


Near t' Rock Bottom out on Route 23
The first step to ending your addiction to issuing deceptive public health messaging to 328 million of your fellow citizens, is admitting you have a problem.

As July draws to a close in states of affairs far less ambiguous and far more chaotic than did June, we may indulge in a topical post. Nothing here will be very salient to this journal’s primary audience, the future reader.
But for us here in the present, when the government seems to be convulsing as if it is a hammock that someone has put seven cats into, it will be salient; as when the country awoke on Friday it appeared that four more cats had been added on. Thus while the screams are still saturating the patio, let us take a look at the CDC’s formally leaked communications-update presentation appearing last night, soberly entitled: The Steering Wheel Has Fallen Off This Wagon of Lies - But Don’t Worry, So Have All But One of The Regular Wheels.

By now, affixing the image of SARS-CoV-2 to the header of a document seemingly represents the royal seal of our novel but endless Public Health Theocracy. Just in case there were any worries that we have not yet been officially relieved of all that wanton, unruly self-governance stuff.
The document was issued via a rushed but admirably comprehensive report in the Washington Post.1 The goal of leaking the presentation that generated the report was, vaguely, to interface with the CDC’s host of mainstream media water-carriers to adjust their coverage of recent confusing and contradictory agency proclamations, because apparently the coverage wasn’t making them look confusing and contradictory enough. Internally, the goal of generating the report, was to offer a data- and modeling-backed analysis for adjusting the CDC’s communication strategy so that CDC communication could be made more… improve-y…?
1: Why leak it?
Objective 1 - the objective of leaking the presentation - has been a smashing success. By Friday morning, other news outlets were releasing their own parroted reports of the Post’s, and on Thursday night as they began to compile these, the cornucopia of fodder for alarmist headlines must have been dizzying to behold (the first quote of course being the Post’s own selection; the Millennial reader is not discouraged from reading the following bullets in their internal local-TV Monster-Truck-Rally-announcer-monologue voice):
“delta infections likely more severe”
“public convinced vaccines no longer work/booster doses needed”
“a variant so contagious that it acts almost like a different novel virus, leaping from target to target more swiftly than Ebola or the common cold.”
“vaccinated individuals infected with delta may be able to transmit the virus as easily as those who are unvaccinated”
“vaccines are not as effective in immunocompromised patients and nursing home residents”
“vaccinated people who became infected with delta shed just as much virus as those who were not vaccinated”
“35,000 symptomatic infections per week among 162 million vaccinated Americans”
“universal masking is essential to reduce transmission of the Delta variant”
“a “canary in the coal mine” for scientists who had seen the data”
One cannot help but imagine the portion of the American public which has not already tuned out the expert/media Theatre of the Pandemic completely, as a space-pilot who has been traveling for six months to an enemy planet in a craft that his home-planet’s scientists had declared as being all but invulnerable to the enemy’s weapons; and now as he is mere space-days from the battle, broadcasts from command flood his heads-up-display every hour warning both, “The enemy has weapons more powerful than ever comprehended!”2 and, “We might have put your lasers on backwards!” combined at last with, “Christ’s sake, couldn’t you go a bit faster?!”
But in the context of the present, such fatalistic messaging chaos need not coherently advance a rationale for why the vaccine-hesitant should get the vaccine even if it is less effective than promised when they originally decided to wait; they, in fact, do not seem to be the target audience. The purpose - if we offer a theory of purpose that strictly infers intention from effect - is to whip the already-vaccinated into a froth; to stoke in their minds a veritable frenzy of resentment and alarm about the unvaccinated who are “holding us back” from “putting Covid behind us!” Under this theory, the CDC - whatever shadowy element of the CDC blessed the decision to release this confusion-sowing document unto the public under the vague guise of “correcting” their previous lack of transparency around the mask guidance reversal - has decided to recruit vaccinated Americans in the counter-revolt to the revolts which will follow the coming universal vaccine mandate. With this shotgun-blast of internal statistics on the state of the “war,” the capacity of our expert-adoring media to spin negative news about the vaccination campaign has been exceeded, and what thus becomes clear in the resulting dishevelment is that the war has been lost. By leaking this presentation, the CDC has signaled to the Americans that still counted on them for salvation: “We tried, but… look. We just can’t do it. We’re all out of ideas. These anti-vaxxers… Nothing’s going to reach them.”
