Unlike other aspects of "lockdowns," banning visitors to nursing home residents was seeded in a mysterious 2016 revision to federal regulations. (Nursing homes, 2020: pt. 2)
Continued from Part 1 (introduction and overview).
Pop called them a last time a little after 8pm on 5 April, “hysterical” because management had taken away his mobility chair and put him in a bed without a call button. “His final words were, ‘I’m not going to make it out alive,’” the Montuores wrote. “That was the last conversation we had with him.”
Two days later they were told that Cognac was having trouble breathing and had an elevated heart rate, two signs of Covid-19 infection. They begged for a test. “No fever, no test,” they were told repeatedly by staff over the next few days.
At one point, a staff member used her personal phone to help Pop speak to his family. Then on 11 April the facility’s nurse practitioner called to tell them that Pop was failing; when they asked if he had Covid, she said no, heart failure.
A few days before the [October] protest, the Montuores found out that Pop’s roommate, Daniel Bartus, had died of Covid-19 on 5 April.1
Alabama National Guard Task Force 31, Soldiers, and Airmen disinfect Bill Nichols State Veterans Home in Alexander City, Alabama, April 18, 2020.National Guard (flickr.com) (CC BY 2.0)
Where did the incredible decision to ban visitors from nursing homes come from? Why were these bans implemented so swiftly, and so broadly?
Unlike much of the groupthink “plan” that led to lockdowns, it has no basis in the CDC’s 2017 guidelines for nonpharmaceutical interventions during a so-called pandemic (the source of the “flatten the curve” graphic, as reviewed last week2). In fact, that same document doesn’t even consider the question of limiting outbreaks in nursing homes; the phrase “nursing home” itself only appears in characterizing residents as a group at risk of “complications” from influenza-like infections.3
The Economist article which jumped the gun on promoting a society-wide “flatten the curve” effort is somewhat more prescient, briefly recognizing that nursing homes may be the grounds for “sporadic outbreaks,” caused by “the rare infected person” in the dreamland where everyone is doing their duty and staying home.4
If I am right that lockdowns were dreamed up by professional class “groupthink,” the case for this groupthink producing the idea of banning nursing home visits would be weak. At best, the professional class added an awareness of the problem of nursing homes, prisons, and other facilities to the simplistic “flatten the curve” dream in the days of early March.
The simple answer, of course, is that I am completely wrong — when it comes to the banning of visitors in nursing homes (and hospitals). Nor is this surprising — the theory that lockdowns were a result of mass panic was never meant to exclude other outlets of conspiracy and premeditation, and it makes sense that nursing home outbreaks would be included in the latter category.
This post will observe the following provenance on the rapid-fire ban on visiting nursing homes in early March, 2020:
A revision to Medicare regulations in 2016 inserted language for restricting visitors to prevent community-associated infections (however, this should not have applied to family).
Medicare issued a de facto nationwide ban on all visitors on March 9, 2020; followed by a de jure nationwide ban 4 days later.
States soon followed up with their own redundant bans.
There was no federal authority for banning family visitors “because virus”; in fact, it should have been prohibited.
However, changes to existing regulations enacted in 2016 nonetheless served as the pretext for the bans. The following timeline reviews how this came about:
As background, nursing homes and long term care facilities are subject to all-encompassing federal regulation in order to qualify for Medicare payments. The code describing these regulations, 42 CFR §483, received a first-in-fifteen-years revision in 2016.5
Lest one read too much into the Phase 3 timeline, the (potentially) relevant changes to the code were included in Phase 1. Among these was an expansion of the rationale for restrictions that may be applied to “other” visitors.
How the revised law, 42 CFR §483.10(f)(4), could be the basis for banning family, even though it explicitly does not allow homes to ban family on “clinical and safety” grounds, in fact it forbids it, will be discussed below.
The commentary associated with the 2016 revision somewhat clearly associates this change with disease mitigation, at least in 3rd party sources citing CMS comments that I haven’t located:
Immediate access must be provided to immediate family and other relatives, subject to the resident’s right to deny or withdraw consent at any time.
Other visitors must be provided immediate access to a resident, subject to the resident’s right to deny or withdraw consent at any time, and also subject to reasonable restrictions that, according to newly added language, must be based on clinical and safety concerns.
In the comments to the regulations, CMS gives some examples of clinical and safety restrictions. A clinical restriction could be limiting visitors to prevent the spread of communicable disease.6
[Note, again, this only applies to “other visitors.”]
