


The Austria Omicron Study
A hodgepodge of unique outcomes with no clear meaning.

After months of natural immunity outperforming injection-based immunity,1 a small Omicron study has generated fodder for the humiliated pro-injection side. But for the unvaccinated, is the news really that “bad”?

The Set-up
Rössler, et al. wanted to see whether blood samples from people who recovered with infection from BA.1 (“Omicron”) were any good at stopping different versions of the virus in a simulated neutralization assay.2 Why?
Well, because earlier, other studies had looked at how well blood samples from people not infected with Omicron were at stopping Omicron in a simulated neutralization assay. The information gleaned from these tests allowed other scientists to repeat the information and make wild guesses about what the information could mean. So, naturally, this study adds new information to make wild guesses about. This is just a thing you do, if you are Science.
And so the authors collected blood samples from Austrians who had recently recovered from infection with BA.1. Some were truly “SARS-CoV-2 naive” (unvaccinated with no previous infection), some were previously infected, some were Covid vaccinated, some were both.
They took the serum (the part without blood cells) from these donor samples, mixed it with calibrated doses of different variants of the virus, and dumped the result onto some Vero cells (modified to express ACE2 and TMPRSS2), to see how many got infected.
It’s a tired gimmick, at this point - and yet it happened that the authors found some interesting results: In this small sample, BA.1 infection wasn’t a very good way to make serum that will protect Vero cells from the virus, even after “moderate” infection, as we will discuss below.
But interesting as these results are, they aren’t groundbreaking, or revelatory. They cannot predict the future in terms of real life immune response.
Broken Record
Antibodies, especially circulating antibodies in the blood, are not the full story of immunity to a respiratory virus. And yet that is all that neutralization assays can measure. They are akin to attempting to gauge whether a space probe will successfully land on Venus by burning a cup’s worth of rocket fuel.
It is no more appropriate to use a few convalescent blood samples to conclude that the Covid vaccinated are trapped in some make-believe immune imprinting purgatory,3 than that the unvaccinated’s “so-called ‘natural immunity’” is “clearly rubbish.”4 Either claim is a sign of raw desperation.

So-called "natural immunity" against COVID-19 has always been a dodgy argument for avoiding vaccination during the pandemic.5 But amid omicron, natural immunity is clearly rubbish.
Unvaccinated people who recover from an omicron coronavirus variant infection are left with paltry levels of neutralizing antibodies against omicron. They also have almost no neutralizing antibodies against any of five other coronavirus variants, including delta.6 People who were vaccinated before getting an omicron infection, however, have strong protection against all five variants, and they have some of the highest levels of neutralizing antibodies against omicron.
If you have been hypnotized into imagining you are a mother eagle who has to keep a nest-full of babies alive with regurgitated, party-line affirming “proofs” that nature somehow has no idea how to run the immune system, it’s no surprise that the study by Rössler, et al. would seem like a feast compared to the last six months of famine. But if you haven’t been hypnotized into imagining the above, you probably would recognize this study as the tiny scrap of data that it is. There were 59 donors, so a handful of outliers in any group could have radically altered the results.
And so, the study shows that Omicron leads to “moderate” infections, in that a handful of moderate infections were reported. And the study shows that Omicron “doesn’t generate a high level of neutralizing antibodies,” only after a year of real-world experience demonstrating that a high level of neutralizing antibodies is such an ephemeral status anyway, with no practical significance in the long run, that it’s long past time we stopped caring. What better argument for doing so than Mole’s own words a few months prior?7
That data—which we'll get into below—has consistently shown that immune responses from natural infections are extremely variable, thus unreliable. Vaccines, on the other hand, have repeatedly been proven to generate highly protective immune responses.
And yet the variable “immune responses” (here, naturally, she only was referring to antibodies,8 having presumably received her PhD for successfully memorizing cartoon biology shorts from the 1950s) proved reliable, and the repeated (as in non-variable) immune responses proved unreliable. The entire “consistent antibodies = better immunity” argument of summer, 2021, went down like the Hindenburg.9 This fact doesn’t stop being true merely because Omicron has come along to douse the embers with a bit of rain.
