


Updates to "Efficacy by Procrastination"!
Brian punches back again... at himself!

Somewhat substantial additions have been made to yesterday’s post!

Changes:
Added a figure from Mitsi, et al. showing post-vaccine IgG in lungs — because why not, since I kept asserting that it was there (go)
Added a nice cartoon of the respiratory epithelium from Denney, Ho; and corrected my characterization of alveolar macrophages (they have both IgG and IgA receptors) (go)
Attempted a normalized comparison of pre- and post-Omicron deaths (go). I declared this too difficult in the original post; today, I decided to give it a crack using changes in elderly blood donor N antibody seropositivity.
Result of the last thing:
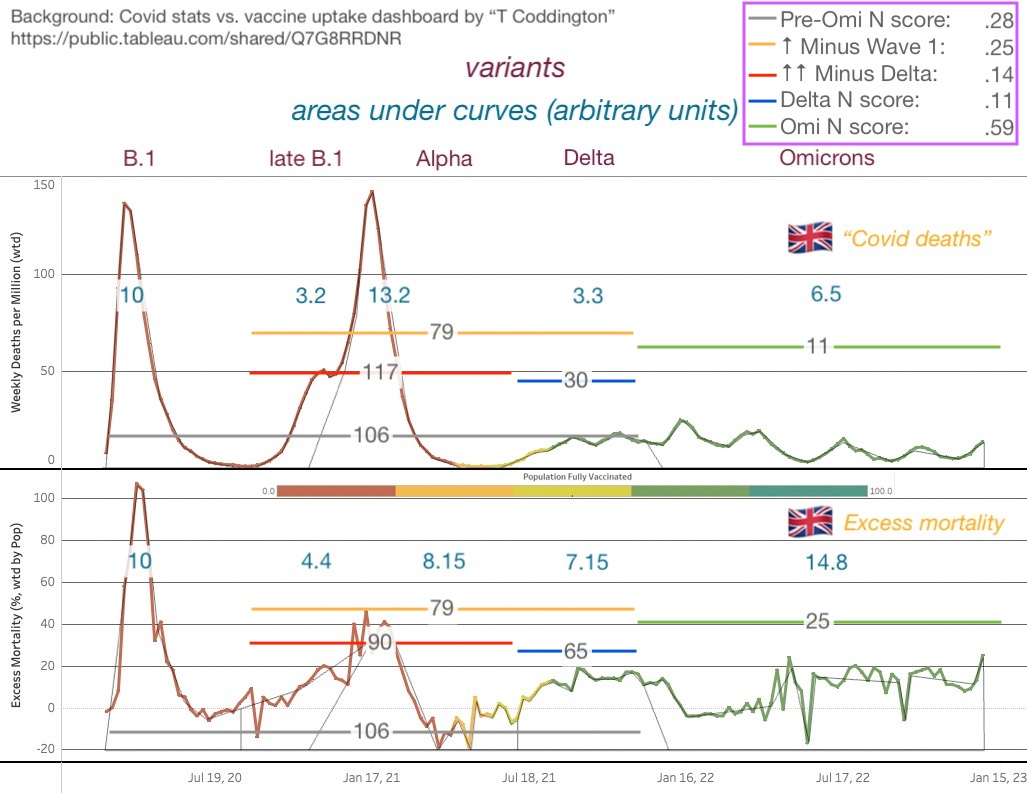
This was quite a bit of fun, and seems to restore an argument for severe efficacy being real (per-estimated-infection “deathiness” goes down in Delta era (65 from 90), and further in Omicron).
Of course, there is no accurate way to weight deaths for (elderly) infection (in particular due to the reduction in testing about a year ago). Because the adventure above is based on crude estimates of a very biased and heterogeneous blood donor pool, I conclude:
Besides revealing some weird accidentally matching ratios in areas under the curve (B.1 / (Late B.1 to Delta) is the same on both graphs), has the paradox persisted, or not? Deaths-per-badly-estimated-increase-in-elderly-seropositivity argues for severe efficacy in the Delta era. Omicron… well… applies an additional discount. So now you have reduced deaths from both severe efficacy and a family of heaven-descended milder variants (vs. would have occurred if the same rise in infection rate had occurred without both elements). Perhaps there’s no problem here after all?
Overall, I remain (newly) doubtful. If I have overestimated the true number of elderly (especially vaccinated elderly) Delta infections, the whole argument is out. A few points difference changes the excess deaths score from 7.15/.11 = 65 to 7.15/.08 = 89, which is just the same as the pre-vaccine wave.
This concludes the update announcement.
Thank you for subscribing to Unglossed!

If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Apologies for asking the bleeding obvious, but does the calculation for efficacy take into account pull-forward deaths and the likelihood (my understanding only) that viruses evolve to be milder [to leave their infectees more long-lived and transmitting vs more deadly with shorter victim lives and thus less chance of transmitting]?
To test this you'd need:
1. comorbidity data for deaths (we sometimes got some of this - avg was 2.4 for Australia, from memory)
2. virus deadliness measures (No good idea how you could measure this unless with a live virus sample injected into mice?)
If we killed chunks of the comorbid patients up front, then vaccinated the less comorbid and those lesser comorbid were infected with a milder variant, it could convincingly look like vaccine efficacy.
What potentially happened is hardier / healthier people were infected with a milder variant. Vaccine still potentially does something for comabting virus, not denying that.
A claim that it might be Vitamin D deficiency that is causing the problems, because your immune system consumes the activated form of D3 when it creates antibodies. So, if you are low to begin with, after the gene therapy treatment you will be even lower.
https://twitter.com/Parsifaler/status/1634269280102502412