


Week-End Review: 22.4.8
Quick takes on notable studies, etc.

(A new but old format, to offer the reader short reviews of the more salient elements of the latest week in noise. Full housekeeping-type announcement in the footnotes.1)

On the docket:

Sweden “33 Times!” Study!

The Headlines
“Covid” Super-Multiplies Risk of Bleeding Complications!3
My Quick Take
Although a well-designed study in other respects, the authors made the hard-to-forgive decision to lump together patient outcomes from spring, 2020 and afterward.
The paucity of testing in the first Sweden wave ensures that first-wave “cases” are largely limited to those who required medical care.
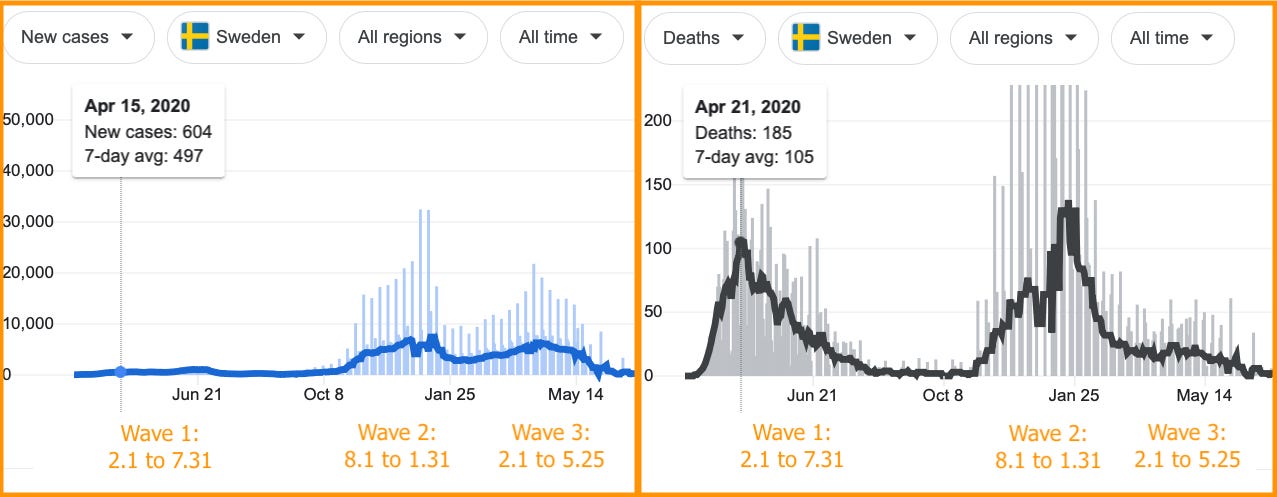
“Cases” and deaths during Katsoularis, et al. study windows. This makes the definition of a “case” within the study wildly inconsistent. And compared to strictly measuring results when testing was more robust, it weights the overall meaning of “case” to some extent toward severe infections.4
Although un-tested mild cases might also drive up control events, this would not be proportionate to the control denominators (and would probably not come into play in the self-controlled portion of the study, in light of natural immunity).5
This is not a new problem; it largely drives the high rates of clotting complications in early 2020 studies which are abundantly mined for headlines already.6 It’s just surprising to see this problem recycled in a study published in 2022!
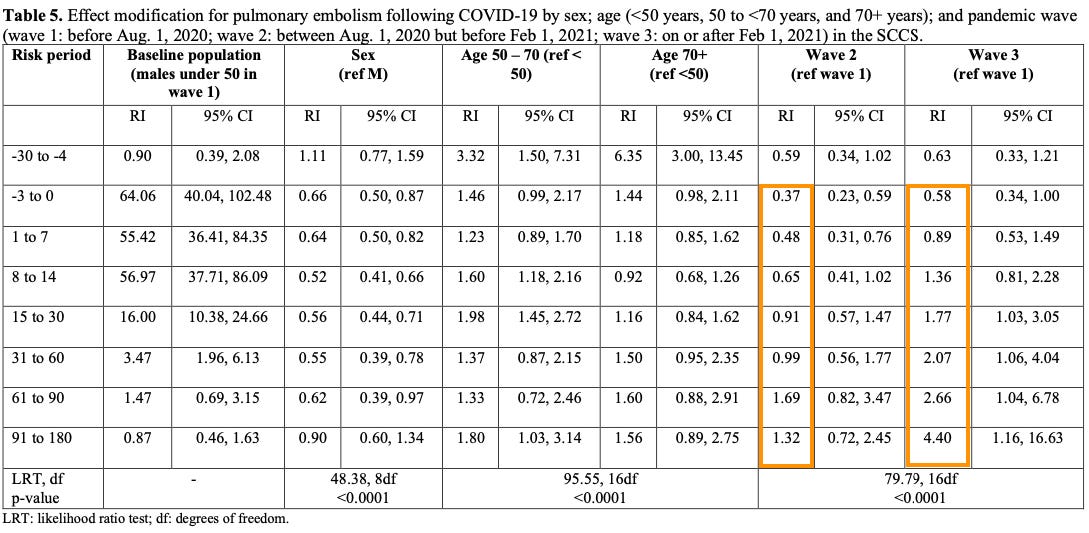
Inferring from Supplementary Tables 4-6, this seems to particularly exaggerate the risk for Deep Vein Thrombosis and “Bleeding,” but not so much for Pulmonary Embolism (which drives the headline “33 Times!” value. (Wave 2 and 3 rates seem consistent in balance with Wave 1, though it would require a lot of math to verify things here.7)
The high rates for Pulmonary Embolism are not surprising given prior research.8 Still, the headlines that vaguely associate this risk increase with all three outcomes, or fail to specify the large disparity in risk between mild (6.77 times risk) and hospitalized (139 - 289 times risk) cases, are rather deceptive. Moreover, relative risk is not absolute risk: In all, the added risk from mild infection seems to have driven a couple hundred events in a non-locked-down, mostly non-vaccinated population of ~5 million during the entire study period.