In response to this play-acted Kieler Matrosenaufstand, the Believers of the Experts have gone… it can’t really be put delicately… Full Nazi. The Believers, who have spent the last 10 days of dire reports of Covid vaccine non-efficacy out of Israel and the UK in states of shell-shock or giddy denial - “I was worried for a while, but if the news is this bad, it can’t be true!” - now have seen their Siegfried collapse in stage-death under the media’s disintegrating backdrop; and having confused the Pandemic Opera for reality, all that is left to do is hunt for the nearest Hagen. Indeed, the tone online (I go there sometimes) today is one of explicit violent coercion against the unvaccinated: If we aren’t going to “see reason” (meaning that the reasonable arguments in favor of vaccination have all been dismantled), then we must be forced. This fervor burns no less intensely within the breast of those who were never hawks about the virus itself to begin with; in fact it might here be found at its highest temperature: For these are the more intelligent of the souls who have bought into this grand fraud. They are invested in a decision they arrived to rationally, based not on fear but on assigning sound judgment to other actors who did not deserve such credit (they’ve apparently never met or talked to a real American corporate executive). They cannot help but intuit that their frustration and embarrassment over the revelation that not only did they make the wrong choice, but others didn’t, would go away if Storm Troopers Vaxxing at Gunpoint = true. And so they, too, join those who still buy into Covid-19-alarmism sincerely, in hunting down the Hagens to expel from their soil.
So, if effect implies intention, the CDC has just made a brilliant maneuver. 60 million American citizens have been turned into their neighbors’ Other overnight. But really, why should we imagine that their powers of understanding of public behavior are nearly so acute? Indeed these powers seem not to exist at all; if they did, the CDC would not have wasted time with the narrative-muddling song-and-dance of lifting masking guidelines in the first place; moreover, we would all be vaccinated by now.3 If the CDC has achieved, via the last 10 days of missteps capped off by this defeatist leak, a public manipulation coup of such brilliant effect that it would make Goebbels shed an admiring tear and is sure to one day get its own sub-heading in the Setting the Stage to Purge Your 60 Million Dissenters - FOR DUMMIES handbook, it is plausible that it has done so entirely by accident.
4The Post has obligingly but somewhat narrowly supported this either intended or accidental neighbor-othering coup, by burying what is actually the most significant implication of the (already known, but now acknowledged) plummet in Covid vaccine infection efficacy at the bottom of their report: If a non-trivial percentage of vaccinated individuals can both catch and spread SARS-CoV-2, vaccination does not contribute to “herd immunity.”
100% vaccinated still = no herd immunity = 100% eventual exposure
In the conclusion to Part 2 of The Natural Immunity Illusion Illusion, I already forwarded the argument that herd immunity is not a valid framework for thinking about this virus (this argument will be fleshed out in an essay next week).5 But within the epidemiological-political construct used to promote these vaccines to individuals who are not at significant risk from SARS-CoV-2, the sudden removal the of Herd Immunity Cog brings the whole machine to a halt. The vaccination of the not-at-risk does not in any way contribute “protection” to the at-risk.
However-many Americans have received the vaccine not because they thought it was the right choice for themselves but imagining that they were doing it for their loved ones (I think this must be millions), these have been medically defrauded.
The significance of plummeting infection efficacy cannot be overstated. As also mentioned in Part 2 of NIII, herd immunity has, all along, been the only argument for why anyone who believes that the risks of the Covid vaccine might outweigh the risks they face from the virus itself should choose the former. Either our Public Health “experts” were sincere about the original 94% infection efficacy rating, and must stop citing their fine print for why the efficacy drop does not violate the explicit promise of the Covid vaccines, or they were insincere about the infection efficacy rating, and the herd immunity argument has been fraudulent propaganda all along. Either way, the dismantling of the herd immunity myth means that the push for 100% vaccination either must end or must be continued, from this point, by means of raw factual deception or force.