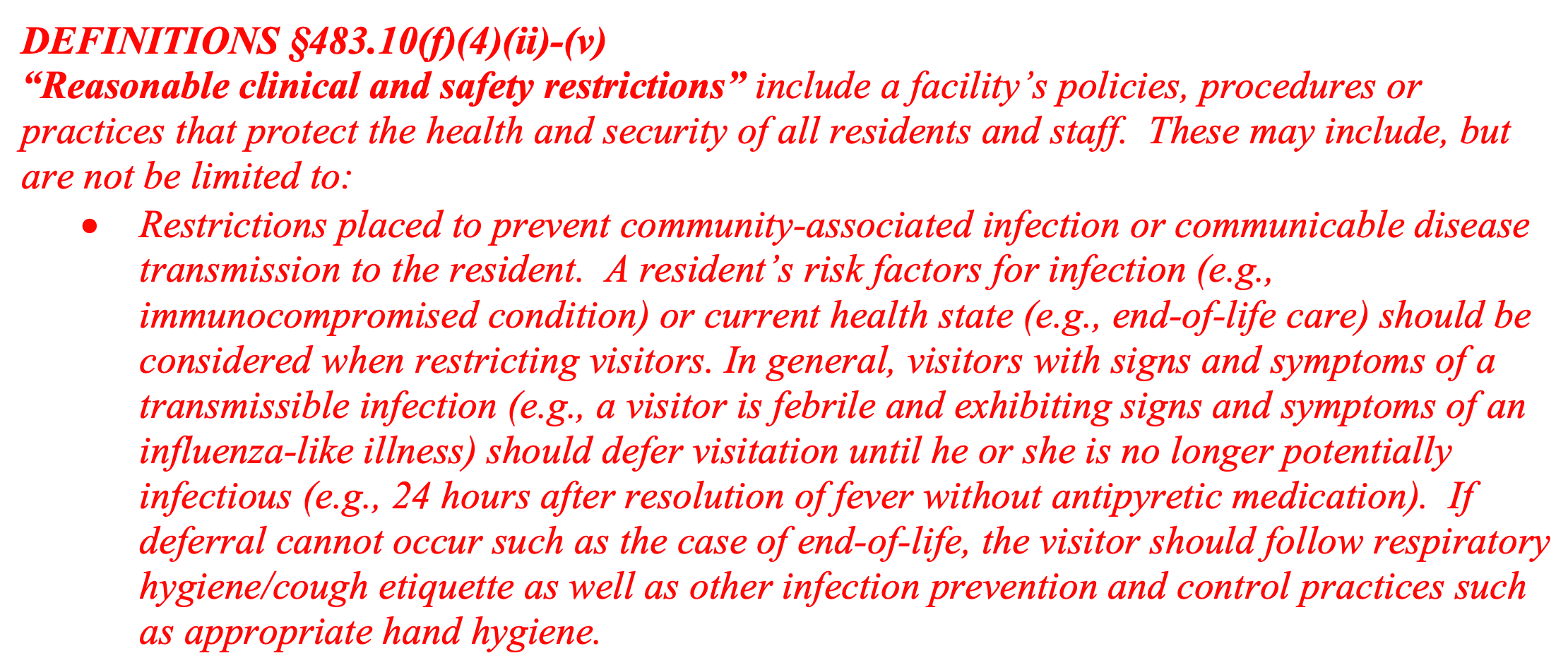
The 2016 revised regulations are then translated to the updated “manual” for state surveyor guidance in 2017, with a specific insert defining “clinical and safety concerns.” As such, the mandarins in charge of inspecting nursing homes for compliance nationwide are to understand:
DEFINITIONS §483.10(f)(4)(ii)-(v) “Reasonable clinical and safety restrictions” include a facility’s policies, procedures or practices that protect the health and security of all residents and staff. These may include, but are not be limited to:
Restrictions placed to prevent community-associated infection or communicable disease transmission to the resident.
Surveyor manual “tag” F563 is important in the implementation of the ban itself.
Summary of the legal background:
No authority was granted to restrict family visits against resident wishes; all homes denying family were in fact in violation of Medicare compliance.
The “clinical and safety restrictions” for “other visitors” is not prescriptive. They are measures homes may choose to take, not that they have to take.
This is affirmed in the surveyor guidance:
If limitations are placed on a resident’s visitation rights, the clinical or safety reasons for the limitations and the specific individuals the restriction applies to must be communicated to the resident or resident representative in a manner he or she understands.
