


The War On Pee
Around ten years ago, a medical myth over 150 years old was upturned: Urine is not sterile. And yet, billions of dollars per year rest on continuing to pretend that it is.

How many urologists does it take to screw in a lightbulb? Probably just one. But how many does it take to promote the health and function of the recently-acknowledged Urinary Microbiome, instead of destroying it over and over again with antibiotics?
And, more importantly - are any of them even trying?


I also sometimes think I'm creating a monster of a UTI infection that will be resistant to anything.1
2021: Women throughout the West are in revolt. After suffering two decades of constant yearly growth in the rates of first-time and recurrent urinary disorder in every adult age group, they are rejecting the conventional approaches outright, having recognized them as the very mistreatment which caused their ailments in the first place. Urologists, already having recognized that something was wrong with their approach over ten years ago, are meanwhile entrenched in the fiction that these trends were being caused by the ever-handy scapegoat of antibiotic resistance. Meanwhile, no effort was even put into reversing these trends of medical harm until the revolt had already started.
By then it was too late. Restoring trust in modern medicine among women seems, at this point, impossible; and the mistreatment of urinary disorders to be entirely to blame for the crisis. Meanwhile, medicine’s scapegoating of antibiotic resistance for its own failures of care has only magnified the alarm and anxiety expressed by women suffering from recurrent urinary disorder. A snapshot of the mistrust and desperation prevailing among women who have suffered under the mistreatment of urologists is revealed by a new paper, which presents results from a focus group undertaken among patients experiencing what urology still insists on mislabeling “recurrent Urinary Tract Infection™.”2 Sample comments provided by the paper include:
You can't count on doctors.
Now I have developed a phobia of antibiotics
UTIs have made me skeptical of doctors in a lot of ways.
My antibiotic for UTI once put me in the hospital for three days with [inflammation of the colon from Clostridium difficile monoculture disorder]
Treating it like it's in your head or you're kind of making a bigger deal out of it doesn't help
I feel like nowadays, antibiotics are prescribed for everything and they shouldn’t be…walk into Urgent Care like oh, here have an antibiotic you have a cold. You don’t need that
sometimes even the strongest antibiotic won't work for somebody. That's why some people are dying in hospitals
Where did this crisis come from? And how great the scope? Guessing how many women have fallen victim to the 21st Century’s epidemic of recurrent urinary disorder is difficult. Current figures for how many women will experience at least one urinary disorder event in their life are often quoted around 50%; in 2011 they were roughly the same; while in 1999 they were around 40%; and sources in all these eras are often derived from other sources that are already nearly a decade out of date at the time. But overall, healthcare visits for urinary disorder in the first two decades in the US and the UK seem to have doubled, if not almost tripled. An extensive analysis in 2011 found that between 1998 and 2009, the number of hospital admissions for older women increased by over 17% per year:3

