
Means, etc.
Revisiting / refining my wild accusations of a "late summer hospital killing spree."

The American Northeast did not partake in the late-summer rise in excess mortality. Is that because there weren’t any unvaccinated infected in that region for hospitals to kill?1

After my first two posts on the controversy of “what drove excess mortality in 2021?”2 I noticed a stark disparity in the US regional trends which supports my theory of the case. However, I didn’t publish any updates discussing said disparity.
The reason for this, is that I am pretty sure my entire “map of reality” as pertains to this topic essentially hails out of Bizarro World for most readers. But as the controversy is back in the spotlight, I would like to share my observations. And I now realize that the easiest way to communicate these observations is to lean into the “alt-reality” theme.
And so:
Bizarro World Travel Guide!
In Bizarro World, severe efficacy is real. This solves the alleged “puzzle” (over in regular Earth) of why there is evidence supporting that severe efficacy is real - i.e., why after all the other claims made about the Covid vaccines turned into dust, severe efficacy was still standing. Is it partially some sort of bias in the data, as well as some manipulation of official stats? Probably, and more-so in some regions than others. Is it entirely bias? No. In Bizarro World, circulating antibodies improve infection outcomes. That’s why the body makes them. Weird but true (in Bizarro World).
In Bizarro World, Delta was at least equally, in not more virulent than the 2020 strains. This solves the alleged “puzzle” over why only contrived and explicitly manipulated interpretations of the data can support the otherwise explicitly baseless assumption that it wasn’t. The virus doesn’t care that “Immunology 101” thinks it should have self-attenuated overnight. Nature is more complicated than Immunology 101, in Bizarro World.
Perhaps older Unglossed readers are at least a bit more willing to entertain the first bullet, at this point, than when I first opined on the excess mortality question?
Perhaps the example of Hong Kong, where very few elderly have received any version of the Covid vaccine, and deaths are higher than elsewhere, has closed the “all the evidence can be explained away as healthy user bias” escape-route? But if not, just please keep in mind that the people of Bizarro World see things differently. They believe severe efficacy is real.
Given that the inhabitants of Bizarro World believe in the two bullets above, they see the question of excess mortality in 2021 differently than most of Covid vaccine skeptical substack. The US listed more “Covid deaths” in summer 2021 than in 2020. Using the cumulative death timestamps in Worldometers, they observe the following comparison between “summer Covid-19 deaths” in 2020 and 2021:
Oct 15 - July 15
2020
226,534 - 142,544 = 83,990
2021
748,469 - 627,080 = 121,389
Bizarro Worldians don’t look at this 40,000 increase and conclude that the Covid vaccines must not be effective. Instead they ask, why were so many unvaccinated Americans allowed to die? Why didn’t they receive effective therapeutics that can prevent severe outcomes and deaths just as well, if not better than the injections? And was something done to increase how many unvaccinated Americans died “with Covid”?
I know that to a Covid-vaccine-skeptical Earthling, these questions are also “of interest;” but the Earthling will nonetheless not accept that all 40,000 surplus deaths actually had anything to do with the virus, nor that they were among the truly unvaccinated, as matches government records, rather than the “secretly” (as in recently-dosed) Covid-vaccinated. The Earthling will dissect the data to bits looking for evidence that these deaths were just misclassified Adverse Events of some type.
The Earthling will even do this when the upticks in nationwide excess deaths match the surges in officially-recorded “Covid deaths”:


Delta wave by the numbers
Per the combined propaganda efforts of our illustrious government and corrupt state and regional healthcare organizations, absolute numbers of American deaths during the Delta wave primarily consisted of the unvaccinated,3 completely the opposite of more highly Covid-vaccinated countries:

Here, the CDC implies an unvaccinated death toll (78,256/.62 = 126,219) coincidentally similar to the overall summer death toll above (121,389). (Note that the CDC’s analysis excludes anyone who was between 1 dose and the 14th day after completing the “primary” series4).
To discount for the extra months in the CDC’s tally (the first half of July, the second half of October and all of November, all periods when deaths did not increase as much), a Bizarro Worldian will just say “100,000 unvaccinated Americans died in the summer, 2021 wave.”
Now, whereas an Earthling looks at this data and rushes straight to the nearest (equally unreliable) government figure for Covid vaccination uptake to try and demonstrate that the 100,000 “unvaccinated” were secretly just-dosed Covid vaccinated (even though those are excluded from the analysis), a resident of Bizarro World simply asks:
Why did 16,000 more unvaccinated Americans die in summer 2021 than in 2020, even though there were only half as many unvaccinated Americans in the second year?
Did American healthcare systems kill some portion of 100,000 unvaccinated citizens by denying them effective treatment, isolating them from family trying to follow up with care, and placing them on ventilators, all to receive payouts from the government?5

The Bizarro Worldian can’t look away from this question. Americans who walked into a hospital with a positive test for the virus have spent the last two years with a Government Bounty on their head. In summer of 2021, an astounding 100,000 unvaccinated Americans wound up dead; and American hospitals had the means, motive, and opportunity to “help” them get that way. Isn’t that a bit suspicious?
So the Bizarro Worldian, bizarrely, looks for a clue that the so-called “unvaccinated Covid deaths” were actually exactly what they were called. Finding the clue turns out to be as easy as using the region and age filters, back at usmortality.com.
Now, mind that the Bizarro Worldian, much like the Earthling, wants to look at what is happening in the non-elderly adult age groups. Essentially, both regard non-elderly adult mortality as a more “sensitive” gauge of an unusual change to background mortality rates, on account of those rates being lower than the elderly to begin with, but also not so low that a handful of deaths can cause wild swings in the trend, as with the young.
And so when viewing regional deaths in the 25-44 and 45-64 age groups, it turns out the United States did not have a summer uptick in excess mortality in 2021. Only the South, and portions of the Midwest and West. Whereas, in the Northeast:
25-44

