A new HPV vaccine study highlights the absurdity of modern vaccine campaigns.
This post lazily tackles the most obvious, glaring logical flaws in the HPV vaccine experiment and the “HPV cancer theory” itself. Reader beware: Esoteric biological philosophy awaits.
A follow-up post may raise the broader question of why the biological fate of the entire human race has been assigned to a few (individual, unaccountable) human hands to begin with? Why does science believe it has any right to literally play God?
Forgive the occasional absence of citations; I am back to working on mobile today. Missing citations will be retroactively added some time Wednesday.
Spilling Over
Hot off the presses, is the latest micro-update in what will be a decades-long experiment by unelected biologists and the medical profession at large to determine if vaccination against Human Papilloma Virus can magically reduce cancer.
What are these “benefits”? Good health, lower rates of illness (namely cancer), increased rapport with panthers? No. Fewer encounters with a virus no one ever heard of before everyone was suddenly told they need to inject their teenaged children with a potion against. It turns out, this “benefit” is starting to “spill over.” Which (it turns out) is a fancy way of saying that it is beginning to erode. From the MedPage Today summary:
Notably, vaccine effectiveness in females appeared to drop from 84% in the 2011-2014 era to 60% in 2015-2018. Vaccine effectiveness last stood at about 51% in the 2013-2016 period for males.
The investigators cautioned that though vaccine effectiveness is an important metric, it could be misleading.
"As herd protection increases and prevalence among unvaccinated persons decreases, vaccine effectiveness might be difficult to estimate," explained the authors.
So, the “better” it works, the harder it is to tell how well it works, allege the authors. That’s not the least bit self-serving!
"We do not believe that these findings raise concerns about waning immunity; multiple studies show long-lasting protection after HPV vaccination."
Yes, but this is the latest one. And it shows that the con is unraveling.
The Long Con
HPV vaccines are recommended for early teens, in order to reduce infections resulting from parents being out of town. This is meant to reduce HPV-associated cancer.
Half of “HPV-associated” cervical cancers are diagnosed after age 49. At that point, many of today’s teen girls have already finished being tomorrow’s out-of-town-going mothers. For other cancers believed to be prompted by HPV (anal, oropharyngeal, vulvar, vaginal, and penile), the median age of diagnosis is 62 or higher. For this reason, the HPV vaccines approved and recommended for teens and young adults in the last two decades are still experimental in every sense of the word. All published “efficacy” studies to date, including today’s, report endpoints like confirmed infection and “pre-cancer,” occasionally abandoning the former when results turn south over time.
For cervical cancer, per-decade rates of diagnosis are highest between the 30s to 50s, this timespan representing a “gauntlet” of increased risk in which about four woman in every 1,000 will be diagnosed at the going rates1 (and about another two to four in the years after, depending on longevity).
Half of an entire new generation (reflecting middling uptake rates) in the US and elsewhere has been subjected to a decades long experiment - a shot in the biological dark - so that a handful of biologists can have make-work manipulating and measuring antibodies against a recognized-as-almost entirely harmless bug. After all, they have bills to pay. Groceries don’t grow on trees.2 Sorry, humanity - it’s business.
source: cdc.gov The CDC further recommends experimental injection against HPV for anyone under 27 who hasn’t yet been experimentally injected.
Note that no study yet demonstrates that the HPV vaccinated are diagnosed with cancer less often than the unvaccinated even in the short term (only “pre-cancer,” and rates of protection here are not impressive; and often require replacing the control group after previous controls get vaccinated). The rates are too small to compare; the vaccinated aren’t old enough.
Instead, the CDC touts overall lower rates of diagnosed cancer in modern times in the youngest age ranges, as a marker of the shot’s success - this says nothing about whether rates will be lower in the older age ranges when diagnosis is common. Teen girls and young women subjected to the experimental HPV vaccines could expect to discover whether they “benefited” (only the minority who were fated to experience these cancers will be in a position to benefit; the other 992 in 1,000 were never at true risk to begin with) starting when they are in their 30s. However, actual “discovery” presumes that whatever lower rate there is will be measurable.
What could stop it from being measurable? Well, today’s micro-update might offer a clue: Prevalence of the vaccine-targeted strains of HPV is now dropping in vaccinated and unvaccinated individuals alike. This is attributed, in the latest paper, to a “herd” effect. The unvaccinated are free- loading. For now, at least.
