


Myocarditis And Bolus Theory
The whole spike in myocarditis-having-kids paper: "Bolus" vindicated? Brian speculates it is more to do with disparities in full-length RNA content.

Summary (click to expand):

Whole Spike After Vaccine-Induced Myocarditis
Readers are probably already familiar with the paper:1

It presents a bit of a puzzle. What is the experimental mRNA injection actually doing in the body this time? And this isn’t tiring at all. No, all these little mRNA experiment mysteries are an endless delight. Like a free New York Times Games™ account.
16 kids who showed up to Boston hospitals with post-vaccine myocarditis had blood samples taken. These were compared with age-matched or young adult controls sampled shortly after their second injection.2
The emphasis was on immune response. Given that “myocarditis” is an acute inflammatory condition, there were naturally some differences in circulating innate immune markers consistent with inflammatory activation.3
In spike antibody and T-Cell land few differences were found. Both myocarditis and control donors had spike and Receptor Binding Domain antibodies, and spike-recognizing T Cells. More generically, the myocarditis kids’ T Cells showed increased markers for exhaustion (but the n is too small here to rule out random chance):

So the innate immune response was reacting to the myocarditis, but the myocarditis didn’t seem to be a reaction to the memory immune response to the vaccine, since these were similar in subjects and controls. What about differences in vaccine by-product?
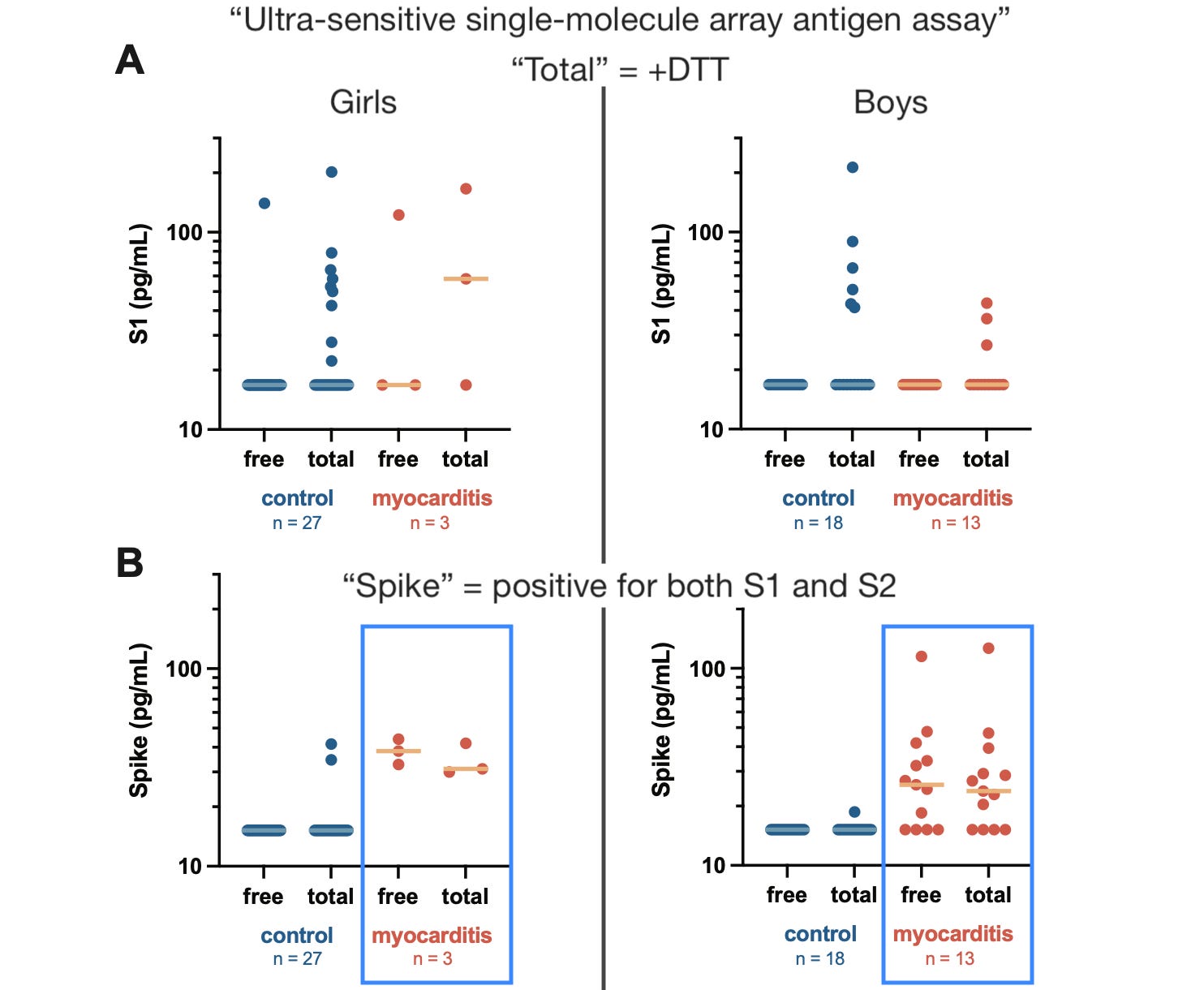
Here, even though both myocarditis and control kids had circulating “S1” — the head of the spike protein, which can detach and fly around the body despite fact-checks to the contrary — kids with circulating full spike protein were mostly limited to the myocarditis group:
There are three ways two interpret this:
The myocarditis kids simply manifest some mysterious “order of operations” problem where the immune response looks the same, but intervening steps exacerbated cell destruction (e.g., didn’t kill spike-producing cells quickly enough, or killed them too quickly, or whatever). This post will not comment on this theory as there is no way to evaluate it.