This buried lede - which is to say the conclusion drawn from what was already clear from Israel and the UK - is delivered by the last two outside experts who supplied comment for the report, Jeffrey Shaman and Kathleen Neuzil.6 Here is how Shaman summarizes this (again, long obvious) conclusion (with a grossly truth-obscuring equivalence between reinfections and post-vaccine “breakthrough” infections needlessly thrown in):
“In some sense, vaccination is now about personal protection — protecting oneself against severe disease. Herd immunity is not relevant as we are seeing plenty of evidence of repeat and breakthrough infections.”7
Presumably the Post distributed the CDC presentation to many if not all of their expert contacts sometime on Thursday, and used whichever replies they had received by print to pad the article with analysis that they could have easily done themselves. I count six total contributing analysts - short shrift, therefor, for Shaman and Neuzil, that their intelligent observations were considered less relevant than three renditions of, “Gosh, it sure looks like Delta’s gonna kill us all!” and one rendition of, “Now this is what I call scientific transparency!” Apparently Shaman’s reinforcement of the Natural Immunity Is No Escape trope did not make his opinion sufficiently palatable, and Neuzil’s caveated hawking of the vaccines was found to be insufficiently absolutist:
Kathleen Neuzil, a vaccine expert at the University of Maryland School of Medicine, said getting more people vaccinated remains the priority, but the public may also have to change its relationship to a virus almost certain to be with humanity for the foreseeable future.
Only more people, Neuzil?8
Regardless, if the Post was trying to salvage one last shred of the pro-Covid-vaccination argument by burying the destruction of the herd immunity myth at the bottom of their report, they needn’t have bothered. To the audience of Believers mourning their CD-Siegfried, the fact that the unvaccinated are no more a threat to the vulnerable than the vaccinated is only all the more grounds for vengeance.

2: Why write it?
Whether Objective 2 in our backwards sequence - the objective of preparing the presentation - is a success, depends. If the presentation was prepared specifically so that it could be leaked in order to make matters look hopeless, then it has been, naturally, a success. If it was prepared in order to generate actionable strategy, it is surely an utter failure.
Like the transmissions from command in our space pilot analogy, the presentation moves in three directions at once, producing only uncertainty. What’s more, despite the presentation being leaked under the auspices of substantiating the “new scientific research” that was alluded to during the announcements which preceded the leak, the information “revealed” in the presentation is all almost one to three months out of date. The idea that the CDC should be making changes to guidance now based on information from April is mind-boggling (within the artificially-imposed context that SARS-CoV-2 is a “pandemic,” and not already an endemic routine virus which has tired of the limelight).
Since the presentation therefor offers no very obvious logical framework for analysis, we can use four of the “frightening” quotes offered above for our prompts.
“delta infections likely more severe”
(For correction notice on this segment, see footnotes.10)
If there is any element within the presentation that most seems to support the written-to-be-leaked theory, it is this one. Upon inspection, the work is not as shaky as it appears, but it is still a bit shaky.
It should be better, given that the CDC here has performed a violent 180 on the narrative that Delta is the less edgy, commercial-radio friendly version of Covid-19™, serving the viewers at home with a Travoltaesque pivot toward evil. It has done so, furthermore, using data that is transparently flimsy-at-best. Even with the fluttering chaff of “scoops” littered throughout the presentation it is astonishing that the Post’s three writers and six consulting analysts did not feel that the potential superficiality of the work upon which this assertion is based merited much more cautious reportage. But now that they and their puppets have already gone and promoted the Declaration of Evil Travolta, and have done so while replicating and amplifying the red herrings in the presentation, no meaningful correction to the mainstream narrative, if it turns out to be necessary later, is possible. A separate three-author team at the allegedly “independent” Science News, for example, has already repackaged the original presentation into an “explainer” that repeats the contained assertions within “The CDC says” text strings that make no mention of the fact that they source from preliminary findings leaked by the Post less than 24 hours ago.11 Thus if later studies reverse the CDC’s preliminary conclusions, it will at best become perpetually “unclear” whether Delta “causes” more severe illness, from here on to whenever SARS-CoV-2’s writers think up the next villain of the week. And yet nothing in the actual presentation supports the “more severe” claim except this slide:

In the three referenced studies,12 local positive PCR tests counts and hospitalizations for infection with SARS-CoV-2 in Ontario, and Scotland, and Singapore were (individually) compiled, and differences in the strains corresponding to the respective PCR tests and hospitalizations were determined by discrete sequencing or by statistical machinery. As hospitalization-per-case rates must necessarily not be the same everywhere in the world all the time, there is no possible way to exclude that these three locations are outliers to whatever the global trend actually is - either for their low baseline rates in the late winter (when “wild” and Alpha strains are found in their sequencing) or their higher rates in early summer (when Delta is higher).13 And as local changes in hospitalization-per-case rates can be caused by literally anything, ascribing these (possibly outlier) changes to Delta is barely supportable on the face of things. There are as many “confounding factors” in all of these strain comparison studies as there are humans on Earth.
