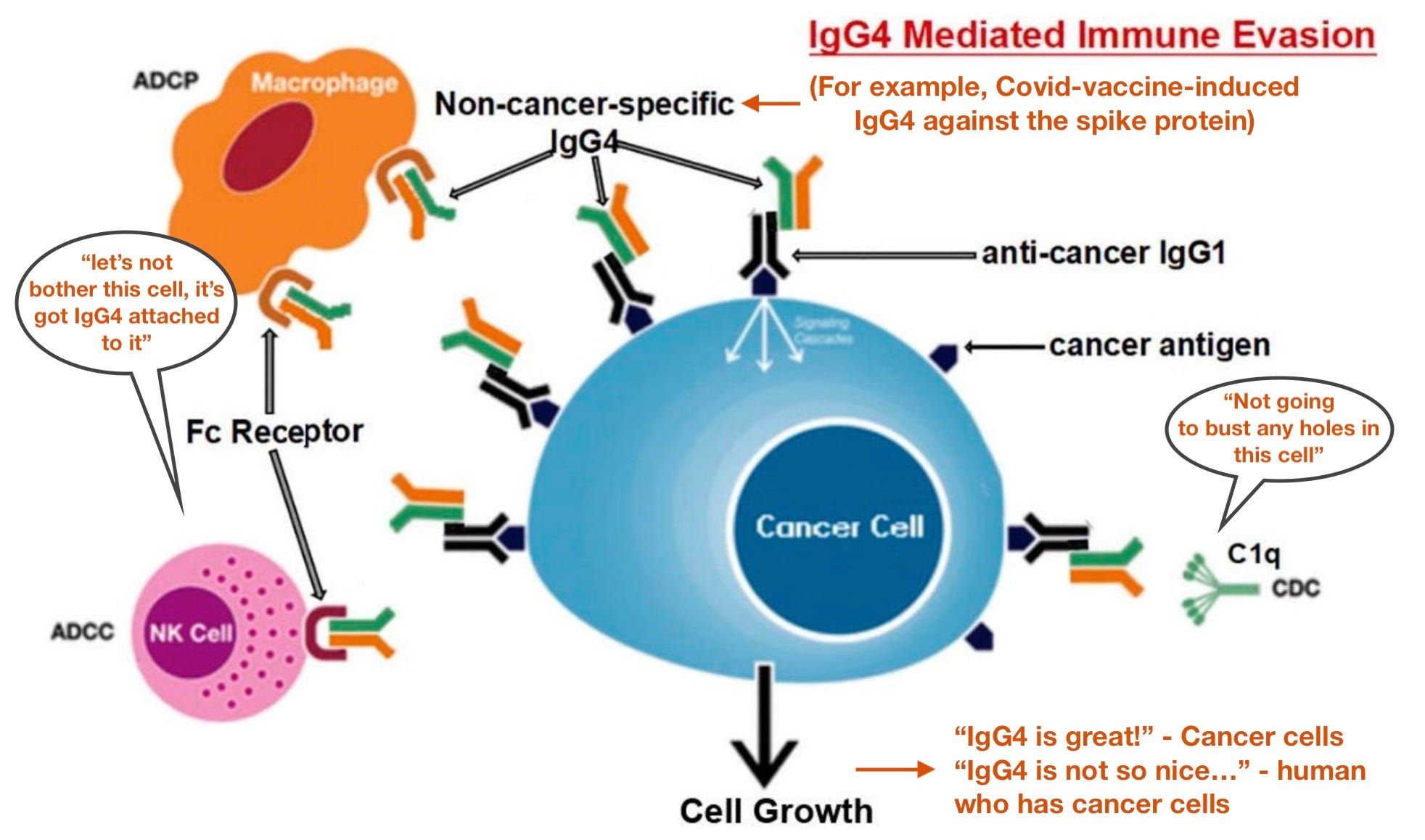
i. The IgG4 and cancer comments: Emphasizing the pan-cancer risk of IgG4
In my review of Irrgang, et al. last July, I proposed that anti-spike IgG4 could shield mRNA vaccine-transfected cells from immune clearance, just as tumors evade destruction thanks to IgG4 conversion — which would be a problem if these transfected cells decide to become cancerous.3
Uversky, et al. make a persuasive case that IgG4 could suppress anti-cancer immunity “across the board” — mRNA-induced anti-spike IgG4 could suppress resistance to existing tumors of any type, anywhere:
Locally elevated levels of IgG4 in cancer tissue hindered antibody-mediated anticancer responses, assisted cancer in blocking the local immune response and indirectly aided in cancer progression. Three separate immune-potent mice models supported this theory. It was discovered that local administration of IgG4 dramatically sped up the growth of implanted colorectal and breast tumors as well as skin papillomas caused by carcinogens. Researchers also examined the IgG4 antibody Nivolumab, which is used in cancer im- munotherapy, and discovered that it dramatically accelerated the development of cancer in mice when compared to phosphate buffer saline (PBS) and IgG1-treated groups [101].