The myocarditis kids have more cellular destruction because more cells were transfected, hence more S2.
Or, there is no difference in how many cells were transfected, because S1 levels are not higher; therefore, if anything, the myocarditis kids have more full-length RNA (as opposed to truncated species).
Added as a result of reading over my own post after publishing: Circulating spike is simply a result of tissue-specific inflammatory cascades that result in more simultaneous cell-destruction and scuttling of spike. So now there’s two “hall-pass” theories that make “bolus” potentially irrelevant.
Interpretation 2: “Bolos”?
What’s puzzling about this result, to me, is not so much that the myocarditis kids have circulating whole spike — rather, that the controls (mostly) don’t.
For example, if heart cells have been transfected and are being destroyed by the immune system, then maybe spike protein (the S2 “stalk” of which would normally be anchored to the cell surface) is being released into the bloodstream as debris. The “problem” is, why wouldn’t this also be happening when other, less critical cells get destroyed? Wouldn’t any transfected cell eventually result in “scuttled” spike protein?
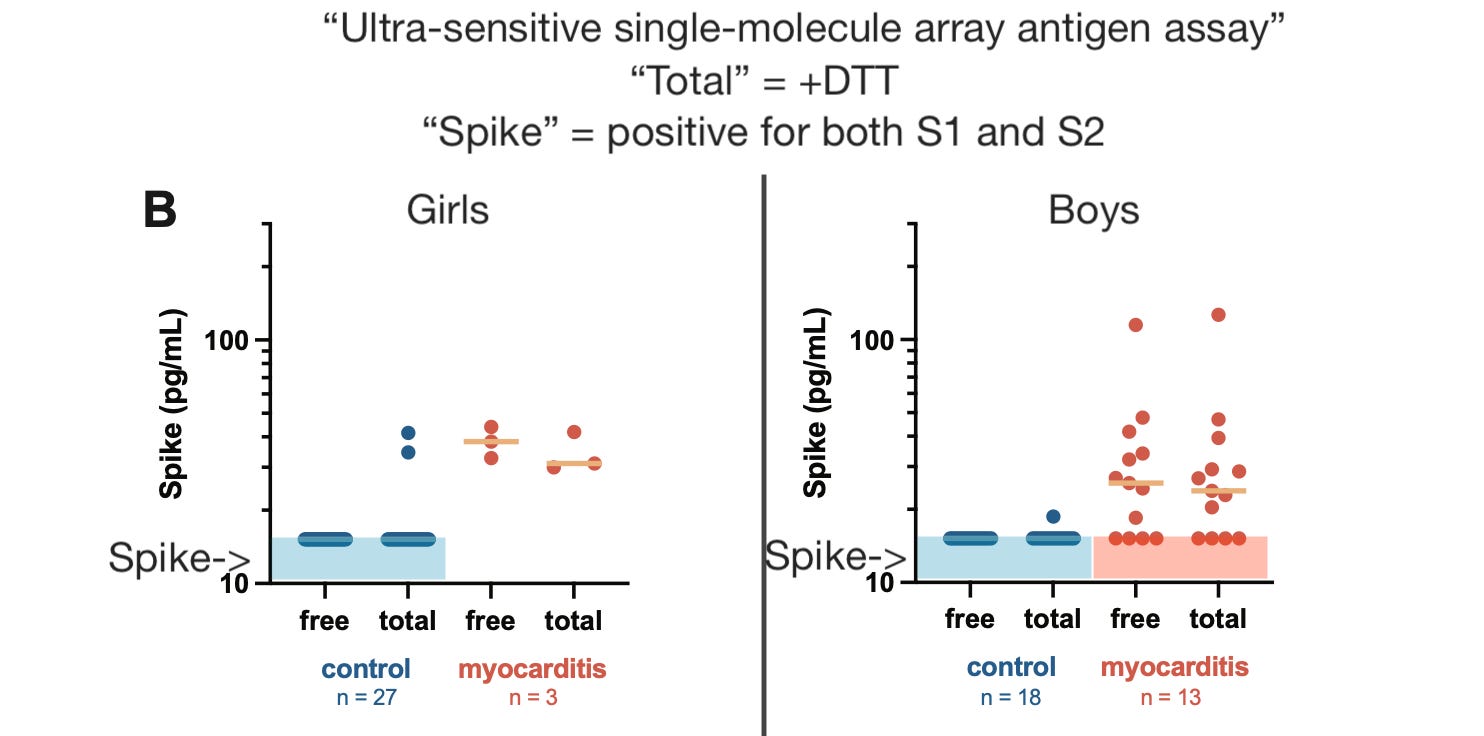
After a few weeks of mulling over the problem, I have decided the likely difference is that the controls are simply (mostly) below the limit of detection for S2. It’s in there, but it is below the cutoff. Like the gas still in the tank after the gauge bottoms out:
Support for this interpretation comes from a previous “what actually happens when this product is injected?” study, the famous “exosomes” paper. In this study — Bansal, et al. — 8 of 8 subjects were positive for the S2 subunit of spike at multiple time-points after the first and second doses.4 However, Bansal, et al. did not employ any cut-off as their isolation of spike involved Western blotting of filtered exosomes. At all events the peak of detected S2 was at the same time-point examined in Yonker, et al.'s control kids — after the second dose.
If everyone who gets mRNA-vaccinated makes exosomes with S2, these should be detected in the assay used by Yonker, et al. Besides using a different assay, however, Yonker, et al. differs by requiring co-detection of S1, and not reporting results under the limit of detection. With no access to raw values for their reader, we are just left with inference. There was likely “some” S2 detected in all subjects and controls. The myocarditis kids just had a lot more.