The measured “effectiveness” of the HPV vaccines has therefor declined in kind, write the authors. It only “looks” like the vaccine is less effective at preventing infection because the dirty unvaccinated are benefiting. Except, this theory doesn’t actually hold water. Whatever the unvaccinated infection rate is, it is a product to some extent, if not completely, of the virus’s attack rate in the population. If only 100 imaginary “vaccine-target-HPV-strain bullets” are shot at the whole population instead of 1,000 of same, then the ratio of “being hit” between the vaccine-shielded and not- vaccine-shielded should still be the same. Simply shooting fewer bullets shouldn’t make the ratio of successful hits change, unless the shield is fading. (Note that this critique is tentative since I have not accessed the actual study to examine the raw numbers of their efficacy calculations.)
So the time may fast arrive when the HPV-vaccinated are more frequently infected than the unvaccinated, as the latter have been harmlessly colonized by the virus already; in which case, they will be in “negative efficacy by catchup” territory.3 The authors of the editorial accompanying this new study seem to perceive that threat, though they don’t say so directly:
However, Perkins and colleagues noted that the COVID-19 pandemic has hampered HPV vaccination efforts and other immunization programs, reversing "much of the progress made in recent years."
"During the pandemic, providers and health systems have deprioritized adolescent vaccination, and particularly HPV vaccination, which in turn has led to more severe drops for HPV vaccination than for other adolescent vaccinations, and for adolescent vaccination compared with early childhood and adult vaccinations," the editorialists wrote.
This could be taken as referring to a reduction in immunity rates in at-risk age groups. But of course, this would allegedly lead to a recovery of strong apparent efficacy, per the logic offered earlier. It more seems like the authors are worried that the HPV-vaccinated are already in need of perpetual “herd protection” to maintain the illusion of lower infection rates.
Like any other injected vaccine, the HPV vaccine doesn’t actually work unless virtually every child is forced to take it, forever. Otherwise the virus in question merely has to wait for humoral immunity to wain, and get back to infecting the injected.
And of course that humoral immunity, in the realm of HPV, is only narrowly-targeted to begin with. And so at any moment, one or more of the non-vaccine-targeted strains may simply step in to the top spots in infections (still no sign of that, allege the authors of the latest paper).
And so in a few more decades, supposing that the HPV-vaccinated do have lower rates of cancer, it might prove to be the case that this is despite a higher rate of infection. Of course, this would refute the causal relationship between the virus and cancer to begin with. At which point one would have to conclude that some sort of selection bias likely accounts for the lower rate.
Or the rates for both infection and cancer could be higher.
Or who knows what other unexpected results.
And if or when these results come about, and (to the best of human powers of perception) are observed, who will the recipients of these experimental HPV vaccines hold accountable? Will any of their experimenters - the biologists, doctors, and politicians who pushed this product on the next generation of humanity - even still be alive?
Will anyone even be around to be asked the question, why did you think this would work to begin with?
And even if anyone is still around, they won’t have a satisfactory answer.
It Won’t Work
(The Official Unglossed Totally Reckless Theory for why.)