Yet even if basing a permanent, irreversible pivot in messaging around Delta on three local studies is intrinsically crazy, it turns out that the studies do seem to strongly suggest the possibility that Delta can lead to more severe outcomes. In particular, the confounding factor that sticks out like a sore thumb in all three - that all locales were simultaneously undergoing the rollout of the Covid vaccines - implies that Delta is showing this increase in severe outcomes despite a discount. All three areas were removing older-aged citizens from the potential infection pool as the study period progressed. Yet despite the dwindling of the winter waves which corresponded with Delta’s moderate absolute rise (and corresponding proportional surge) in local PCR-test positives, the youth and middle-aged who were testing positive were ending up in the hospital at a higher rate-per-positive than the overall population had been doing, when vaccination rates were low. And while the vaccination figures compiled in the Scotland study appear not to be publicly available, the Singapore study seemingly dampens any speculation that vaccination itself was driving post-infection trips to the hospital among the young or middle-aged.
The authors, for one portion of the study, examined the 1,007 individuals who, after scoring positive on a PCR-test, were entered into the NCID clinical management center specifically. Of these, only 23 were among individuals more than 14 days on from their first dose (18 of which were with the Delta strain), and none of these resulted in a severe outcome (defined as pneumonia or worse):14
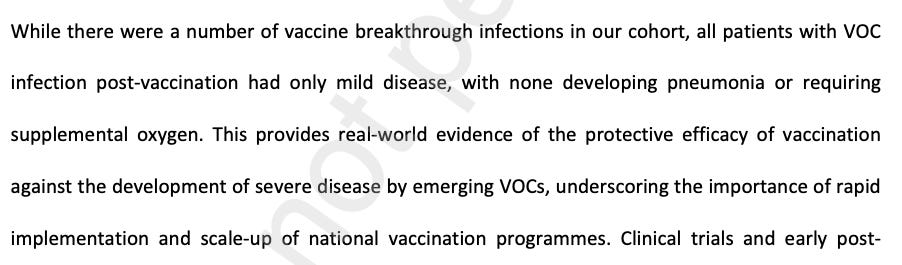
Because the Singapore NCID clinical management center sample of 1,007 is too small to grant a great degree of accuracy, the corresponding lack of patient vaccination status information in the larger Ontario study - which pulled from 211,197 cases - means that a confounding effect from the vaccination of the young is still on the table (once again, the vaccination status information in the Scotland study appears to not yet be publicly accessible).
Further, the text of the Singapore study at present does not assign absolute certainty to the collection of vaccination status information for the clinical management center’s “Wild Type” patients - those who did not score below the given PCR-test cycle threshold - who are used as a quasi-control. Bearing in mind that the Wild Type patients also did not undergo sequencing, room is left open for other disparities in statistical collection. The authors in the Singapore study are captive to the bureaucratic data-collection designs and implementations of the Ministry of Health and the NCID clinical management center, and may not even have direct knowledge of how accurately or consistently their own data was collected in practice.
Thus with the vaccination confounding factor “discount” left as a question mark, it is here that the arguments for declaring Delta ready-for-arraignment in the Court of Travolta Evilness more or less end. They are not weak, but will the jury buy them? There’s still a lot of noise among these different studies - including the other portion of the Singapore study, which was more broad but did not include vaccination status - and room for multiple different confounding factors that coincidentally push in the same direction.15
For both the Ontario and the Scotland study, for example, changes in hospitalization threshold may be contributing to higher hospitalization rates per positive test. If local health care centers are simply more inclined to encourage the young to err on the safe side when their beds are less full, this could account for a coincidental surge in Delta’s “hospitalization rate.” This leaves ICU and death rates unexplained - but these are small enough to be higher merely by means of local flukes or a very small increase in post-vaccination-infection severe outcomes.