To measure immunity to this virus, we must measure reinfections, the same way it has been done since the concept of immunity was first observed.10 Anything else is a false idol.
Response
Absent observation of real-world immunity/reinfection, the results obtained by Rössler, et al. are more an assortment of anecdotes than a guidepost for the future.
The antibody results are all but useless. Helpfully in this regard, the authors go through the trouble of plotting neutralization results by day of sample (post BA.1 infection), demonstrating the importance of waiting for seroconversion (the arrival of new antibodies) circa day 12 or later:
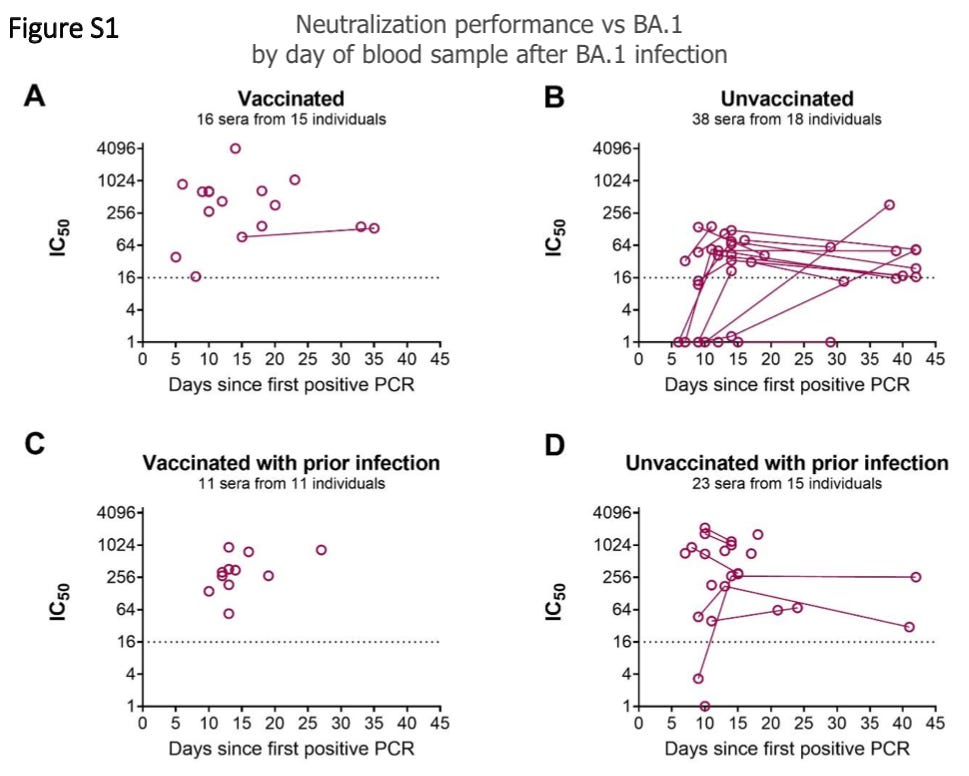
So, beyond the first few days, among the unvaccinated, few changes are apparent. And very little duplicate sampling took place among the Covid-vaccinated. So in summation, it’s impossible to tell whether infection with BA.1 is actually inducing any kind of “response” among the Covid vaccinated to begin with. We could just be seeing what was already the case before infection - in fact, the strong showing in early (pre-seroconversion) Covid-vaccinated samples suggests this is exactly the case.
In other words, the higher points on these graphs might not correspond to the antibody response “elicited” by Omicron per se, but to the aberrantly high-affinity immune response elicited by pre-Omicron versions of the virus. In such a model, the “unvaccinated, uninfected” group (after the first few days) represents the maximum antibody-affinity that the BA.1 version of the spike protein can generate (which goes up over time, but still settles at a low level), and the other three groups are merely reflecting the high-affinity response previously primed by exposure to the pre-Omicron spike.
