
Invisible Apocalypse
Will the virus really play a major role this winter? And just what was driving excess deaths in the US during the summer?


If there’s one thing Pretend High Pandemic Priest Eric Topol and many Covid vaccine skeptics are in agreement about, it’s that “Now is not the time for happy talk” with regard to the virus.1 Things are going to get bad this winter - whether because of too little or too much use of the Covid vaccine being the point of disagreement, of course - and the present lull is merely the calm before the storm.
But is this really the case? Sure, things look sketchy in the Northern US and central Europe. But does that imply coming disaster for Florida? Or Israel? Or - get ready for a shock - Australia?

Australia is an aberration, of course. Almost a year after widespread approval, evidence for the ability of the Covid vaccines to suppress test-measurable waves of infection is nearly nonexistent. This is because the experimental injections were rolled out at a time when waves were already on the decline or were nonexistent almost everywhere in the world, save for South America.2
Australia’s delayed rollout is the first real opportunity to re-run the experiment. And, despite still-open questions about the consistency of manufacture and cold chain, this run at last seems to reveal an association between widespread rollout of the Covid vaccine and effective suppression of cases.3
Of course, it may in fact be the case that despite over a year and a half of national isolation, Australians possess the same strong “dark matter immunity” against SARS-CoV-2 that seems abundant all around the Pacific - but for now the reversal in cases and the rollout of the Covid vaccine are two realities which clearly exist in the same place at the same time (meanwhile, Australia’s stupid statewide lockdowns cannot plausibly be credited with the October reversal, since they were already at or near “100% strength” back in June). This isn’t meant to endorse the use of the Covid vaccines to make charts do cool things. There is no politically practical way to operationalize the idea of rolling out the Covid vaccines exactly while a wave is about to take off; even if there were, it’s too late to do so - the shots have already been rolled out, and we don’t know if triple-dosing will have the same effect; and, last but not least, suppressing cases in the short term does not imply any net benefit in the long term, outside of the fraudulent Herd Immunity paradigm which has already been refuted.4
My point, rather, is that although short-term “positive” impacts on case counts from mass Covid vaccine uptake are necessarily rare, they are possible. Of course they are possible - in the short term, these injections prevent test-measurable infections (though, we don’t yet know if this is true for boosters; more on which below).
The default temperament in Covid vaccine skeptic world seems to be a sort of libertarian self-assurance that meddling into complex systems can never produce a positive outcome. As always, such libertarian utopianism is merely the flip-side of interventionist utopianism. Seen though the interventionist temperament, the intervention is perfect, and the political impracticality of rolling it out effectively is an exogenous flaw which should not count against the perfection of the intervention. Seen through the libertarian temperament, accidentally effectively-applied interventions are prima facie impossible.
And in the end, neither side needs to acknowledge real-world examples that contradict their belief. Topol can comprehensively review the failure of Covid vaccines to suppress (later) case rates in order to nonsensically prescribe, as a cure for still-later case rates, more Covid vaccines now. When these fail - despite his present confidence that dose three will be the nail in the virus’s coffin if only we shoot up with enough gusto - he will doubtlessly fault the “delay” in uptake: A delay defined without reference to any concrete schedule, and thus endlessly implied as whatever the actual rate is “+ 1 faster.” Covid vaccine skeptics, meanwhile, can careen from trotting out one broken clock to the next as often as the sun rises - with so many different clocks that spell “Vaccine failure,” one of them will always be right on a given day, enabling the vindicated skeptic to crow, “See, this is what I said would happen (hyperlink to previous post) if we rolled out a leaky vaccine during a pandemic!”
Never mind that we’ve been doing so for as long as there have been “vaccines.”5
Now, Covid vaccine skeptics are not making a bad bet when they predict that case rates will be high this winter. I think it is pretty likely. But it is still just that: A bet. The actual numbers have yet to come in. There is still room for the virus to mysteriously abate, or for the pseudo-vaccines to temporarily delay spread. In which case, “happy talk” on the subject of the virus will be vindicated after all.