March 9: And then Medicare just bans visits anyway
Here, again, the centralized, top-down imposition of the nursing home ban is clear, as the Medicare Oversight office pushed out the policy directly to all 15,000+ facilities in the US that qualify for payment on March, 9:
From: Director / Quality, Safety & Oversight Group
Guidance for Limiting the Transmission of COVID-19 for Nursing Homes
How should facilities monitor or restrict visitors? If visitors meet the criteria below, facilities may restrict their entry to the facility. Regulations and guidance related to restricting a resident’s right to visitors can be found at 42 CFR §483.10(f)(4), and at F-tag 563 of Appendix PP of the State Operations Manual.
Facilities should actively screen and restrict visitation by those who meet the following criteria: […]
Residing in a community where community-based spread of COVID-19 is occurring.
Nursing homes should not allow visitors into their facilities who live in a place "where community-based spread of COVID-19 is occurring," or meet other criteria, according to new recommendations from the Centers for Medicare & Medicaid Services.
Four days later (and some hours after the original version was archived on Wayback), the Medicare guidance office issued even sterner language, converting their de facto national visitor ban into a de jure national visitor ban:
Although citing 42 CFR §483.10(f)(4) and F-tag 563, the March 9 ban is totally unsupported by the law and existing interpretation in the manual — at best, Medicare could have recommended considering restrictions on “other” visitors. Yet it implicitly and then four days later explicitly mandates banning family.
It’s additionally notable that the same March 9 document delivers the contradictory discouragement of transferring infected residents to hospitals, and requirement of re-accepting recovering residents.
When should nursing homes consider transferring a resident with suspected or confirmed infection with COVID-19 to a hospital?
Facilities without an airborne infection isolation room (AIIR) are not required to transfer the resident assuming: 1) the resident does not require a higher level of care and 2) the facility can adhere to the rest of the infection prevention and control practices recommended for caring for a resident with Covid-19.
When should a nursing home accept a resident who was diagnosed with COVID-19 from a hospital?
A nursing home can accept a resident diagnosed with COVID-19 and still under Transmission- Based Precautions for COVID-19 as long as the facility can follow CDC guidance for Transmission-Based Precautions. If a nursing home cannot, it must wait until these precautions are discontinued. [This guidance is essentially a catch-22 requiring acceptance of released patients.]
How can mandating restrictions on family visits protect residents from infection, if potentially still-contagious residents are simultaneously mandated back in?
March 12: States double down
And so with this one document, the stage is set for the 1,000s of deaths that would occur in New York, New Jersey and elsewhere one month later.
Besides that, an entire nation’s elderly and other institutionalized dependents have now been deprived of not just social stimulation, but the advocates who ensure that staff know what they actually need on a daily basis. They have been cast into an abandoned cage, left to fend against, well, at least a rather aggressive bobcat. 1 out of 6 occupied beds would be vacated over the next year (hopefully partly due to relocation).
(Take note of the 16% / 1/6 figure; it will be a repeating theme.)
Who wrote the visitor ban memo? One David Wright, director of the same Medicare Quality Safety & Oversight Group on the letterhead. And was he the “author,” or merely signing off on a policy hastily designed by the Trump administration — as suggested by the rapid revision and expansion of the ban?