Rounding back to Singapore, the severe outcomes observed with Delta in the clinical management center portion of the study are potentially poisoned by the “outbreak among [potentially unvaccinated] elderly in a healthcare facility” referenced in the study text, which is explicitly tied to the Delta cohort (but not to the 18 vaccinated Delta infections mentioned in the next sentence), and which could easily account for nearly all the rise in severe outcomes, without which Delta would have scored values similar to Alpha and Beta:


Or, it could turn out that the elderly Delta patients did not contribute to the severe outcomes - particularly if all of these individuals, despite meeting the lower cycle-count threshold for entry into the “cohort” group, are in the 18 vaccinated non-severe outcome pseudo-group defined by the authors’ text (the 1,007 clinical management center cases span from December 20 to May 12; but since the “elderly healthcare facility breakout” is ascribed to Delta, high levels of vaccination are not at all unlikely).
This leaves the non-NCID portion of the study, which does statistics to overall Ministry of Health case data for the 2,930 PCR-confirmed infections with SARS-CoV-2 in Singapore between January 1 and May 22. Here there is no way to infer any potential selection bias effects of the 976 cases which were chosen for sequencing, as the authors do not explain what criteria were employed for each health system supplying data to the Ministry, nor whether that criteria was consistent or changed midway through the study period, with obvious potentially distorting effects. If a given health center, midway through the year, switched from random sequencing to severe outcome-targeted sequencing, that would clearly poison the results. Overall, no access is provided to the statistical machinery used to produce their “adjustments” for age and sex and no comorbidity data was available for the authors. Moreover, the authors could not even measure hospitalization rates for this portion of the study, for the ironic reason that Singapore enters all PCR-confirmed infected patients into the hospital system by default (and unlike in the NCID portion, diagnosis of pneumonia was not available as a proxy): Thus the authors are left, in this portion, to use the (vastly) more rare outcomes of oxygen administration (30 patients), and ICU admission or death (10 patients) to try to gauge the differences between Delta, Alpha, and Beta. These 40 events are used to produce the odds ratios represented in Table 1, but are not given to the reader to see in raw form.
Ruling out all of these corrupting effects would require access to the raw data for all three studies, and a few million hours of analysis; after which it’s still entirely possible that the wrong result will be arrived to. Just as it has been possible all along that the observations of Delta’s contagiousness have been mistaking correlation for causation, almost any attempt to wiggle the divining rod at severe outcome rate is likely to come up dry. And, more to the point - why isn’t the CDC defaulting to its own data on Delta’s severe outcome rate? Does it not have this data? Does it have it, but regard it as less accurate a reflection of reality than a data analysis of 40 sequenced variant-of-concern severe outcomes in Singapore?
“a variant so contagious that it acts almost like a different novel virus, leaping from target to target more swiftly than Ebola or the common cold”
Thankfully we just covered that problem. Again, we really have to question if this is the quality and thoroughness of a document intended for internal consumption, rather than public release. Here a five-month old chart from The New York Times is repurposed with edits that I could do in Preview, and merely to serve the apparent justification of hyping Delta’s transmissibility with gratuitous references to the classic bogeymen of yore:

“vaccinated people who became infected with delta shed just as much virus as those who were not vaccinated”
This, once again, is based on a handful of studies from abroad and one released today by the CDC themselves concerning a sampling of 469 PCR-positive “cases” in Barnstable County, MA in July.17 Here, 80 vaccinated individuals and 65 unvaccinated individuals were found to be just as “virus-y” according to how few cycles were needed to produce a positive test. This result, however, elides the study’s glaring selection bias: only individuals who either sought out a test or were identified via cluster-contact tracing were included in the sample set.18 If there were 4000 vaccinated asymptomatic cases and 500 unvaccinated asymptomatic cases going on outside of the study sample, the “finding” of the study would turn out to be completely false.