And what of the outcomes that will accompany these possibly rampant winter cases? I remain sanguine.
Since August, I have predicted that antibody dependent enhancement is probably not going to arrive until another year or two of “antigenic drift.”6 Despite the scare induced by Trevor Bedford’s September analysis of the super-accelerated evolution of the SARS-CoV-2 spike protein between late 2020 and mid 2021,7 Delta has remained dominant, at this point settling down from “flavor of the month” to “flavor of the half-year.”
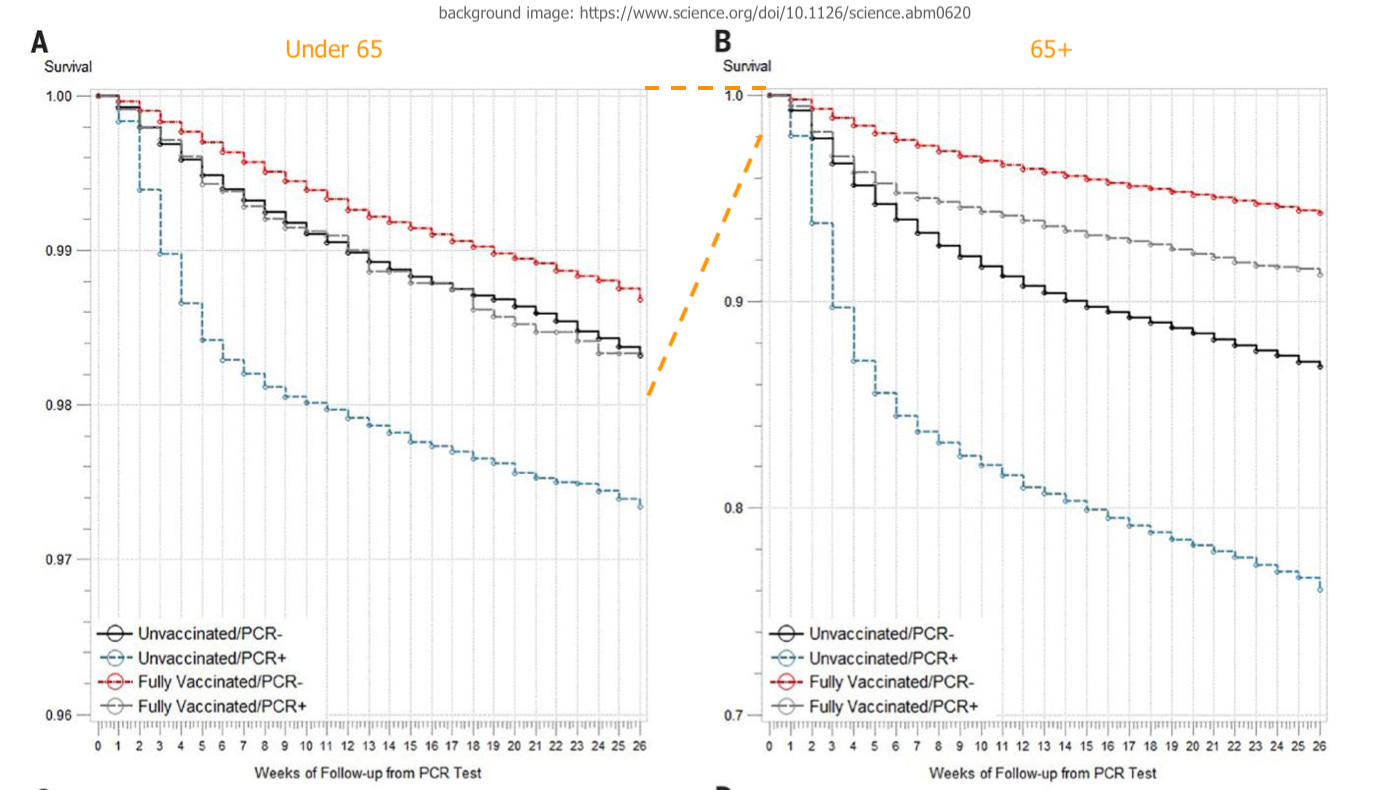
Meanwhile, a paper appearing in Science ten days ago provides an updated snapshot that suggests “deaths efficacy” was still holding at +50%-70% for Covid-vaccinated veterans even into September, sans booster.8 Although there are significant limitations to the study design - the “negative” for each cohort was not a proper control group, but rather individuals who were tested for infection for some reason or another - and despite no raw data being provided, the authors’ own analysis asserts (emphasis added):
[A]mong those with a positive PCR test on or after July 1, 2021, vaccination was protective against death […] For age ≥65 years, VE-D was 71.6% […] for any vaccine; 52.2% […] for Janssen; 75.5% […] for Moderna; and 70.1% […] for Pfizer-BioNTech.