Thus:
Myocarditis correlates with RNA payload?
This interpretation would clearly seem to (partially) vindicate the predictions of Marc Girardot. There are major differences in payload of Covid vaccine product, and these differences largely account for the “horsies and unicorns” distribution of apparently unharmed and gravely harmed recipients. Here is a substack-cameo of his latest post, which also references Yonker, et al.:
I say partially vindicates, because, if the reader is not already aware, Girardot’s claims are more extreme than the characterization provided above; and, these results, even if accepted as a reflection of “bolos,” rebuke the extreme form of the claims. Specifically: Girardot dismisses inconsistency of manufacturing, packing, preservation, and administration of LNP product (I make baffled gestures even as I type this); Girardot renounces all claims of direct spike toxicity (more baffled gestures), and attributes side effects solely to immune-mediated cellular destruction of transfected cells.
Therefore, all that matters is inadvertent intravenous injection leading to widespread dispersion of spike. Needle hits blood vessel; Lipid Nanoparticles shoot through the body as opposed to politely staying in the injection site. He claims that all vaccines have always had this risk, and all vaccine AEs have always been explained by this risk; for example, smallpox vaccine; which isn’t even actually injected5; but anyway.
But, as said, Yonker, et al. refutes this extremist model.
“Bolos” extremism rejected:
Girls with high payloads can “tolerate” spike (high whole spike levels in 2 of 27 control dots). This isn’t surprising, given that sex-differences in susceptibility to myocarditis have long been evident to the naked eye, but sex should not make a difference to likelihood of intravenous injection. This might not be fatal to “bolos” since sex probably does affect dispersion (i.e., RNA doesn’t land in heart), but Yonker, et al.’s controls probably excluded adverse reactions of any type.
Boys without high payloads (3 of 136 below-Limit of Detection myocarditis dots) can still develop myocarditis.