One model involved injecting non-cancer-specific IgG4 into the subcutaneous inoculation site for breast cancer cells. In comparison to other groups of mice (injected with PBS or IgG1 without IgG4), this group’s cancer cell proliferation was dramatically accelerated, generating a significantly larger cancer mass by 21 days.
Perspective:
IgG4 is the rarest of IgG antibodies, and it is abnormal to have IgG4 for a viral antigen. This does not mean that anti-spike IgG4 antibodies from mRNA Covid vaccines will so substantially increase the overall level of IgG4 to introduce a “shotgun” pro-cancer effect as observed in the described mouse models. However, since the mRNA platform appears to promote vaccine-induced IgG4 due to the designed excess of both antigen (mRNA-transcribed spike) and antibody concentrations to begin with, the risk here can’t be easily dismissed, either.
Presumably, risks would be highest when anti-spike antibodies surge, as after re-injection or infection (even if IgG4 conversion increases afterward, since overall anti-spike antibodies will still be fading again). This could account for anecdotally-reported surges in cancer remissions after boosters, for example; though, those anecdotes aren’t well-substantiated by any hard data. Still, it would seem to suggest that the “worst” of a generic pro-cancer effect from Covid vaccine-induced IgG4 has already been seen, and isn’t so bad.
Edit, May 31:
I had unfortunately forgotten that reader and researcher Jim H has previously highlighted the Fc-Fc interaction theory for IgG4 cancer risk, specifically in the context of post-booster cancer surge anecdotes. Please see his excellent article here:

In the comments of this post, Jim also points out that the threat of IgG4-promoted cancers is not limited to Covid vaccines, since mRNA is being expanded into flu (and other) vaccines at this very moment.
ii. Chronic infection, enhanced disease: Reflecting the Unglossed model
Uversky, et al. propose ramifications for future infection outcomes that essentially reflect the theories previously discussed in TASD:

The series concludes, in Pt. 3:
The likely implications of IgG4 tolerance in light of the reality of severe “Covid-19”: persistent infections, ADE [defined as recapitulation of severe disease, or organ destruction from uncontrolled viral replication, leading to sudden death]?