As a perfect picture of reality, there is not much to recommend this study beyond the likely accuracy of Covid-vaccination status (outcomes for the “partially vaccinated” were excluded from the results, which has no bearing on the question of boosters anyway). But it at least reinforces the global lack of any evidence that severe outcome efficacy wanes alongside with infection efficacy, no matter how much Covid vaccine skeptics would like to torture the data to suggest otherwise.
As it has been since August, the question is not whether boosters will “save” the Covid-vaccinated from worsened outcomes - since they are already protected - but whether they will imperil them, by reviving “escape pressure” on the spike protein. I have my own hunch, but the reader is probably better served by letting time or their own judgement lead the way.9
Moreover, the efficacy against “waves” of boosters is even more ambiguous than the initial (1 and 2 dose) rollout was.
To pick on Topol again, one could credit the aggressive booster roll-out in Israel with finally reversing the summer wave - an “unequivocally proven” fact, in his view10 - but as noted previously this would be ignoring the simultaneous reversal of the summer wave throughout the Southern US, most notably in Florida. Things certainly seem pretty “equivocal” down there.
Further, preliminary data show that booster uptake, without accompanying edits to the passport system as already implemented in Israel, is not nearly as enthusiastic as the initial two-dose binge - this lack of “voluntary compliance” is the very reason for Topol’s fear-mongering predictions to begin with, after all.
With what we know so far, I think it is unlikely (but not impossible) for the boosters to contribute to suppression of the coming winter waves (if they lead to a reduction in infection at all11). Similarly, it seems unlikely (but not impossible) for the boosters to massively accelerate pressure against the currently popular model of the spike protein.

All of this is important in a way that goes beyond merely concern-trolling for my own “side.” The broad refusal among Covid vaccine skeptics to accept that older unvaccinated are driving “Covid deaths” to at least a significant degree leads to a failure to ask certain questions. Most notably: Why are so many still being allowed to die in the US? and, are many not only being allowed to die, but essentially murdered by improper care?
This brings me to a recent post by the blogger who goes by el gato malo, “the strong incongruity of reported vaccine efficacy against covid death and all cause deaths.”13
In this post, the author proposes some sort of paradox between the asserted “deaths efficacy” of the Covid vaccines, and the increase of excess deaths among Americans over 65+ so far this year compared to all of 2020. In fact, the trend is just as visible for middle-aged adults:14

Loosely taking death rates among young adults as a proxy to litigate the question of whether deaths “from Covid-19” are driving this increase, el gato malo concludes that the increase is instead a strong signal only for Covid vaccine-induced deaths.
It’s unclear, however, why young-adult death rates are a meaningful measurement of fatality from an infection that does not threaten young adults; and anyway the US still keeps official counts for overall deaths “from Covid-19.” In deciphering whether Covid vaccine harms or infections are driving higher deaths, we can look at these numbers to interrogate whether the increase can be a signal for both things. This makes more sense, since the Covid vaccines were rolled out in the late winter (during the first rise in excess deaths among 45-74 year olds), and test-confirmed “cases” for infection with SARS-CoV-2 dramatically increased starting in July (during the second rise).