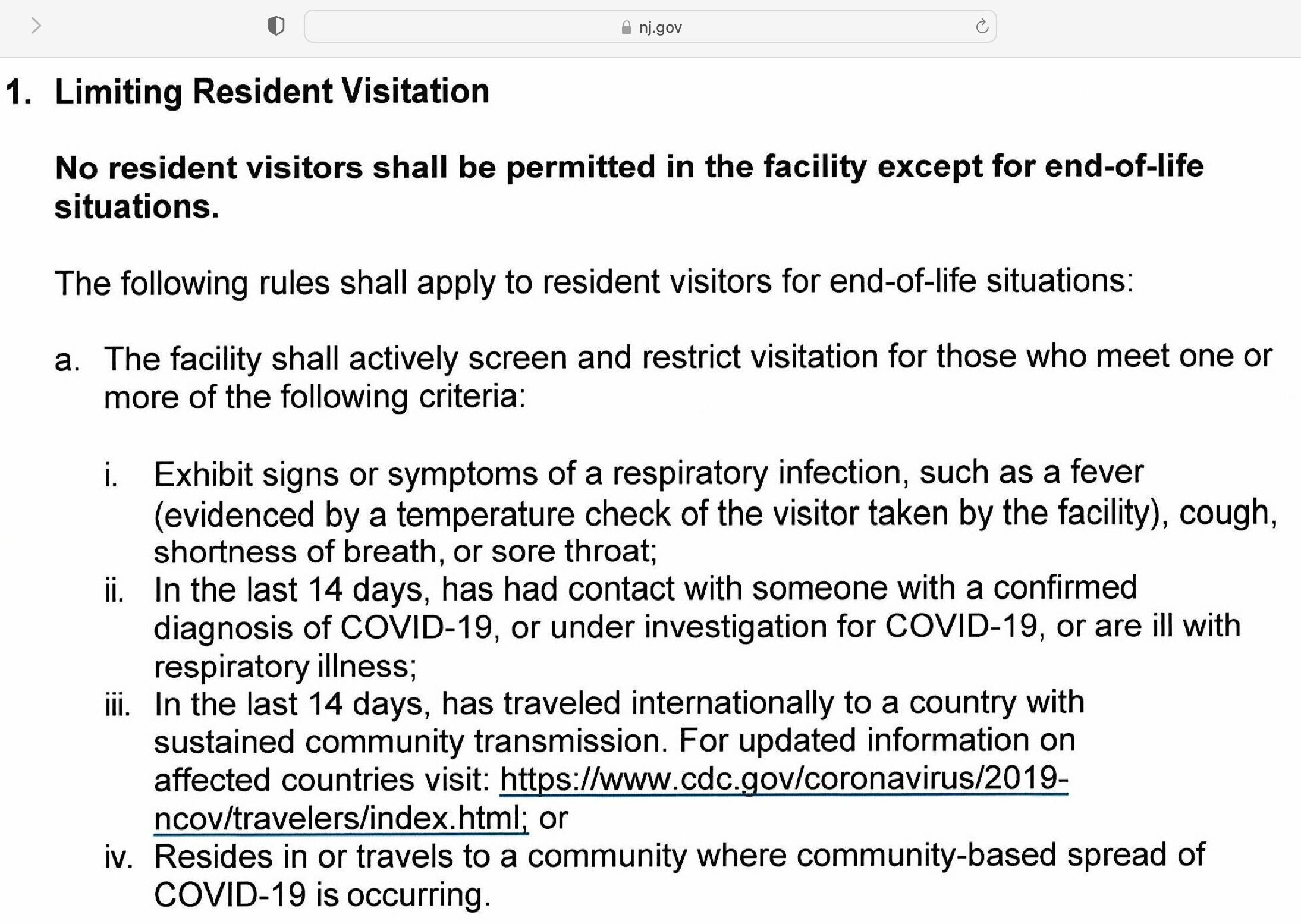
In a way, these questions do not matter, because institutions and states were soon to add their own redundant bans as part of the overall “lockdown” package; and these bans would not depend on 42 CFR §483.10(f)(4), nor be obviously legally vulnerable to a challenge on the basis of it (thanks to the “Limiting the Transmission” guidance explicitly dictating that visitor rights will not supersede state bans). Veterans Affairs homes were covered by a redundant ban starting on March 10.7 New York state published its own visitor ban on March 13; followed by New Jersey a few days later.8
March 16, 2020. nj.gov (pdf) Another catch-22: No would-be end-of-life visitors residing in New Jersey could possibly qualify.
The radical, astonishing notion of leaving a group typically dependent on rights-advocates to fend for themselves had successfully been injected from the federal government into a nationwide, state government program, one that received no meaningful protest from cowed citizens.
March 12: And citizens do nothing
Even if, unlike the overall script of “lockdowns,” the nursing home visitor ban was conceived and dictated in a top-down manner, it remains that no tanks and storm-troopers were required to enforce it. Not only did individual states quickly add their own bans, but visitor bans were generally embraced.
I say generally, because here, unlike lockdowns in general, at least some people seem to have realized immediately that these policies were overtly harmful, and inviting of disaster. Meanwhile, some long term care facility employees seem to have been optimistic that being left responsible for patients for an undefined amount of time without visitor advocates to help them assess needs would be, well, just hunky-dory:
All of these reactions, besides the insightful comment by @j_wingfield10, could perhaps be defended in retrospect by the argument that “This incredibly radical, seismic change to how we interact with the vulnerable who are already marginalized from society couldn’t possibly have been predicted to cause mass harm in advance.”