45-64

Massachusetts, New Jersey, and New York had high Covid vaccine uptake, and should be the model for the impact of the injections on working-aged all-cause excess deaths. They suggest that the extra deaths do not correspond to injection roll-out. It is only the end-of-year upticks in Massachusetts that seem to support a signal for acute deaths following boosters (remarks in footnotes6).
In New York and New Jersey especially, the Covid vaccines are either apparently not driving extra deaths at all (there is no apparent response to in-age-group uptake), or they are doing so in a manner akin to ticking time bombs for all recipients. The Bizarro Worldian has no problem assuming the latter is the case. Microclots are ticking time-bombs. If that means that the death toll from the injections is essentially impossible to “prove,” so be it.
But what is more important is that all these states likely had high uptake of triple-dosing in these age groups, including illicit pre-approval boosting in August. If boosters were driving the summer uptick elsewhere, it seems fantastic that these states remained on trend through August, September, and October.
Meanwhile, Pennsylvania, the least-Covid-vaccinated state in the Northeast, is the outlier; it will resemble our Southern states in the next graphs.
Again, the Earthling visitor to Bizarro World has to remember the travel guide. They believe in severe efficacy in this planet. The way they see the issue, the “frying pan” is the Covid vaccine; the “fire” is the virus combined with hospital mistreatment; and the “jumpers” are the middle-aged American unvaccinated.
To see this dynamic in action, just observe how the deeper South mirrors the Northeast until the timeframe corresponding to the official nationwide surge in “Covid deaths”:
25-44
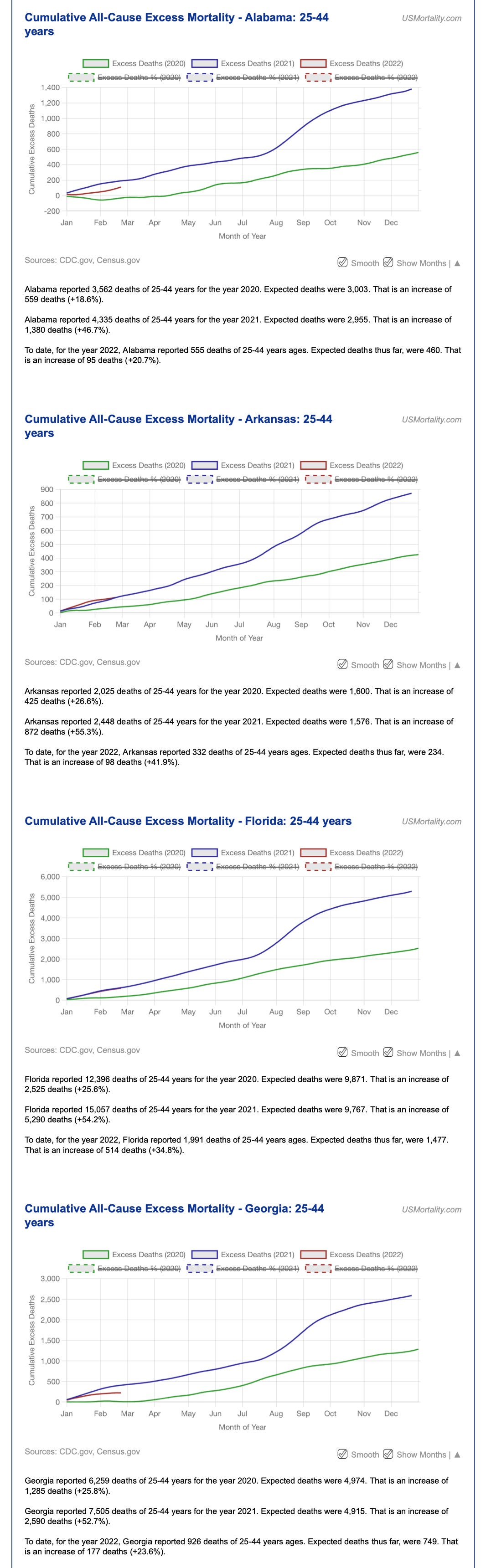
45-64

It would be overkill to show the other deeper-South states. For the Midwest and West, results are more heterogeneous by state, and are more distinct in the 45-64 group - but also contribute less to the absolute figures, compared to the South and especially Florida and Texas. There are, however, prominent upswings in that age group in California and some other Western states toward the end of the year, which could do with additional scrutiny (are these rural unvaccinated and infected, as matches news reports, or boosted?).7 But the example in low-uptake Southern states seems not to demand an immediate answer to the mixed-uptake California question.
To the Bizarro Worldian, there is no getting around it. The summer surge in excess deaths were the middle-aged unvaccinated, infected, and quite likely hospitalized, in precisely those regions from which anecdotes of family members being denied treatment and aggressively placed on ventilators were more frequent. Meanwhile, in the Northeast and West Coast, where high Covid vaccine uptake and severe efficacy kept the middle-aged out of the hospital, there were no unvaccinated middle-aged for the hospitals to kill.8