Annual costs in the US, meanwhile seem to have leveled off somewhere just over the $2 billion mark. The leveling, however, is due to the concurrent plunge in prices for antibiotics themselves - the rest of that $2 billion having shifted into the pockets of the predatory healthcare systems prescribing them.
Urinary disorder is a devastating ailment. In perfect health, urination might seem like matter for (literal) toilet humor - an object of biological derision or shame; an inconvenience at best. In ill health, urination reveals itself as no less essential to the human experience as breathing - and painful or restricted urination, no less terrifying and debilitating than having one’s mouth and nose sealed shut.
Yet urologists in the West seem to regard the primary goal of their work as getting their patients to leave them alone, and to regard the female urinary tract as a perpetual burden to humanity and an object of bacteria-ridden shame. In this, of course, they reflect the harmful attitude toward urination prevailing within the urbanized West as a whole, which has defined as “normal” a barbaric and nearly unlivable taboo against (primarily female) outdoor urination.
While in Ancient Rome, supposedly an era of medical primitivity, laundromats would line city streets with pots which were used for immediate relief by every citizen, in our modern era we pride ourselves on waiting in indoor lines to access filth-ridden cells while our detrusor muscles are pushed to their inevitable breaking point.
Our refusal to confront these harmful taboos has led to a completely predictable medical disaster in the wake of the entry of women into the gig transportation economy: Unknowingly signing up for a form of work that has always been sustained by unspoken male in-vehicle urination, female gig drivers have become stranded in a world not built for them, and their bladders and their mental health have borne the cost.4
But if the West at large has been waging war on women’s urinary tracts, that hardly excuses urologists from doing their best to lead the charge. Yet when the farcical myth of the sterility of the urinary tract was at last upturned in 2013, not a single change was made to urological care in response. And despite the ongoing revolt from their patients, the field is still dragging their feet on acknowledging the Urinary Microbiome, as well as the absurdity of treating bacteria in the urinary tract as an invader which must be repelled by any means necessary. And while several individual urologists have, at last, descended to the front lines of the revolt to attempt to staunch the exodus of their own patients (or to try, fruitlessly, to co-opt the revolution), urology at large seems intent on pretending that nothing is even wrong. The focus group study quoted above, which captures the breadth and intensity of the revolt against medicine, has only recently been posted online, ahead of an official September 1 print date - but it was submitted for publication back in March.
Women seem to have intuited that antibiotics are making their urinary tracts more dysfunctional, and a new paradigm of care that emphasizes microbiome health must be found. But the sample statements included in the new paper leave out, for the most part, the skeleton in urology’s closet: The refusal to acknowledge the Urinary Microbiome. According to the authors’ analysis of the focus group transcripts, growing awareness (and continuing medical neglect) of their digestive and genitourinary microbiomes was the second most important concern regarding antibiotics among participants, after antibiotic resistance (emphasis added):
Women described a strong knowledge of collateral damage from inappropriate antibiotic use, which fueled their fear. Many reported learning about the negative impacts of antibiotics from Internet searches, magazine articles and television programs, and not from physicians. Numerous women stated that they had reached such a level of concern about antibiotics that they would resist taking them for prevention or treatment of infections, even when prescribed by physicians.
The first theme addressing the negative impact of antibiotics discussed by participants was the development of antibiotic resistance. During these discussions, women noted concern for their own ability to be treated for future infections, but also acknowledged the broader implications for society as a whole. Second, women reported concern about the collateral damage of antibiotics on their gastrointestinal and genitourinary microbiomes. Several women had subsequent Clostridium difficile infections after taking antibiotics, with 1 requiring hospitalization, and many noted general gastrointestinal disturbances that had taken several months of recovery.
These are both important concerns in of themselves, as well as competing theories for the rise in in first-time and recurrent urinary disorders. Is this surge due to over-prescription of antibiotics in the first place, or due, as the study from 2011 suggested, to an increase in antibiotic resistance? We will only need to examine if the rate at which first-time urinary disorders treated with antibiotics have led to recurrent urinary disorder has risen, or stayed the same - for their is no plausible reason that first-time patients should already be suffering from an antibiotic-resistant Urinary Microbiome monoculture. Moreover, an improved understanding of microbiome polycultural diversity in the last two decades has made the framing of the “antibiotic escape by natural selection” narrative largely obsolete.5
Instead, could this modern medical disaster all be the result of reversing a forty years-old, absurdly-high threshold for clinically designating urinary tract “infections”?
Did removing the Urine Culture-based standard known as the Kass Threshold - a move intended to bring more nuanced care to women who were reporting symptoms of urinary disorder - unintentionally create a path for doctors of all types to inappropriately screen for “asymptomatic disorders” - in other words, to prescribe antibiotics to women whose Urinary Microbiome was actually in perfect health? Is this what has driven the explosion in urinary disorders among women in the West?
A clue for this mystery lies in the chart above. If we have indeed been in the midst of a two-decade medical assault on the Urinary Microbiome, women are not the only apparent victims: Elderly men have suffered at equal rates as younger women. Meanwhile, potential excessive screening events prompted by irresponsible surgeons and elderly care center administrators have coincidentally just come to light.6
The humble and miraculous bladder thus finds itself in the center of a historic medical revolution unlike any other - one led by the patients, not the doctors. An irresponsible and backwards pseudo-medical regime finds itself confronted by a sudden, widespread revolt among its own long-terrorized subjects. Women throughout the west are rejecting en masse the “wisdom” of their predatory caretakers and the fiction that reproductive and urinary medicine is helping, not harming them. Their great turn toward remedies natural, super-natural, and hyper-unnatural has thrown gynecologists and urologists into a crisis of alarm, dismay, and suppressed guilt; and though they have attempted to quell the revolt by descending from their intellectual towers to the front lines of social media, they have been met at every turn with suspicion and resentment.
The era of medical tyranny over the female Urinary Microbiome seems to be at an end. But will the revolution result in true gains of health, or merely a mass revenue transfer to the marketers of false cures, including radical, potentially life-altering surgeries, leading ultimately to a backlash that lands our incompetent “expert” doctors back in charge? With $2 billion dollars of annual revenues on the line, will urinary “microbiome prosperity” truly, finally be allowed to flourish?