Except that is an obviously, intrinsically stupid belief!
It’s the same obviously, intrinsically stupid belief that led to abandoning children; it’s the same obviously, intrinsically stupid belief that led to abandoning demi-homeless (car dwellers, etc.) who relied on public facilities; and the same belief that led to abandoning millions of small business owners, active prisoners, and etc. and etc. and etc.
It is exactly the belief for which I hold and have for three years held Americans themselves responsible for lockdowns to begin with. We complied with this disaster; and by doing so, empowered it.
The whole point of conservatism is you do not suddenly change the world overnight because you are scared; rather, you assume the status quo has unperceived benefits.
The only framework in which the obviously, intrinsically stupid belief “made sense,” from the perspective of the communally housed elderly who were especially vulnerable to the viral “bobcat” they had been left to fend with, was under the magical assumption that visitors staying home would prevent transmission, even though workers still had to come to work every day. (After all, that’s what the “flatten the curve” graphic said would happen, and it’s Science, so it must be right.)
Was this the same assumption behind the bans to begin with? Or were nursing home residents simply being sacrificed in a maniacal and self-defeating effort to “avoid healthcare collapse”? Or, worst of all, was the intention a mass die-off in the first place? If it wasn’t stupidity, it was premeditated murder either way.
At all events, with the legal framework behind nursing home visitor bans now established, let us assess the disaster in New Jersey.
“Residents of nursing homes” are listed between pregnant women and American Indians as a group at risk of complications from infection; no mention is made of measures to prepare for or respond to viral outbreaks in homes. The list of “community settings” to which social distancing measures might apply is limited to:
educational facilities, workplaces, and public places where people gather (e.g., parks, religious institutions, theaters, and sports arenas
Whether school closures are proposed but nursing homes and prisons are omitted from consideration is because the CDC report seeks not to appear radical (and be blamed for any future radical government measures), or because it is assumed that keeping kids from school will somehow protect adults confined to communal living, is unclear.
However, I do not see any such elaboration in the comments actually printed in the preamble regarding the change; it is merely stated that the text is added:
“Then on 11 April the facility’s nurse practitioner called to tell them that Pop was failing; when they asked if he had Covid, she said no, heart failure”
Normally if a resident is suffering unstable heart failure they get sent to ER. They seem to have stopped doing this, and may also have curtailed services relating to feeding and hydration.
One of the purposes of restricting visitors is so they cant see the culling that occurred in some care homes. This was also done in other countries like UK. Remarkable coordination.
Fed money offered as incentives to states that went along
For whatever reason, Ontario nursing homes immediately adopted the same rules on March 9 2020 even though there was no such 2016 revision to guide our public health regulations. When the gene jabs became available, Ontario nursing homes extorted 'consent' from every worker for two jabs to stay employed, and on civilian family members and visitors to be allowed to visit - but inexplicably, residents could refuse without punishment. Nursing homes lied to the public and their workers and called jab requirement a legal provincial mandate, despite the fact that the Ontario government had never imposed a gene jab mandate on publicly funded health care facility staff or civilians. As a result of this lie, I was forbidden to care for my elderly mother for almost three years while their neglect and stupidity caused her incalculable suffering and preventable infections and deterioration.



")











“Then on 11 April the facility’s nurse practitioner called to tell them that Pop was failing; when they asked if he had Covid, she said no, heart failure”
Normally if a resident is suffering unstable heart failure they get sent to ER. They seem to have stopped doing this, and may also have curtailed services relating to feeding and hydration.
One of the purposes of restricting visitors is so they cant see the culling that occurred in some care homes. This was also done in other countries like UK. Remarkable coordination.
Fed money offered as incentives to states that went along
For whatever reason, Ontario nursing homes immediately adopted the same rules on March 9 2020 even though there was no such 2016 revision to guide our public health regulations. When the gene jabs became available, Ontario nursing homes extorted 'consent' from every worker for two jabs to stay employed, and on civilian family members and visitors to be allowed to visit - but inexplicably, residents could refuse without punishment. Nursing homes lied to the public and their workers and called jab requirement a legal provincial mandate, despite the fact that the Ontario government had never imposed a gene jab mandate on publicly funded health care facility staff or civilians. As a result of this lie, I was forbidden to care for my elderly mother for almost three years while their neglect and stupidity caused her incalculable suffering and preventable infections and deterioration.