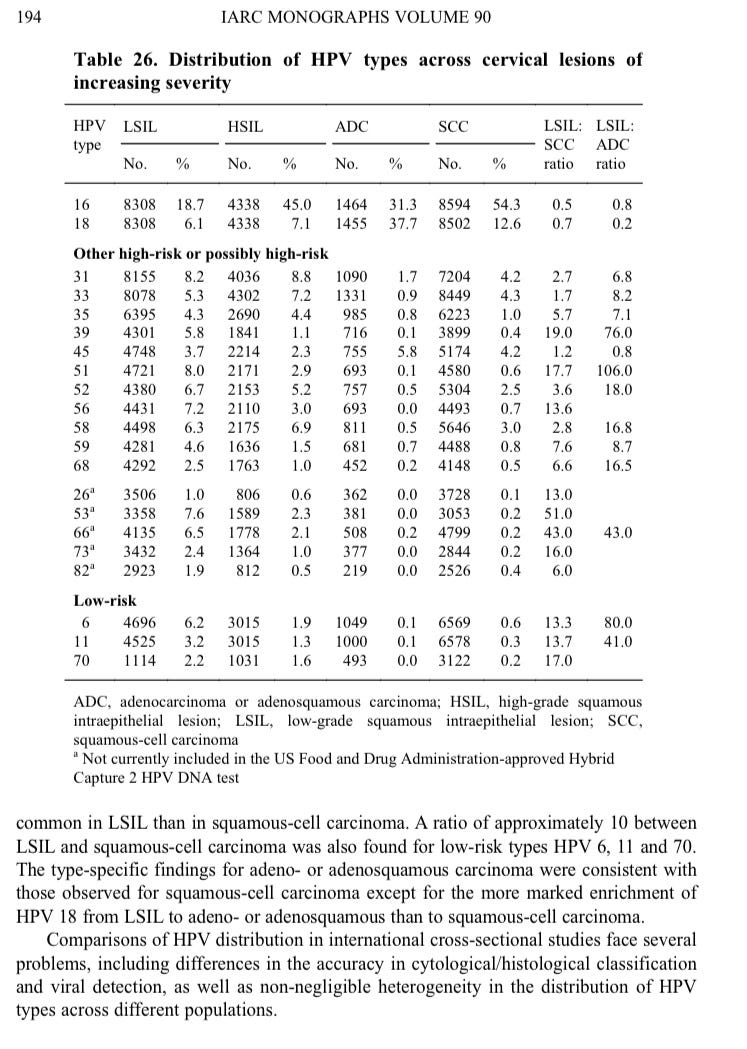
The evidence for a correlation - note, correlation - between HPV and epithelial cancers, especially cervical cancer, is stronger than for any other virus or cancer type. Some strain of HPV DNA, but especially DNA for types 16 and 18, is found in almost all of these cancers; and detection of infection is likewise a correlate for increased risk of later cancer. Lastly, HPV is believed to accelerate cancer by suppressing the p53 tumor-suppressing protein, whereas for cancers related to mutations in p53, HPV is not commonly found.4
So what?
The common thread that unites HPV infection and cancer is innate immune failure. HPV seroconversion (the appearance of antibodies against HPV) does not occur after all infections; instead, these are usually “transient,” meaning they are innately suppressed and do not require a strong immune response. Likewise, “transient” infections are less likely to be caught by screening, and so most DNA- or antigen-detected infections will be persistent infections, which are associated with increased rates of cancer. But in either case detection of HPV infection is both a correlate for cancer risk and for innate immune failure, which implies the latter could easily be the true cause for both things.
Against the theory that HPV “causes” cancer, we may further wield the blaring, obvious fact that most people are exposed to and infected with HPV at some point, and do not develop cancer. So a model where these cancers are a result of innate immune failure or suppression, and the HPV virus and its genes are merely a “passenger” in this local, immune- suppressed environment, is more plausible. As these cancers are epithelial / mucosal in nature, initial development of the cancer (and its preceding lesions) may be related to overall host un-health, lifestyle factors, or dysregulation of the microbiome (which, in a healthy state, promotes epithelial immune regulation and tissue regeneration). Only in combination with these factors do the ubiquitous, but benign cell-replication-promoting genes of the HPV virus pose a threat to the good-working-order of local tissue.
As cancer proceeds, tumor tissue propagates physical and chemical barriers for the invasion of innate immune and anti-cancer T cells. This further enriches the innate-immune-suppression environment for the proliferation of tumor-localized HPV. Here, perhaps, the anti-p53 genes of HPV are synergistic, and act as an accelerant. But it may still be the case that this should be taken as a functionally intrinsic feature of the cancer itself, because HPV is ubiquitous. The vaccine can only target so many strains; the strains of HPV currently believed to be the most carcinogenic may simply be the most abundant.
Will vaccine recipients just develop cancers involving other strains in the long run? It seems plausible. (Of the lower rate of HPV DNA in p53-mutant cancers: These cancers are not “caused” by innate immune failure, but by p53 malfunction. These cancers may have more rapid progression, not allowing time for HPV to colonize the tumor tissue. The mutation of p53 removes the “benefit” that the HPV E6 and E7 proteins can offer to the cancer, so that the cancer tissue does not confer a fitness advantage to HPV compared to non-cancer tissue, resulting in less proliferation despite innate immune suppression).