Katsoularis, et al. Fig. 3


BioNTech Omicron Breakthrough Study!
The Headlines
Well, there haven’t been any. But what the headlines should say is, “OAS Proven False for 900th Time!”10
My Quick Take
While I may yet devote a full post to the study, I have a bit of hesitation about over-hyping “simulation”-based (neutralization assay and flow cytometry) results as any kind of surrogate for real-life observation of post-infection resistance against reinfection;11 let alone results obtained almost entirely in-house by BioNTech.
Still, even if the study doesn’t prove anything about post-Omicron immunity, it does totally refute the “mechanism” invoked by those who argue that the Covid vaccinated are going to be afflicted with the unreal, mythical phenomenon known as “OAS.” In what ways?
Plasma from post-Omicron-infected Covid vaccine recipients, in this small sample, inhibit both BA.1 and BA.2 in neutralization assays (whereas (non-longitudinal) uninfected Covid-vaccine recipient samples fail to do so, particularly in the not-recently-2nd-dosed group). Crucially, the breakthrough-infected plasma samples score a coveted “1” in the Wuhan/BA.1 neutralization ratio in the live virus challenge.

Quandt, et BioNTech. Fig 2. This might not be relevant for long-term immunity, but it still demonstrates that “immune imprinting” does not forbid generation of a novel, anti-variant spike immune response in any way. Since the myth of OAS is wedded to antibodies, which are all that is measured by neutralization assays, these results refute OAS (as did the results in Rössler, et al., though I didn’t mention it at the time12).
The flow cytometry results score fewer hits against OAS, potentially due to differences in the sensitivity for measurements of “Wuhan” and Omicron-tailored Memory B Cells which may partially be driven by time of sample.13
See previous posts for more in-depth discussion of why OAS is not real:


CDC “Cardiac Complications” Study!
The Headlines
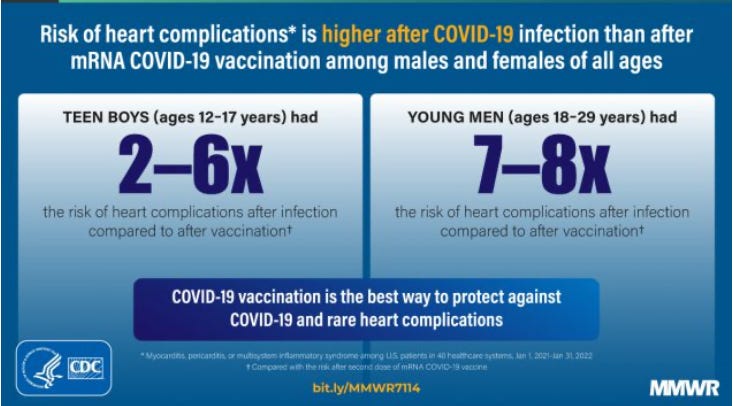
As spoon-fed to the media in the graphic above!15
My Quick Take
Unlike similar studies conducted in other countries, the database involved in this study does not have comprehensive data for patient infection or Covid-vaccination events. Since the under-reporting factor for either category is unknown (how many patient infections were not recorded in the system; and how many patient injections?16), comparing associated cardiac events is impossible. Even if one undertook two separate underreporting analyses on the data, the fidelity of the adjusted rate comparison would be not much better than a random guess.
As always with MMWR propaganda, the weakness of the study is conveniently acknowledged in the “at least X limitations” list. This one’s a doozy:
Third, only SARS-CoV-2 test results and mRNA COVID-19 vaccinations documented in EHRs were available for assessment. SARS-CoV-2 infections were not captured if testing occurred in homes, schools, community sites, or pharmacies. Similarly, EHR data in this study captured ≥1 dose of mRNA COVID-19 vaccine for 28% of persons aged ≥5 years. Nationally, 82% of persons aged ≥5 years were reported to have received any COVID-19 vaccination; 97% of all vaccinations administered were mRNA COVID-19 vaccines. Underascertainment of SARS-CoV-2 infections and mRNA COVID-19 vaccinations reduced sample size and might have introduced bias if capture of infection or vaccination within the EHR occurred differentially for those with cardiac outcomes. Fourth, case definitions for myocarditis, pericarditis, or MIS were ICD-10-CM code–based; diagnoses were not confirmed with chart review and are subject to misclassification.
The more reliable studies, which obviously will never make it to the headlines, are those which have a robust view of patient outcomes; such as the one that found scores higher likelihoods of myocarditis from the Covid vaccines for males under 40.
The UKHSA Blackout (Is for the Best)!
The Headlines
As alarmingly phrased above!
My Quick Take
The last two years of endless mass testing have been more illuminating than some predicted (the problem of false positives turning out to be not as bad as expected). Still, ending mass testing can only help push the West toward “moving on” from the virus.
The end of free testing for low-risk groups in the UK would only exaggerate the risk of the virus, as well as increase bias between the Covid vaccinated and not. So, the stated rationale is reasonable.
I really don’t trust the denominator used for the unvaccinated in the UKHSA dataset any more anyway. I do not think it is accurate to call the UKHSA “the best source of raw data,” for example, when the unvaccinated population is calculated indirectly.18
So, this is all fine with me.
Recommended Links!
“BEAK MASKS,” by Joel Salatin. (Hat-tip to 2SGITW.)
As avian influenza runs through the nation’s poultry flocks, with the current extermination of about 28 million laying hens and turkeys, I can’t help but wonder why we aren’t putting beak masks on the chickens. […]
Hmmmm, I wonder if decentralization of poultry would be better than centralization. Notice that on one farm, 5.8 million laying hens were destroyed—ON ONE FARM!
It’s all blamed on wildlife. Folks, whenever a culture views wildlife as a liability rather than asset, you know everything is wonky. It’s like blaming babies for drug addiction. Or blaming churches for drunkards. When wildlife is the enemy, something is out of whack in the culture’s thinking.
“UBS Debates: What Did the Massive Bangladesh Masking Study Really Find?” by James Lyons-Weiler.
Dr. Jason Abaluck and Dr. Lyons-Weiler agreed to compare notes on Dr. Abaluck’s study on masking in Bangladesh. What do you think Dr. Abaluck is safe in concluding?
See also my notes in the comments, and the follow-up post by Lyons-Weiler in which Abaluck rage-quits an email exchange.
“The Meta-Analytical Fixers, Part III: Defamation of Paul Marik, Take Two.” by Mathew Crawford.
Sheldrick [who recently accused Marik et al. of fabricating data in a 2017 Sepsis study] seems to think this won't have a substantial effect on his probability calculation, but having built an artificial intelligence system that crunched dozens of variables for the purpose of stock trading, I can guarantee that he is very wrong […] Computing p-values without respect to these correlations is wholly inappropriate, and not particularly meaningful. The results can be off by orders of magnitude. Sheldrick's casual dismissal of this hurdle is frightening. I'm frightened for him and the legal fees he may suffer.
Random Object #1!
Though less dramatically to-the-wire than Bron’s 2019 race, this one wins in “mood-enhancing helicopter flybys.”
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.21


While Friday multi-topic posts were pretty frequent here at Unglossed last summer and autumn, they became superfluous once the the big questions surrounding Covid vaccine (non-) efficacy were resolved, and the media exaggeration of the risks of the virus had been discussed ad nauseam. For me to spam the reader with study reviews that don’t reverse or challenge those prior conclusions seemed pointless.
This weeks’ Sweden study, especially, demonstrates that even if certain orthodoxies have become obsolete, the media will still hawk “fresh” evidence to support them. So, I’ve revived the multi-topic format to offer the reader quick notes on studies that don’t reverse or challenge prior conclusions.
Related: Regular Service Resumption Notice
The last two weeks were split between several overdue household errands and a lot of core research. Output should return to a normal level beginning this weekend.
(link anchor)
For example, using cumulative figures for July 31, 2020 in worldometers produces a first wave case fatality rate of 5,726 / 76,686 = 7.5% for the defined “1st Wave” period! See https://www.worldometers.info/coronavirus/country/sweden/
In other words, the “baseline” against which post-infection outcomes were measured would include some number of events potentially prompted by untested 1st Wave non-severe infections. However, the impact of these excess events on the baseline would only be proportionate to the amount of person-time spent post-mild infection in the control group, which would be marginal. Moreover, these events would likely not make it to the baseline for the self-control analysis, since few 1st Wave convelescents are likely to have gone on to test positive again in the remainder of the study window (see NIII: Pt 1.)
As complained about way back in “Where Free Thought Dies.”
Supplementary Tables 4-6:


(Reference pending.)
(link anchor)
Quandt, J. et al. “Omicron breakthrough infection drives cross-variant neutralization and memory B cell formation.” biorxiv.org.
Unlike some authors…
See “Austria Omicron Study.”
Limitations previously discussed in “Macaque to the Future.” Applied here:
Memory B Cells for Omicron spike may still be undergoing enrichment in germinal centers, and thus have a lower affinity for the Omicron spike tetramer (“Limitations of this study are that the data were generated from blood samples obtained a few weeks after Omicron infection. Later time points might reveal formation of memory responses against novel epitopes that are not yet visible.”).
Additionally, Omicron spike may just not bind as strongly to B Cell Receptors due to differences in chemistry vs. the classic model; or Omicron infection may prompt enhanced immune response against the more broadly-shared “C-terminal” epitopes of the spike protein (a suggestion offered by the authors in the Conclusions section).

Quandt, et BioNTech. Fig 3.

An“OAS Fanatic” could torture the Fig. 3 results and associated discussion text to rescue the OAS myth from oblivion, if they really wanted to. However, Fig. 4 demonstrates that breakthrough infection leads to an increase in cross-recognition Memory B Cells vs boosting; I would argue that the flow cytometry results are not of high enough quality to take any leaps from; and the study authors themselves feel that the neutralization assays override the other results. (“In aggregate, our results suggest that despite possible imprinting of the immune response by previous vaccination, the preformed B-cell memory pool can be refocused and quantitatively 15 remodeled by exposure to heterologous S proteins to allow neutralization of variants that evade a previously established neutralizing antibody response.”)
(link anchor)
Both categories could further suffer from underreporting via misclassification of cardiac events, as suggested in the papers estimating underreporting after injection by Sharff, et al. (For a review, see Rose, Jessica. “Kaiser non-permanente?” (2022, January 3.) Unacceptable Jessica.)
(link anchor)
Or at least, I think the Israel Ministry of Health data is better here, even if the unvaccinated population is counted by the same means. The smaller population and lower Covid vaccine uptake seem to reduce the “unvaccinated population overestimation hazard” (or what I have previously termed the “Iceland Dashboard Bias”).
(link anchor)
(link anchor)
(Add’l housekeeping notice for longer-term subscribers: Going forward, I am replacing the monthly “drive” model with per-post donation solicitation. However, I will continue to try to create value for long-term readers via monthly “magazine-worthy” articles!)
actually requiring medical care would seem an eminently better proxy for an illness named Severe Acute anything than a useless overamplified PCR test with staggeringly useless level of false positives.
So my overall sense of outrage/injury makes me want every study to "prove" that the vax is creating exactly what was predicted by warnings of Geert Van den Bossche. Only because in real world examples the denial of vaccine injury are pervasive. We recently had a patient 30 year old woman came in to the psyche unit with severe depression r/t new onset migraines and tinnitus, tremors, severe paroxysmal tachycardia...onset 3 days after 2nd vaccine. No previous issues at all. Looking through the chart, my daughter who works as a CNA offered the possible explanation of vaccine injury and was shot down. (even though her NP quietly admitted she could be right). Meanwhile every test imaginable was done to find out what was going on. Of course they found nothing so discharge was planned, she was started on antidepressants and before she left the physicians encouraged her to take the booster. She declined. So anyway I love the deep science even though I usually have to read these studies several times to understand, even remotely, what is being said. Back to my first statement, you, and a couple other science type stacks, keep me HONEST.
Brian I recognize that you have devoted a lot of time simplifying these ideas for me. I would love to know what you think about Geert and his ideas, the VAERS reports, sudden deaths, collapse of athletes ect. I realize there is a difference subjective/objective but the ongoing denial of anything but the "safe and effective" vaccine narrative continues to perpetuate vaccine injury INJURY.
When I began this journey I diligently read all the most current studies from journals about covid immunity of the infected. The studies, month after month post covid onset all found "broad and durable" immunity. Then the vaccine came along and suddenly, even though the "broad and durable" immunity was still acknowledged..." by almost everybody (except that idiot at the NIH leading the country in worship hymns to himself) "BUT, you should get the vaccine as additional protection, because we don't know how long natural immunity will last".
I'm probably going to have a heart attack because of my continuous head spinning frustration, but at least they won't be able to attribute it to a "coincidence" post vaccine.