This section also uses figures reported nationally on the lower required cycle threshold generally found for patients infected with Delta - i.e., once again, more “virus-y-ness.” This, however, doesn’t really belong in the list of research that supports an estimation of the relative degree to which vaccinated individuals, exclusively, are spreading Delta.
None of this means that the resulting assertion - vaccinated individuals (particularly as infection efficacy wears off) are contributing to the spread of SARS-CoV-2 - is wrong. Just that it is not strongly supported by the CDC’s own citations. And as long as the CDC, via this leak, is purporting to show their own work, the writers and consulting analysts at the Post should have been able to recognize that the work itself was faulty.
“universal masking is essential to reduce transmission of the Delta variant”
This is just pure fabricated nonsense. The presentation uses a model constructed from arbitrary efficacy-rates for masking which are not supported by any research to arrive at a predetermined result that masks are universally necessary to lower some magic statistical swirls - to an end that isn’t even clear. If I’m going to obey health dictates based on the completely imaginary protective power of a small cloth, I at least want to understand why lower swirls are any better than higher swirls. This is America, not Fascist Spain, and I know my Swirl Comprehension Rights.

“You don’t, when you’re a public health official, want to be saying, ‘Trust us, we know, we can’t tell you how,’” [Kathleen Hall] Jamieson [director of the Annenberg Public Policy Center at the University of Pennsylvania] said. “The scientific norm suggests that when you make a statement based on science, you show the science.”
If you can make the CDC sound like they are being unfairly attacked in the midst of their horrible month, your problematization skills are awe-inspiring.
Nonetheless if the narrative that this leak was an attempt by the CDC to improve transparency a.k.a. adherence to “The Scientific Norm” is to be taken seriously, it must be called a half-hearted attempt at best. The “Improving Communications” leak does not improve upon their mid-week innuendos, but merely deflects from the critiques of those innuendos by offering a hashed-together montage of reckless over-certainty, topical misdirection, and arbitrary guesses in their place. If the CDC has a rock bottom from which no further trust can be expended and its leaders and staff must confront their years of nearly ruthless abuse and manipulation of their fellow citizens, it hasn’t reached it yet.
In the meantime the most truly informative slide within the presentation appears at the end. When originally uploaded by the Post, the presentation’s authors were listed on the last slide. Mid-morning on Friday, the version available online was changed, to reflect the appropriate degree of public disclosure for such a sensitive document:
Abutaleb email bio follow, Yasmeen. Johnson email bio follow, Carolyn. Achenbach email bio follow, Joel. “‘The war has changed’: Internal CDC document urges new messaging, warns delta infections likely more severe.” (2021, July 29.) The Washington Post.
“I mean you oughta see these things! They’re a beaut!”
Additionally, I am not sure if the maneuver fits within the hypothetical risk budget of the hypothetical shadowy CDC leak-approver: The gains from this leak in terms of putting mandates more nearly on the table seem to have been great; but the leak also risked making mandates less acceptable by endorsing many of the principle arguments against the Covid vaccines.
Indeed, the most obvious interpretation for why this presentation was leaked is that it was meant to smuggle the weakly-supported reversal on “Delta infection severity” past the Post’s 3-writer panel, by buttressing it with a dozen other weakly-supported research “developments.” Why do this? If the CDC expects an imminent biblical flood of antibody-dependent-enhancement-based adverse outcomes to infections with SARS-CoV-2 among the 180-days post vaccinated, demonizing Delta is the only hope of obscuring-via-misdirection what will otherwise be obvious: The vaccinated will soon be experiencing severe outcomes at a higher rate-per-infection at all age groups than the unvaccinated.
Edit on August 1: This narrative would be critical particularly if Delta infections are more sensitive to (early) post-vaccination antibody dependent enhancement than Alpha (as potentially shown from the Ontario study graph in footnote 15, if we again wave the specter of a post-vaccination severe outcome confounding factor among younger and middle-aged Covid vaccination recipients), because it is only partially a match for the Covid vaccine-scripted antibodies, as suggested by the Planas, D. et al. “Reduced Sensitivity” study as reviewed in NIII Part 2. (It could still be possible that in later post-vaccination infections, a closer match to the Covid vaccine-scripted antibodies leads to worse outcomes. If you open a can of worms, you can’t expect them to all flop in the same direction.)