In other other words, all the authors have demonstrated is that BA.1 is not very antigenic - regardless of mildness (as in, even if symptoms were reported as “moderate”).
And that is where the results prove interesting.
And Call
While the antibody / neutralization values are vague, the values for symptom severity and patient demographics are quite rich.
From these, it may be gleaned that the (possible) low-affinity antibody response elicited by Omicron infection doesn’t seem to be a result of universal mild infection. Potentially as a result of the skewed age of the naive unvaccinated, or other host/virus factors, or simply the luck of the low-sample-size-draw, there were several “moderate” infections in this group as well as the others:
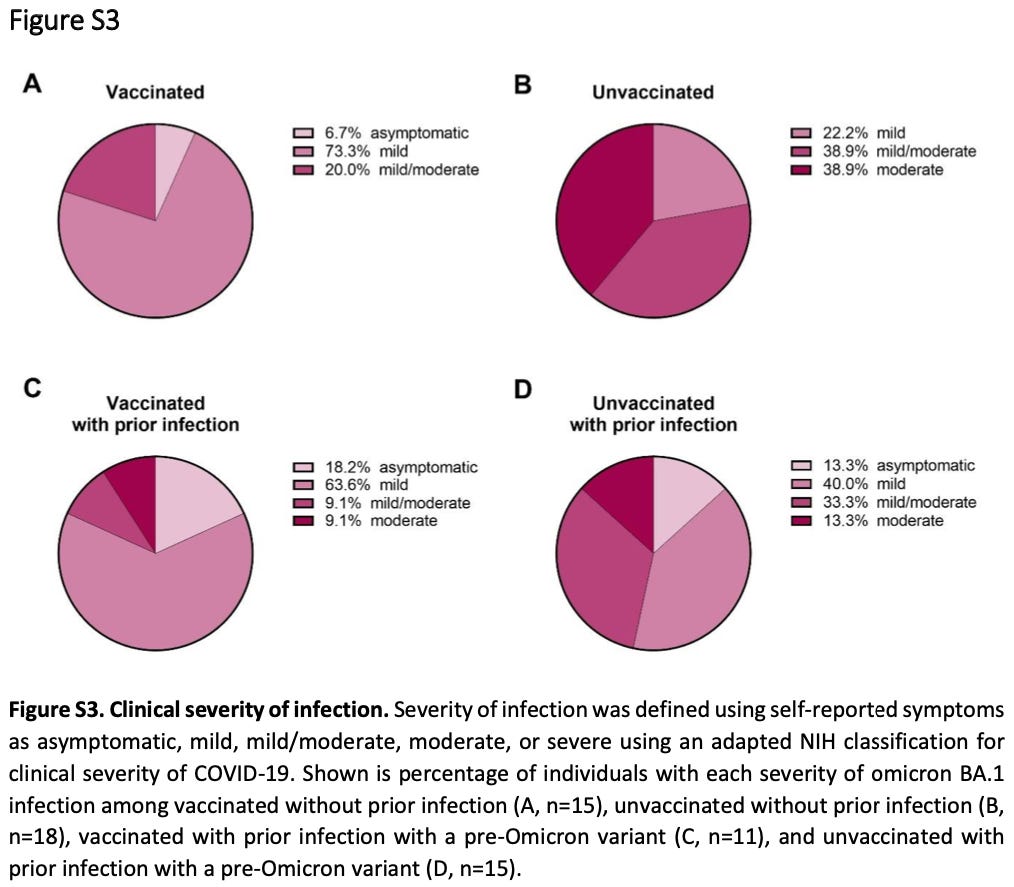
(Other charts in the Supplemental Materials supply even more discrete results, including individual lengths of time since previous injection or infection.)
What should the reader make of these interesting results, beyond perusing them as the raw data points that they are? I recommend: Nothing, for now, beyond the fact that the durability of immunity after Omicron infection is not yet clear. It could be long-lasting, it could be short.