Uversky, et al. offer three precedents (inter alia) to support the same conclusions in TASD, e.g. an eventual heightened risk of severe and chronic SARS-CoV-2 infections in young vaccinees:
Recombinant SARS-CoV-2 vaccine precedent
The conventional SARS-CoV-2 vaccine’s ability to provide immunological protection may be significantly impacted by over-vaccination [here referring to the study from China which did not involve mRNA vaccination, but demonstrated immune exhaustion with multiple doses of spike antigen,4 which is still an important model in understanding the implications for mRNA-induced antigen overload]. If this happens, either newly diagnosed COVID-19 cases or people who have already contracted the virus again may have a more severe case of the illness. […]
HIV vaccine precedent
[Results from HIV-vaccine trials with multiple doses support] the notion that an increase in IgG4 subclasses could lead to extended viral persistence in case of infection, considering that Fc-mediated effector action is essential for viral elimination […]
Malaria precedent
It is important to note that the probability of contracting malaria increased by around three times when non-neutralizing IgG4 levels doubled. Up to the age of 24 months, IgG1 and IgG3 demonstrated 51% and 56% protective effects, respectively; however, IgG4 was linked to a higher risk of malaria infection throughout this age range [115]. It is interesting to note that a separate study also found a link between high IgG4 levels and a higher risk of infection and malaria exacerbations […] Moreover, IgG4 has been demonstrated to prevent the opsonization of infected erythrocytes by IgG1 and IgG3 in vitro
They recap in the Discussion:
However, a very different situation occurs when a virus invades our body. In this scenario, vaccine-induced tolerance can potentially have several negative, unintended consequences because tolerance to the spike protein could inhibit the immune system from detecting and attacking the pathogen (Figure 4); thus, potentially exacerbating SARS-CoV2 pathology in susceptible individuals who suffer re-infection of COVID-19 in the setting of vaccine-induced immune suppression. […]
In this situation, we suggest that even these less pathogenic Omicron subvariants could cause significant harm and even death in individuals with comorbidities and immuno-compromised conditions. […]
A tolerant immune system might allow SARS-CoV-2 persistence in the host and promote the establishment of a chronic infection, similar to that generated by the hepatitis B virus (HBV), the human immune deficiency virus (HIV), and the hepatitis C virus (HCV)
(They also propose generic suppression of innate anti-microbial and anti-cancer immune response, but this is not related to antigen-overload or IgG4, and not portrayed as an mRNA-vaccine exclusive mechanism).
Perspective:
Uversky, et al. are not compelling that real-world evidence supports the theory of enhanced disease already occurring. It should be recalled that redundancy is the overarching design philosophy of the immune system; for example, if SARS-CoV-2 infected cells are producing other types of viral proteins, then non-spike antibodies (generated from previous infection) may be sufficient to rescue the immune system’s cell-killing response.
It is still useful to revisit Irrgang, et al.’s finding that triple-Covid-vaccinated blood suppresses in vitro monocyte and complement-mediated cell-killing, vs. the post-second dose response. Rescue from antibodies for other viral proteins may be a question of balancing this suppression.

iii. Autoimmunity - IgG4 just a “symptom” of pathological overstimulation, and are Covid vaccines the tip of the iceberg?
I have previously resisted speculating that IgG4 can be presumed harmful simply because of the association of overall IgG4 levels to autoimmune and inflammatory diseases, or worse infection outcomes with SARS-CoV-2, since IgG4 may simply be a correlate for those diseases, rather than the cause, with T Cell responses driving both disease and IgG4 conversion.
Uversky, et al. offer evidence in support of the direct harm of IgG4 in animal models which perhaps argues for rethinking my prior stance. However, this is ultimately less provocative or compelling than their mention of a recent, but obscure theory of autoimmunity:
Repeated vaccination could also lead to auto-immunity: in 2009, the results of an important study went largely unnoticed. Researchers discovered that in mice that are otherwise not susceptible to spontaneous autoimmune disorders, repeated administration of the antigen promotes systemic autoimmunity. […]
According to the self-organized criticality theory, when the immune system of the host is continually overstimulated by antigen exposure at concentrations higher than the immune system’s self-organized criticality can tolerate, systemic autoimmunity inevitably occurs
There is no real way to review the theory in question without derailing this post. The 2009 study by Tsumiyama, Miyazaki, and Shiozawa purports to reliably induce T-Cell mediated autoimmunity (generation of myriad autoantibody producing B Cells as seen in Lupus) by injecting mice with high concentrations of common antigens multiple times:5 Given enough exposure to any given antigen, Lupus-like autoimmunity results from the splenic T Cell response. The authors repeat and refine on their results using flow cytometry a few years later, linking the pathological T Cell response to PD-16 — a marker of T Cell exhaustion and tolerance which was also elevated in the Chinese repeat-spike-vaccination study.7
Despite offering an earth-shattering proposal to reshape how autoimmunity is understood to arise, with obvious and extreme implications for all vaccines, the 2009 paper only has 16 citations in pubmed prior to the mention by Uversky, et al.