An “at the time” would be appropriate to append here. Hospitals in these states may have begun to make up ground in unnecessary “Covid deaths” in autumn and early 2022, as discussed in Footnote 6.
See “Invisible Apocalypse” and “Indiana Down.”
Indiana Down contains the Secret Third Bullet of the Bizarro World travel guide: The insurance executive never actually said most of the excess working age deaths are not “Covid deaths.”
Only 1 dose for the Janssen product; 2 doses for the other brands.
Note that actual payment practices after mid-2020 are extremely unclear. Funds for general support are backlogged, with a large dispersement in September only covering the period up to March 2021, before the Delta wave and associated unvaccinated deaths. See Goldstein, Amy. “Billions of dollars in pandemic aid for hospitals and nursing homes is being handed out.” (2021, September 10.) The Washington Post Democracy Dies in Darkness TM.
Friday’s announcement marks the first time any of the federal money intended to help the health-care system stave off financial hardship because of the pandemic has been handed out since President Biden took office.
A wide swath of the health-care industry has been voicing escalating complaints in recent months that the money was sitting unused, especially as the highly contagious delta variant fills hospitals in some parts of the nation with patients sick with covid-19, the illness caused by the virus.
Previous money, given out in three phases, was available only for financial burdens incurred in the pandemic’s first months, through June 2020, although the vast majority of infections occurred since then. The newly released money can be applied to expenses from July 2020 through March of this year.
At the same time, it doesn’t appear that direct treatment payments ever stopped. See Rabe, Layne. “Health district says hospitals get funding for COVID-19 cases- no profit gained.” (2021, October 13.) kmtv.com
Putting you first, we spoke with the South Central Health District to see if this was true. Brianna Bodily with the health district says hospitals only get more funding for COVID-19 cases because of the high cost of treatment for the virus.
She tells KMVT that hospitals don’t make money from COVID-19, but get funding for the very high costs of treating COVID. She said there is extra personal protective equipment that is needed when treating COVID-19 and it becomes extremely expensive if a patient needs to be on a ventilator.
Bear in mind, however, the low absolute number contained within those upticks, and that these could also be associated with breakthrough infections combined, again, with intentional hospital mistreatment. It is not as if no Covid vaccinated died in the summer (or autumn, in MA’s case) waves, and these deaths would likely be preceded by hospitalization, placing the patient under the same “CARES Act Bounty” as the unvaccinated hospitalized.

Miniaturized grabs for the aberrant Western states (click to expand). Hawaii 45-64 seems the most alarming, and not supported by official “Covid deaths” rates. Nevada and California seem to match “Covid deaths” California seems to have had a heavy healthy user bias (with immigrant middle-aged and elderly seeming to dominate hospitalizations in the press), and so is likely more akin to the South in the over-45 groups and to the Northeast in the under-45 group. My iPad got picky about where to auto-crop the graphs here:


So, returning to Bodily’s quote in Footnote 5, the issue is not that the hospitals are “padding” Covid cases. It’s that they are guiding their (unvaccinated) patients into the most expensive “treatment” path possible, which is naturally the least effective and most likely to get them killed.
I am also a resident of Bizarro world, at least to some extent.. the fact that the hospital protocols literally kill people is a massive thumb on the scale. My pro-vax father can't get past this because he has seen unvaccinated people die of covid or have terrible sequelae, and says they should have gotten the vax, without realizing that the proper comparison is to a treatment protocol that isn't designed to kill the patient. People also get wrapped around the axle on effectiveness and waning. From what I can tell, the shots initially have negative effectiveness and a higher odds of infection (the worry window), then are broadly effective for a period of time, and then may resume negative effectiveness after "waning". At least that's what the UK data appears to show. Many people latch onto the waning and then attempt to disprove the period of effectiveness, which actually does exist. But remember, it doesn't need to prevent or even reduce chances of contracting covid, it only has to increase your odds of staying out of a hospital!
To make things more complex you also have variants that very in vax effectiveness as well as underlying severity.
Anyway, I had also noticed what you point out about all cause mortality in the northeast. There's no question that the Bizarro world effect is in full force here. However, as far as vax injury, I don't think it's impossible to see in all-cause mortality. Some vax injury happens right out of the gate, but other shows up later as a slow drip. The key to analyzing all cause mortality is age stratification, because death rates in the people who were likely to die anyway swamp the numbers. Have you seen this write-up on german numbers? It's a slam dunk in my opinion (note that I'm unaware of the covid protocols used in german hospitals, they are probably not as bad as the US):
https://metatron.substack.com/p/excess-mortality-in-germany-2020
He also has a deep dive on massachusetts which also shows a lot of problems if you stratify:
https://metatron.substack.com/p/the-definitive-guide-to-covid-and?s=r
One interesting question is how the vax stacks up against vitamin D.. if that was enough to reduce severity to keep out of the hospital, would it fix the stats?
It would be helpful to reader to be a bit more concise.