Using the cumulative death timestamps in Worldometers, we can make the following comparison between “summer Covid-19 deaths” in 2020 and 2021:15
Oct 15 - July 15
2020
226,534 - 142,544 = 83,990
2021
748,469 - 627,080 = 121,389
Beween mid-July and mid-October, almost 40,000 more deaths were attributed to “Covid-19” in 2021 vs 2020.
The corresponding increases to usmortality.com’s figures for “excess deaths” for Americans of all ages:
Week 43 - Week 30
2020
243,704 - 148,954 = 94,750
2021
362,067 - 178,723 = 183,344
Almost 90,000 additional “excess deaths.” 20,000 of these can be attributed to ages 25-44, who, importantly and predictably, show less of a relative rise corresponding to the summer wave itself - but who are still climbing rapidly against baseline throughout the entire year:

These 20,000 excess deaths between mid-July and October, therefor, could be predominately due to the Covid vaccines. As could some of the remaining 70,000, presuming deaths related to boosters after September played a part. (Alternately, the increased baseline rate among all age groups is driven both by vaccine-harms and by factors like delayed and substandard care for everyday medical issues, with no way to assert which is the primary driver.)
Thus - bearing in mind that the evidence for a drop in “severe outcome efficacy” among the Covid-vaccinated does not exist anywhere - it seems plausible that the rise in “Covid deaths” this summer was driven predominately by the unvaccinated. As for why there should be more deaths in 2021 than 2020, despite the broad use of (death-protective) Covid vaccines, despite the increase in natural immunity via infections and recovery since last year, despite the previous exposure and deaths of the most vulnerable, there is one simple explanation: In summer 2020, it was vaguely understood that the treatment regimen of the spring - do nothing, take Remdesivir, get ventilator-ed - was a mistake; not only ineffective, but actively harmful. In summer 2021, it seems - vaguely, again - as if hospitals throughout the US pivoted back to that outdated regimen in lockstep, presumably motivated by the still un-updated provisions for Covid-19 in PREP Act.16
The resulting increase in deaths would thus imply that around 40,000 unvaccinated Americans between ages 45 and 74 have been killed by American hospitals since the summer, via suppression of effective therapeutics and deliberate use of Remdesivir and ventilators.

Topol, Eric. “Covid cases are surging in Europe. America is in denial about what lies in store for it.” (2021, November 12.) The Guardian.
Most notably in Brazil, which also seems to finally show a plausible association between uptake and reduction in cases. However, since Brazil’s Covid vaccine rollout was so slow, half of recipients will be leaving the “infection efficacy window” in the coming two months, implying that a resurgence of cases is possible.

Covid vaccine skeptics, therefor, have used this accident of timing to (justifiably) discount the association between the shots and the decline of the winter waves, and to (unfairly and triumphantly) assert an association between the shots and any subsequent uptick in cases - as if there would not have been an uptick anywhere in the world this spring, but for the Covid vaccines.
All year long I have found this theory lazy and perilously over-assured. Still, one could torture the Australian data (I can reuse the phrase because this is the footnotes) to infer yet another “smoking gun” for “1st Dose Waves” if one really wanted to. Although 1st dose rates still increase after early October, they do so more slowly than before. At the same time, the rise in cases reverses. Spoopy…

There aren’t many countries in the West with a population similar to Australia (25.69 million), to give a sense of how early the Australia wave has been reversed (at only 2.5k test-measured cases per day).
West-adjacent Romania (19.29 million) at least set out to Covid-vaccinate like the West, with predominant use of Pfizer - but as with other countries in Eastern Europe, overall uptake was quite low. Still, there is an interesting lack of association between the increase in first doses prompted by the autumn wave (as also seen in other Eastern European polities) and the reversal of the wave. Despite an additional million 1st doses since mid-September, the wave turned around (reporting on vaccine rates is 20 days behind case rates):


Not all viruses are alike™; not all vaccines are alike™. For my proposed explanation for why Covid vaccines will not create a “Marek’s Effect” on coronavirus, for example, see “Crackpot Corner: Marekspocalypse Edition.”