The sub-head for this essay, “How I learned to Stop…” has already been scooped as of the Weekly Dish post which arrived in my inbox while writing this (I swear I only read it for the articles). If my title is not similarly scooped, I will still get to use the subhead.
A “Columbia University epidemiologist” and “vaccine expert at the University of Maryland School of Medicine,” respectively
There is plenty evidence of rare reinfections. There is plenty evidence of widespread post-vaccination infections.
Seems like someone might be in need of a blindfolded train-ride to the “Vaccine Messaging Consistency Workshop”…
(index link anchor)
Substantial updates and cleanup were done to my analysis of the Singapore study on July 31.
Most significantly, the original sample size offered for Singapore’s vaccination infection outcome dataset (and for the number of cases in Singapore generally post-vaccine-rollout) was incorrectly defined as 100. The correct sample size is 1,007 (if vaccination status was in fact recorded for all NCID clinical management center patients, not just those within the “cohort”) and the correct overall case count in Singapore during the time period used for the non-NCID portion of the study, January 1 to May 22, is 2,930.
Additionally, I initially wrote that there were 18 post-vaccination infections in the NCID portion. This has been corrected to 23 (to include the 5 Alpha breakout infections).
These are the primary corrections made during these revisions - the remaining edits to the Singapore study analysis serve to expand or clarify the original version. Specifically:
Added: Analysis of the non-NCID portion. As the non-NCID portion turned out to only contain 40 measurable outcomes, the original omission of this element from my analysis was not only trivial but insignificant to the conclusion offered (which has not been reworded in any way as regards to how supportive these studies are of the CDC presentation’s assertion that Delta leads to more severe outcomes: the essay remains ambivalent on that point).
Moved: Analysis of the “elderly healthcare outbreak” note in the NCID portion, which I had initially interleaved with the NCID vaccination data analysis, to very confusing effect. This was purely poor editing in the original version.
Added: The paragraph “Further, the text of the Singapore study…” This contains an explanation of the Wild Type / VOC control / cohort distinction and new analysis based on more thoroughly parsing the authors’ design, with the resultant conclusions that consistent collection of vaccination status and other health outcomes among the Wild Type control group is not quite robustly affirmed by the authors’ text.
Removed: Reference to the significance of the Singapore study which was interleaved with the NCID vaccination data analysis:
Even if it still accidentally supports the other results, in no way should a study essentially trying to guess the size of the Earth with a half-broken tape measure be used to inform communications of the premier public health bureaucracy of the United States.
This removal substantially changes the weighting that the segment’s analysis applies to the NCID portion; however, since the “elderly healthcare outbreak” stands as a potential driver of the observed severe outcomes for Delta, the conclusion offered overall stands. In fact, as the further potential obscuring factors described in the previous note were added, the increase in weight of the NCID study only “strengthened” the ambivalent conclusion: The study should not be used to inform communications of the premier public health bureaucracy of the United States.
Changed: The concluding sentence originally reprised the original mistake already noted in the correction above (by using a construction based on the misunderstanding that the scope of the Singapore study was limited to 100 cases).
Does it have it, but regard it as less accurate a reflection of reality than an outbreak in an elderly care facility in Singapore?
To:
Does it have it, but regard it as less accurate a reflection of reality than a data analysis of 40 sequenced variant-of-concern severe outcomes in Singapore?
This retains the rhetorical hyperbole but without using a mistaken reading of the study to formulate it. 40 severe outcomes were used by the CDC to help form their ostensible picture of reality, ostensibly in lieu of their own data. Again, the conclusion itself was not changed.
As the segment was more careful with the Ontario and Scotland studies - specifically because no obvious analysis of whether the effect of vaccination should be a discount or not seems possible from the currently-available data - no further correction is expected. (Additionally, the added point that individual health centers in Singapore may have switched from random to more outcome-targeted screening regimes by coincidence when Delta became more prevalent seems to apply equally to the Ontario and Scotland studies; but I have not yet checked if the authors’ descriptions ruled that out.) Fingers crossed, etc.
Saey email twitter, Tina. Garcia de Jesús email twitter, Erin. Lambert email twitter, Jonathan. “New delta variant studies show the pandemic is far from over.” (2021, July 30.) Science News.