No clear correlation between detected whole spike and Troponin-T values in Table 1S. This may simply reflect (unreported) age and sex confounders, however.
Therefore, “bolos” is not a binary determinate of vaccine harms. There’s “other stuff” going on.
More difficult from the standpoint of the “bolos” theory is the failure of detected S1 to reflect the same signal. S1 — which can only be detected once it is separated from antibodies, in this case via the addition of DTT — can circulate (in theory) simply as a result of cleavage of the spike protein, which allows the head subunit to fly off and go wherever it wants, “harmlessly” (per Girardot).
If the myocarditis kids received inadvertent intravenous injections, shouldn’t they have “more” circulating S1? The answer to this isn’t really clear. If the injection is staying in the shoulder, S1 might still disperse thanks to cleavage of expressed, anchored spike protein.
For that matter, why would intravenous injection lead to more cellular destruction and scuttling of S2 in the first place? Is it just something special about what happens when heart cells are destroyed?
Conclusion
Overall, I would say that Yonker, et al. does little to validate (or demystify) the (inadvertent-intravenous-injection-based) “bolos” theory.
Interpretation 3: High whole RNA payload?
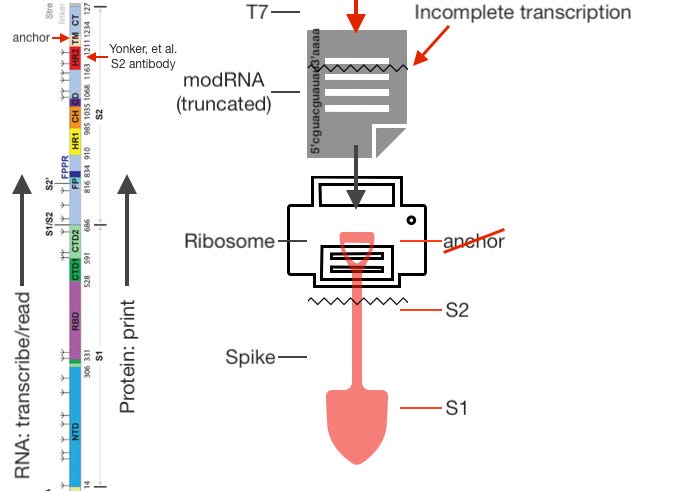
Our cells are full of protein-making 3D-printers called ribosomes. These read RNA molecule “files” from beginning (5’) to end (3’) and stitch together amino acids in the corresponding order coded by the file. For the mRNA-vaccine-encoded spike protein, this results in constructing the S1 head first, and the S2 stalk second. The transmembrane anchor, which keeps spike protein attached to the cell surface, is made next-to-last. It’s also just after the region targeted by Yonker, et al.’s S2 antibody for detection of “whole spike.”

If the T7 “RNA maker thing” at the Covid vaccine factory stops transcription early, the result is a “truncated” RNA that will not code for the whole protein in your transfected cell factories.
As discussed last week, these partial RNAs are likely a huuuge fraction (if not the majority) of molecules included in post-authorization vaccine. They were already up to 40% of the RNA content in the prototype versions subjected to “regulatory review;” and there’s little chance that quality did not degrade as production was scaled up for market. And, the effort done by Pfizer to show that these RNAs won’t get turned into proteins was perfunctory, if not completely fabricated. For more on the substantial differences between the ideal “LNP RNA package” and what was probably injected into people, see, once again, Maria Gutschi’s work.
Anyway, the theory is that partial RNAs won’t be turned into anything inside the body because they lack a 3’ “tail;” the reality is no one has a clue what really happens. It is nonetheless certain that your cells are not going to “improvise” a transmembrane anchor. If partial RNAs are turned into anything, they will lack this element:
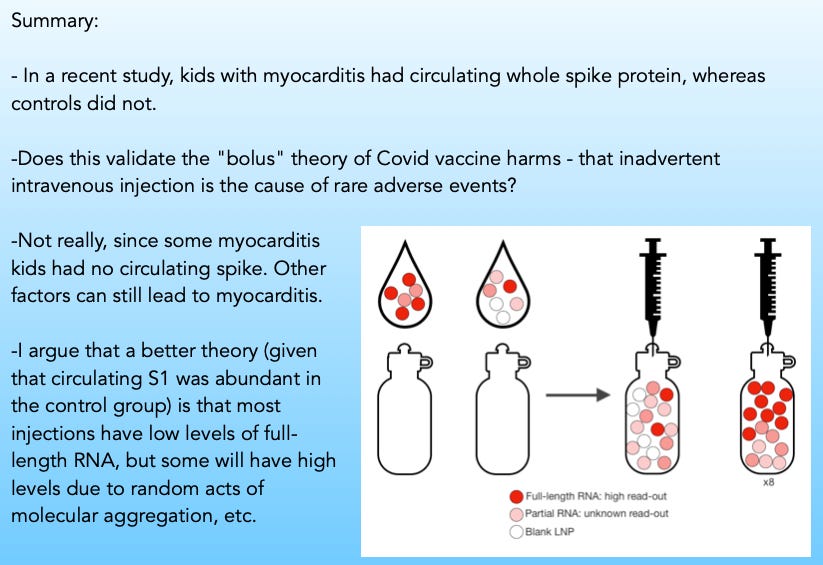
This variability, rather than intravenous injection (which no one really knows, for a fact, to make a difference in end-point dispersion of LNPs anyway7), or in combination with it, probably accounts for much of the biological variety in how Covid vaccines harm recipients.