See “Boostermania.”
See “Saving Private mRNAyn.”
See Cohn, B. et al. “SARS-CoV-2 vaccine protection and deaths among US veterans during 2021.” Science.
The study also prompts serious questions into the distorting power of selection bias for who does and does not get a Covid vaccine (with individuals experiencing severe medical issues to begin with, for example, tending to sort into “unvaccinated” cohorts by default), since both segmenting by age and “±3 comorbidity score values” fails to eliminate a magic protective effect for “PCR negative” recipients compared to unvaccinated (again, however, the conditions that lead Covid-vaccinated and unvaccinated veterans to be tested to begin with might not be the same, meaning that any two “PCR negative” groups are not alike).
My hunch is that boosting will not drive escape pressure. To suppose that it will invites a paradox: First, it requires asserting that the original Covid vaccine roll-out was responsible for the rapid changes to the spike protein that led to Delta, via escape pressure. Then, it requires asserting that Delta is not capable of escaping the vintage-2020 antibodies stimulated by the Covid vaccines at all.
One solution to this paradox might be that the virus is responding to an impossible-to-measure “sub-neutralizing spread escape pressure.” In this model, the virus is still able to spread from cell to cell, person to person in the face of “neutralizing” antibodies, at a very low frequency rate, during intervals between waves. However, inserting a role for anti-spike antibodies into such a model still implicates natural immunity to some extent. As I said, the reader is better off forming their own guess of what is going on.
(Topol, Eric.)
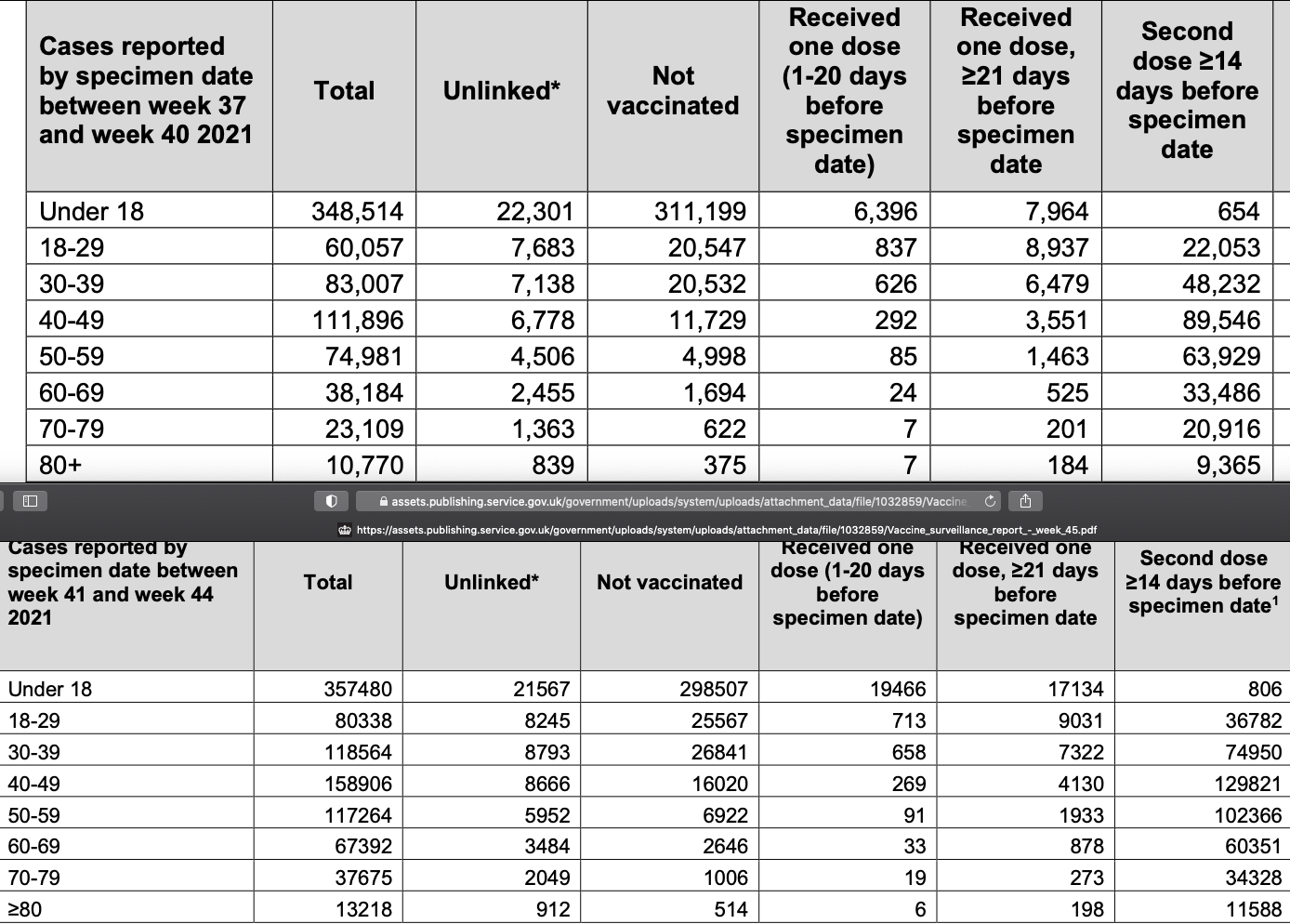
Relative per-100k case rates in the Israel dashboard continue to suggest this is the case. However, as the summer wave has almost fully subsided, “cases” are likely dominated by false positives for the moment. Figures from the UK seem to cast boosters in a far more negative light. Although the triple-dosed are not given their own category, it is odd that absolute case rates continue to rise among the “+14 days 2nd Dose” elderly despite two months and 8 million doses of boosters. From Weeks 41 (October 14) and 45 (November 11) of the UK Health Security Agency report (https://www.gov.uk/government/publications/covid-19-vaccine-weekly-surveillance-reports). Note that absolute rates among 40-59 year olds were already surging in the first report, likely due to high testing rates among school-teachers:
el gato malo. “the strong incongruity of reported vaccine efficacy against covid death and all cause deaths.” (2021, November 12.) bad cattitude.
Your final line “around 40,000 unvaccinated Americans between ages 45 and 74 have been killed by American hospitals since the summer, via suppression of effective therapeutics and deliberate use of Remdesivir and ventilators.” is what I think is super important. They are STILL &#@!^? killing people by censoring *EFFECTIVE* EARLY TREATMENT. Fortunately word continues to spread through independent media.
I keep going back to the question of 'Why did we choose to go with mRNA technology based 'vaccines' rather than our traditional inactivated or dead whole virus method?' We had decades of research on coronaviruses and influenza to understand that nothing could actually inoculate us against rapidly mutating aerosolized viruses. If life saving measures were the goal, we'd have attempted vaccines similar to the influenza model. We would have embraced, and allowed off label use, of any medication showing promise. Rather, we chose a novel technology on a novel virus and denied the right to try early treatments. This could not have been for anything but money (greed). The NIH and Moderna had the sequence ready to go. Big Pharma gets tax payer funded, liability free research for mRNA technology on billions of people. All of this to determine the true downfalls of mRNA technology and its limitations in application. The anti-virals are an equal, money making scam. They know damn well Remdesivir is dangerous, especially for people sick enough to be admitted. They know damn well that Molnupiravir is dangerous and they'll push it anyway. Pfizer ripping off Ivermectin to develop Paxlovid is, atleast, potentionally capable of actually helping people (unless they put unnecessary toxic ingredients in it).
I don't think the evidence truly exists to suggest that these 'vaccines' are remotely effective at reducing severe symptoms and death. There are too many variables at play. Big Pharma destroyed their control groups at 2 months. We know that the data is manipulated, often flat out false at times. There is every incentive to continue pushing some hope with the vaccines. I am going with- they do not work in any capacity, the long term harms are coming and humanity has shown the absolute worst sides.