Fisman, D. Tuite, A. “Progressive Increase in Virulence of Novel SARS-CoV-2 Variants in Ontario, Canada.” medrxiv.org.
Ong, S. et al. “Clinical and Virological Features of SARS-CoV-2 Variants of Concern: A Retrospective Cohort Study Comparing B.1.1.7 (Alpha), B.1.315 (Beta), and B.1.617.2 (Delta).” The Lancet.
Sheikh, A. et al. “SARS-CoV-2 Delta VOC in Scotland: demographics, risk of hospital admission, and vaccine effectiveness.” The Lancet.
All three studies occur in locales with very low PCR-test-positivity rates either throughout the study period or throughout a significant portion of the end of the period, indicating a high prevalence of screening testing. This suggests they could be outliers due to their accuracy: They are capturing asymptomatic cases, particularly in the pre-Delta strains, that other countries are not. However, this could be true and still not imply anything different about what outcomes an individual who receives a positive test after already developing symptoms will afterward experience! For that individual, it is too late to “win” the hypothetically rarer first prize in the hypothetical Delta lottery; that doesn’t mean the odds for hospitalization are also higher. In fact this would simultaneously explain why when Delta appears in areas that do not perform high levels of screening-testing it appears as “more contagious”: it is “moving” asymptomatic, untested individuals into the symptomatic, tested group. Therefor a repeat of the Ontario/Scotland/Singapore studies in an area with less screening-testing would potentially show a lower rate of hospitalization, even if nothing about the hospitalization-per-infection-ratio was changing!
[Redundant after further editing:] That all 23 vaccinated-infected individuals did not have a severe outcome is actually mentioned on lines 267-9.
The Ontario study does not record patient vaccination status or attempt to show a relationship between current age-group vaccination trends and the age-group of patients. Patient age does drop toward the end of the study.
The strongest evidence for associating the rise in hospitalizations and deaths from the Delta strain specifically seems to come from the Ontario study’s handy proportional graph. In the relevant portion of the timeline, Alpha and Delta account for apparently equal amounts of cases. As hospitalizations and deaths are a lagging indicator, it seems that Alpha accounts for a majority of results when it just had been the driver of more cases, but a minority of results after both strains just had been equal drivers of cases:

(index link anchor)
Further reading of the study on July 31 leaves this statement more or less in tact. Out-of-town visitors to Provincetown were “encouraged” to seek out testing in some manner; while many may have done so, it seems unlikely that all did. Only 58% of the PCR-confirmed infection cases collected by the study were among out-of-town visitors, which seems low in proportion to the visitor (“thousands”) / resident (~3,000) ratio in the study period. Asymptomatic post-vaccination infection cases - at only 21% of all post-vaccination infection cases - still seem likely to have been undercounted. Additionally, the study itself contains the same conclusion reached by this essay as originally published (no significant edits have been made to this portion of the essay). It adds, as well, another potential confounding factor which also stuck out to me during my review: If unvaccinated locals as an overall cohort were not congregating as, ahem, vigorously, their infection rate is being misleadingly discounted by a lower exposure rate: The 42% of “resident infections” from the study thus may be skewed strongly in one way or another. From the study:
Second, asymptomatic breakthrough infections might be underrepresented because of detection bias. Third, demographics of cases likely reflect those of attendees at the public gatherings, as events were marketed to adult male participants; further study is underway to identify other population characteristics among cases, such as additional demographic characteristics…
To this can be added, that previously infected individuals may have made up a substantially higher proportion of unvaccinated residents and visitors to Provincetown than of the vaccinated; particularly as previous infection itself is one of the factors individuals may use to decide whether to receive the Covid vaccines. It is not likely that this would skew the results more than ~10% (vaguely the percentage of Americans who have officially been infected with SARS-CoV-2 to date), but only a comparison of infection rates limiting the denominator to the not-previously-infected would rule out a larger potential “margin of confound,” in advance of which this meaningfully adds to the reasons for the CDC or anyone else not to use the Barnstable County study as pretext for a pivot on vaccination infection/spread efficacy.
Instead, use the data from Israel, the UK, and your own eyes.