If the HPV-cancer theory is mistaken, the futility of HPV vaccination is obvious. HPV vaccines do not bolster the innate immune system. They therefor do not adjust the more likely “true cause” of the cancers with which the viruses they target are correlated.
The grand experiment of “preventing cancer” by vaccinating against HPV is just as likely to succeed as “preventing cancer by vaccinating against chemotherapy.”
Just because things are correlated with cancer doesn’t mean they cause it.
To be continued…?
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.
They and the unvaccinated who were “protected” by this flimsy, illusory “herd” effect may also experience novel negative outcomes due to encountering the virus at a later stage in life, when the immune system has begun to approach senescence; though this isn’t prima facie a strong possibility, since HPV is usually easily dealt with by innate rather than memory immunity.
Of the latter, key quotes supporting my characterization:
HPV infections (even with carcinogenic types) are so common that becoming infected is not the limiting factor in cervical carcinogenesis. The critical step for most women might be whether a precancerous lesion develops as an uncommon outcome of infection (Figure 8)
It is widely accepted that persistence of HPV infection is essential for the development of cervical precancerous lesions and cancer. Fortunately, most HPV infections are transient and become undetectable within 1–2 years even by sensitive PCR assays (Ho et al., 1998a; Franco et al., 1999; Molano et al., 2003a; Richardson et al., 2003; Muñoz et al., 2004). Consequently, anogenital HPV infections tend to resolve spontaneously, as do warts any- where on the body. Presumably, they are cleared completely by the cell-mediated immune system, are self-limited or are suppressed into long-term latency. Knowledge of how often HPV transience in the short term represents successful immune clearance versus a self- limited infection would be useful
Case–control designs typically rely on the assessment of HPV DNA at the time of diagnosis for cases and at a similar age for controls. Since persistence of HPV DNA is a hallmark of cervical cancer/CIN3, the vast majority of cases are found to be HPV DNA- positive. In contrast, the low prevalence in controls reflects both recently acquired infections and an unknown, small fraction of infections from previous years (most of which proved to be transient after 1–2 years).
A subset of mucosotropic HPVs that belong to the alpha genus, including the high-risk HPV types 16 and 18, are associated with more than 99% of cervical carcinomas (Walboomers et al., 1999). In these cancers, the papillomaviral DNA genome is often found integrated into the host chromosome (Boshart et al., 1984; Schwarz et al., 1985; Yee et al., 1985). Cervical epithelial cells that harbour integrated HPV 16 DNA have a selec- tive growth advantage over cells that harbour normal extrachromosomal viral genomes; this growth advantage correlates with the increased expression of two viral genes in parti- cular, E6 and E7 (Jeon et al., 1995). The early proteins, E6 and E7, bind and inactivate the tumour-suppressor gene product, p53, and the retinoblastoma tumour-suppressor protein (pRb), respectively (Dyson et al., 1989; Münger et al., 1989a; Werness et al., 1990). In cell lines derived from HPV-positive cervical cancers, these genes are not inactivated muta- tionally, whereas they are mutated in cell lines derived from HPV-negative cervical cancers (Scheffner et al., 1991).
A young man I know got HPV of the throat 6-8 months after HPV vaccination. This has had a debilitating effect on his life, to be sure.* His mother kept him from vaccinations until he was 18. They effing jabbed him with the disease itself. My anger remains. Jabs = disease. Remember back in the 1980's, the commercials against the drug war? Hey kids, drugs are bad. Injected drugs especially are really bad. Well, they are. A healthy body needs no injections.
*When I discussed this with a doctor, off the record, they suggested he had been sexually abused and that is why he had HPV in the throat. This is how a typical MD's mind works...they simply cannot see themselves or their INDUSTRY as causal in sickness. Well, that is the real problem, now, isn't it? Medical industry doctors need to become extinct, they have decimated their oath.
Power to the professional Doctors who are willing to see the damage the medical industry does.
It really is a magic trick that fools the masses into believing that any of this medical “science” has an empirical backing. Few think about the practical ways to validate a premise, thinking that “safe and effective” is determined through some nebulous procedure by people smarter than themselves (“I don’t know how they know it, but they figured it out somehow!”) Like you outline in this essay, there’s only one way to find out if a vaccine like this is effective: you need to wait a super long time (and then be bothered to do a follow-up study.) This is obviously antithetical to most career goals from even a purely personal motivation standpoint… when you start factoring in the economic pressure, it’s basically a miracle if any additional research is done at all.