Perspective
The theory that antigen overexposure of any-type pushes PD-1+, CD4+ T Cells toward blanket autoimmunity has not been well-replicated, due to apparent lack of peer interest. It is nonetheless provocative, and may have some corroboration in veterinary vaccination (for example, ovine Autoimmune/inflammatory Syndrome Induced by Adjuvants8).
Regarding the Covid vaccines in humans, it would not seem to be a danger that has been replicated as reliably as in Tsumiyama et al.’s papers. Additionally, it is not clear if the amount of antigen overexposure from mRNA Covid vaccines (specific to one antigen) is substantially higher than antigen overexposure from all other vaccines on the childhood schedule taken together (specific to multiple antigens), in which case the rates of T-Cell mediated generic autoimmunity might be in line with recent trends that were already underway, and caused by other vaccines.
It is still a theory plausible enough to warrant caution against the reckless maximization of antigen and antibodies that has characterized Covid-19 vaccine strategy. As Uversky, et al. remark:
[Billeskov et al.] also encouraged experts in T-cell vaccination, in particular, to remember that sometimes, less certainly is more.
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


See “Tolerance Cometh.”
Tsumiyama, K. Miyazaki, Y. Shiozawa, S. (2009.) “Self-organized criticality theory of autoimmunity.” PLoS One. 2009 Dec 31;4(12):e8382.
Miyazaki, Y. Tsumiyama, K. Yamane, T. Ito, M. Shiozawa, S. (2013.) “Self-organized criticality theory and the expansion of PD-1-positive effector CD4 T cells: search for autoantibody-inducing CD4 T cells.” Front Immunol. 2013; 4: 87.
See footnote 4.
Asin, J. et al. (2018.) “From the bluetongue vaccination campaigns in sheep to overimmunization and ovine ASIA syndrome.” Immunol Res. 2018 Dec;66(6):777-782.
Well, I remain convinced that the cancer wards saw too many people who were in remission suddenly get cancer again. I didn’t get any jabs and when I had cancer last year (one with pretty bad stats) I made sure to tell the lead oncologist that I was unvaccinated. I wanted her to make the connection. I am currently still in remission but you can tell that they are rather shocked by that. I somehow got in my chart that “I found the jab to be a possible p53 suppressant and therefore was reluctant to take it “ :) I’m kind of geeky proud that I got that in my chart.
Totally anecdotal, but my best friend is German and literally every person she knows (except her), has had 4 or more jabs. They are literally besieged by constant illness to the point where it is completely alarming, but they remain oblivious to any connection. 3 older family members died, one had cancer spread like wildfire, the other an aneurysm, another a sudden heart attack. The others sick, I mean literally its to the point that you can only count the days they felt well, and that is like 20% of the days since the first of January. We both mentioned that we are the only 2 sheep in that field that think the man and the dog are working together....
I sort of felt like this review seemed redundant, but I think I just confused it for the review that was released a few months prior. I raised a point with respect to IgG4 an autoimmunity a while back as I just thought based on conjecture that seemed to have been a reactive, protective response from autoimmune responses. It's interesting that IgG4 doesn't appear to present in mice. I'm curious if this is an evolutionary consequence of longer life and a greater probability of being continuously exposed to an allergen/pathogen.
I think one point of contention I have with the IgG4 cancer argument is that if IgG4 is indiscriminate in the effector-ouroboros binding motif then shouldn't we expect higher incidences of cancer in relation to those with greater allergens? Or maybe that's something that hasn't been investigated due to lack of interest or lack of knowing.
The T-cell argument for autoimmunity seems interesting, although that seems like it would be easily answered by checking for cross-reactive responses. If the paratope of some antibodies diverts to target the host we shouldn't expect them to also cross-react, although that argument would have to be made in lieu of exposure to said cross-reactive antigen.