Only some LNPs will contain full RNA molecules. Some will contain partial RNA molecules; some will likely be blank. LNPs may further associate or disperse into vials and within vials stochastically. The variability on how much full-length RNA can be injected goes well beyond the potential of getting a “5-pack” injection; it could easily span orders of magnitude (though my cartoon example only results in an 8-times dose).

If most people are injected with substantial or even predominant partial RNA payloads (bearing in mind that all 8 participants of Bansal, et al. were pumping out some S2-containing exosomes8), they will experience substantially less immune-mediated cellular destruction.
Partial RNAs may (per theory, should) be broken down near-instantaneously due to lack of 3’ tail, resulting in no or only transient and trace expression of S1 from most transfected cells. Short-term partial-spike-producing cells may still be at risk from destruction due to antigen presentation; but, again, this could be transient, leading to evasion of immune detection (especially after the first dose, when no spike-specific antibodies are available to tag transfected cells for several days).
Alternately, if partial RNAs are in fact durably translated contra the theory, there obviously might still be a lower or slower rate of immune detection (thanks to the lack of the S2 anchor). These cells would pump out un-anchored, free-floating S1. For this reason, circulating S1 levels may be similar among (normal) low full-RNA and (rare) high full-RNA recipients. However, again, this contradicts the theory and currently-published in vitro results.9 It doesn't seem like partial RNAs make S1.
Regardless, high-full-length-RNA recipients will express full-length spike from more cells, for longer. The hazard of immune-mediated cellular destruction will thus be much higher. Full-RNA transfected cells would deck themselves out with spike over some course of time before immune detection; said detection would result in the scuttling of all that full-length spike at once. If positive feedback loops result in nearby transfected cells being co-discovered (due to inflammatory cascades), then myocarditis would by definition be associated with simultaneous scuttling of spike (as opposed to dispersed full-length transfection, where transfected cells may be detected in staggered intervals and S2 would remain under the limit of detection due to breakdown and clearance).

Support from other papers?
Potentially consistent with this model of “RNA Russian Roulette” is Fertig, TE et al., which had extremely poor luck in getting Pfizer Covid vaccine to make blood cells express spike.10 In this, the authors administered BNT162b2 (supplied by the Romanian Ministry of Health) to three types of cells: Human granulocytic blasts, promyeloblasts, and freshly-donated peripheral blood mononuclear cells. The latter two seemed to take up LNPs just fine, but no cell types would make whole spike:
In our hands, despite very high vaccine concentrations (10 μg mRNA per 1 × 106 cells), morphological changes were subtle for all tested cell types.
However, of approximately 100 cells analysed, only three presented spikes, suggesting low levels of expression. Such spikes were absent in K562 cells at 3 and 24 h incubation and were also absent in PBS-treated controls. By contrast, spike-like structures were conspicuously absent on vaccine-treated HL-60 cells or at the cell surface of the lymphocytes, mononuclear phagocytes and platelets identified in the PBMCp fraction, regardless of incubation times.
Did transfected cells, instead, make partial spike? It doesn’t seem so. Western blots were unsuccessful at showing a difference vs. negative controls, suggesting (I would say) that the vaccine they received was a “dud:”
However, as with other in vitro results concerning the Covid vaccines, it could simply be that these types of cells were not an appropriate medium for the intended experiment.