But contra Mole, this study offers no reason to presume that the Covid vaccinated have an advantage over the unvaccinated, since the changes in the formers’ antibody response aren’t actually measured - and after all, they still went and got infected with Omicron in the first place.

See Goldberg, Y. et al. “Protection and waning of natural and hybrid COVID-19 immunity.” medrxiv.com
Rössler, A. et al. “Neutralization Profile after Recovery from SARS-CoV-2 Omicron Infection.” nejm.org.
See “Original Antigroundhogic Sin,” a review of the more straight-laced but otherwise even flimsier mirror image to Mole’s unhinged rant.
Mole, Beth. “Omicron is trouncing the argument for “natural immunity” to COVID.” (2022, March 24.) Ars Technica.
Actually, I will second this. A better “argument for avoiding vaccination” is that these unproven, experimental, inconsistently manufactured, often mis-dosed gene-based medical interventions are no better at mitigating severe outcomes than proactive health management and effective therapeutics, don’t seem effective at mitigating non-severe long-term effects, and, oh yeah, are unproven, experimental medical interventions.
Double-bad news for time travelers!
Mole, Beth. “No, your antibodies are not better than vaccination: An explainer.” (2021, October 8.) Ars Technica.
(Mole, Beth. 2021.)
Since the beginning of the pandemic, researchers have noted time and again that immune responses generated by SARS-CoV-2 infections vary wildly, with some of the weaker responses seen in people with mild disease and stronger responses in people with severe disease.
In one study Ars reported on back in June of last year, researchers looking at SARS-CoV-2 antibodies in people who had recovered found that the difference between the highest and lowest levels varied by a factor of over 1,000.
Perversely, these to graphs are a setup to an argument that antibody concentration as a correlate of immunity (which justify the superiority of vaccines) was established by studies of… nothing other than… natural immunity (as reviewed in “NIII: Part 1”). What was in fact the case was that these studies found that reinfection was rare for the naturally immune with lower antibodies, and even rarer for the naturally immune with higher antibodies. But “breakthrough” infections for the Covid vaccinated proved to be common, not rare, thus flatly refuting the conclusion that antibody levels alone are a correlate of immunity. Mole is a nimble but shameless sophist, nothing more nothing less.
As easily predicted at the time. See “The Hyperlink Archipelago.”
And so, in this respect, it has already been made clear that Omicron (BA.1 or BA.2) evades immunity from prior infection (see “Reinfections in Israel”), but the data is not in on whether lasting immunity follows after infection with BA.1 or BA.2. This does not mean that neutralization assays suddenly become predictive of long term immunity when they have been all-but-useless up until now.
Thank you for this post, which is a better analysis with more references than this NEJM 'correspondence'. Can you send them your summary for a publication?? It is extremely important to read the 'experimental procedure' of how they treat the plasma of the real human beings!!! First to use no white blood cells which are the KEY to the immune response, is the FRAUD No1.
Then on top of it heating the plasma for 30 minutes at 56 °C, that's a condition at which every human is DEAD => FRAUD No 2. To take the viruses grown in some medium with 2% fetal calf serum, instead of anything human, in particular the apparently infected volunteers, that's equally a fraud, No 3. Now taking GMO monkey cells and let these cow grown viruses plus the dead serum to multiply in it, is a complete mixup, fraud no 4. And then performing 'staining' using serum from a completely unrelated 'convalescent patient' and 'goat anti-human IgG secondary antibody' is the tip of these frauds, No 5, with big letters. This entire correspondence is literally like the RIP Robin Williams on a Saturday night show, with humans, cows, monkey's and anti-human goats, all in one pot! DR. Judy Mikovits is always right! Plandemic I and II please:)
ARS technica lacking understanding of natural immunity impugning natural immunity based on a sliver of natural immunity's function appearing to have failed in a study they probably do not understand either. Blergh.
I am impressed you manage to read such drivel and then write about it. I cannot even.