Like you also say, almost everything in medicine has to be studied through correlation alone, for practical and ethical reasons. You can’t go around infecting people with a pathogen to assess direct cause and effect relationships, nor can you account for every factor of an individual’s unique biological makeup. But in order for a correlation to have any causative value, one needs to be stringent in their methodology. It’s why once upon a time, the first postulate of viral theory was that the “microorganism must be found in abundance in all organisms suffering from the disease, but should not be found in healthy organisms.” Fortunately for the perception of progress, Typhoid Mary came along and the asymptomatic carrier, which likely sounded like foolish doublespeak to many at the time, was established, throwing a wrench in what little actual value these mass population studies had. So we now know that viruses cause disease, except when they don’t, akin to how sometimes the heat from my stove doesn’t boil my water. It’s a crapshoot!
Science, by it’s very philosophical nature, is ill-equipped to deal with multi-causal effects and to try and solve this riddle, the discipline has been stripped of all the elements that made it an empirical method in the first place. In the case of cancer, Hippocrates himself allegedly said something to the effect of “the more you do, the worse it gets, so leave it alone, ya wanker!” But ancient wisdom based on common sense seems foolish to us evolved, intelligent monkeys and more importantly, you can’t charge someone for doing nothing (eh, unless you’re the government I suppose…)










A young man I know got HPV of the throat 6-8 months after HPV vaccination. This has had a debilitating effect on his life, to be sure.* His mother kept him from vaccinations until he was 18. They effing jabbed him with the disease itself. My anger remains. Jabs = disease. Remember back in the 1980's, the commercials against the drug war? Hey kids, drugs are bad. Injected drugs especially are really bad. Well, they are. A healthy body needs no injections.
*When I discussed this with a doctor, off the record, they suggested he had been sexually abused and that is why he had HPV in the throat. This is how a typical MD's mind works...they simply cannot see themselves or their INDUSTRY as causal in sickness. Well, that is the real problem, now, isn't it? Medical industry doctors need to become extinct, they have decimated their oath.
Power to the professional Doctors who are willing to see the damage the medical industry does.
It really is a magic trick that fools the masses into believing that any of this medical “science” has an empirical backing. Few think about the practical ways to validate a premise, thinking that “safe and effective” is determined through some nebulous procedure by people smarter than themselves (“I don’t know how they know it, but they figured it out somehow!”) Like you outline in this essay, there’s only one way to find out if a vaccine like this is effective: you need to wait a super long time (and then be bothered to do a follow-up study.) This is obviously antithetical to most career goals from even a purely personal motivation standpoint… when you start factoring in the economic pressure, it’s basically a miracle if any additional research is done at all.
Like you also say, almost everything in medicine has to be studied through correlation alone, for practical and ethical reasons. You can’t go around infecting people with a pathogen to assess direct cause and effect relationships, nor can you account for every factor of an individual’s unique biological makeup. But in order for a correlation to have any causative value, one needs to be stringent in their methodology. It’s why once upon a time, the first postulate of viral theory was that the “microorganism must be found in abundance in all organisms suffering from the disease, but should not be found in healthy organisms.” Fortunately for the perception of progress, Typhoid Mary came along and the asymptomatic carrier, which likely sounded like foolish doublespeak to many at the time, was established, throwing a wrench in what little actual value these mass population studies had. So we now know that viruses cause disease, except when they don’t, akin to how sometimes the heat from my stove doesn’t boil my water. It’s a crapshoot!
Science, by it’s very philosophical nature, is ill-equipped to deal with multi-causal effects and to try and solve this riddle, the discipline has been stripped of all the elements that made it an empirical method in the first place. In the case of cancer, Hippocrates himself allegedly said something to the effect of “the more you do, the worse it gets, so leave it alone, ya wanker!” But ancient wisdom based on common sense seems foolish to us evolved, intelligent monkeys and more importantly, you can’t charge someone for doing nothing (eh, unless you’re the government I suppose…)