Final thoughts:
Given the resounding lack of in vitro evidence for partial RNA / spike expression, it seems Interpretation 3 (differences in whole RNA content) is no better than Interpretation 2 (“bolos”) in explaining why controls were still highly positive for circulating S1.
But I still think there must be some level of partial RNA expression in vivo, and that this makes Interpretation 3 more resilient to the S1 problem. Additionally, I think it is less of a stretch at explaining why more controls do not have whole spike (i.e., whole spike should still be released in immune response to “shoulder spike;” thus, it makes more sense to propose different true payload of readable, full-length RNA rather than dispersion).
Additional measurements that were not reported in Yonker, et al. could help interpret the results.
Specifically, it’s absurd that raw values for detected S2 and S1 were not reported. The authors set their “limit of detection” for their assay at three standard deviations above the background signal (presumably because one of them is involved with development of the assay and would like to establish market standards). This reader thinks that was too high. There is no question that these subjects have Covid vaccine in them; so the idea that false positives would be a problem with a lower LOD isn’t logical.
Further, was there any “naked” S2 — S2 in absence of S1? The supplemental methods clearly specify that co-detection was required for reported “whole spike.” If naked S2 was equally detected in both myocarditis and control donors, that would refute the “Full-length RNA payload” theory. Too bad; Yonker, et al. don’t think we should know what they actually measured.
Related:

If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Yonker, LM. et al. “Circulating Spike Protein Detected in Post–COVID-19 mRNA Vaccine Myocarditis.” Circulation. 2023 Jan 4.
Different modules involved different subjects and controls. For example, for “humoral profiling,” the authors excluded subjects presenting more than 11 days after injection, so that immune responses would be sampled at consistent timings. However, the module measuring circulating spike involved all 16 subjects:

individuals with myocarditis displayed distinct cytokine profiles reminiscent of the profile seen in MIS-C, suggesting likely innate inflammatory activation, with significantly elevated levels of interleukin (IL)-8, IL-6, tumor necrosis factor-α, IL-10, interferon-γ, and IL-1β and lower IL-4 levels compared with healthy vaccinated control subjects
Bansal, S. et al. “Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer–BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines.” J Immunol. 2021 Nov 15;207(10):2405-2410.
Only three subjects are listed as “not detected” for whole spike in Table 1S. I believe this is because subject 10 is exactly above the cutoff, at 17.76.
Regarding the famous mice study, Joomi has made the case that the intramuscular injection also appears to have lead to heart inflammation:
Bansal, et al. lists Sino Biological antibody without a specific product code. Since they describe their blots as staining for S2, they may have used
https://www.sinobiological.com/antibodies/cov-spike-40590-d001
which does not specify a target.
Yonker, et al. used Invitrogen MA5-35946 S2 and specified the heptad repeat region as the target.
See “Pfizer Did Not Know What the Covid Vaccines Actually Do in the Body” which discusses Pfizer’s purported evaluation of the topic for regulators.
And Rotello, R. et al. “In vitro Characterization of SARS-CoV-2 Protein Translated from the Moderna mRNA-1273 Vaccine.” (pdf) Scientific Journal of Biology & Life Sciences. Volume 2-Issue 4.
In this, substantial below-full-weight spike protein is detected from transfected NIH 3T3 cells as “smears” at time-points 24 hours and later; however, the clean lines at 6 hours suggest that these later proteins are products of protease degradation of full spike over time, rather than of expressed truncated RNAs. On the other hand, it is unknown if “partial spikes” would be detected by anti-spike antibodies to begin with, given that structure could be substantially affected, masking epitopes (hence why Pfizer also used a cell-free system with labeled lysine). But this wouldn’t relate to the question of whether detected circulating S1 was the product of partial RNAs or not.
Fertig, TE. et al. “Vaccine mRNA Can Be Detected in Blood at 15 Days Post-Vaccination.” Biomedicines. 2022 Jul; 10(7): 1538.
You had me at "stochastically"....
I second Richard Sharpe's comment that your diagrams in this case were really excellent and helped make it all more understandable. Thank you also for at least considering Marc G. for a trophy, even if his theory is only, maybe, partially explanatory.
It's a treat to see you working your way through the various hypotheses - this is how science is done! Even those readers who don't fully understand what is being described should be able to realize, by seeing how unsettled the science is, that everyone involved in every aspect of the mRNA transfection drive was way, way over their skis as they jumped off the ramp at Mt. Hubris.
Being somewhat (science) illiterate myself. I always read the comments to "tell me" what you said. It's early yet I will check back tomorrow.