I don’t understand how we can do heart transplants and land on the moon and not kill the bacteria in my bladder.7
The Last Microbiome
In 2008, after over a two centuries of scientific darkness, man at last embarked on a journey to explore the most poorly understood natural environment on Earth. No, not the alien realms of oceanic trenches and toxic mineral springs, or the frozen wonderlands of Antarctic underground rivers - but the human body. That is to say, the healthy human body.
At that time, a revolution in human understanding of the natural world - and especially of disease - appeared to be underway. Decades of microbiological observations, finding sophisticated quorum-sensing-based communal behavior and phage-mediated communication and immune-like function among bacteria, as well as the proliferation of strains previously considered pathogenic within the healthy human gut - had tilted over all the pillars sustaining medicine’s superstitious, antagonistic conception of the microbial universe. The five-planet journey of the “Human Microbiome Project,” therefor, was an effort to repair diplomatic relations between man and microbe, a good-will tour of existential significance. Funded by the National Institute of Health, the expedition set out to map the five then-known realms of healthy bacterial-human coexistence: The digestive tract, the vagina, the mouth, the nasal cavity, and the skin.9
The sixth world, the Urinary Microbiome - and a larger nebula of bacterial presence pervading everywhere within the body that man had previously envisioned as a barren void - was yet unknown. It would begin to be recognized two years into the voyage. But this was too late for any change in itinerary.
The landmark paper arrived in 2016, but built off of a presentation from 2014. The title did not mince words: “The bladder is not sterile: History and current discoveries on the urinary microbiome.”10
Although the authors relied heavily on direct access to the bladder for their samples, they additionally applied their method to naturally voided urine and found almost equally promising results. The crux of their method lay in the grounding assumption: There’s more than just “pathogenic” bacteria in the normal, healthy human urinary tract. Thus, they set aside normal bacterial culture standards in favor of a diverse set of culture-conditions, which allowed less hardy or metabolically indiscriminate strains to grow. Under these conditions, the full richness and complexity of the Urinary Microbiome was allowed to put itself on display.
The implications of their work were and still are profound. If there is a Urinary Biome, then bacteria in the urinary tract are likely providing a host of beneficial immune, metabolic, and even behavioral regulatory functions, just as they have been observed to do in the gut. Further, if the similarities in bacterial profiles observed between the Urinary Microbiome and the Gastrointestinal Microbiome hold up in further studies, every standard assumption of fecal bacteria being a threat, rather than a partner to female urinary health may be upturned. In short, the study suggested (and still suggests) that everything urology thinks we should be doing is flat out wrong!
And yet prospects for progress were dim from the start.
The Human Microbiome Project, having received over its entire course a mere 170 million dollars, or .57% of the Institute’s budget for 2008 alone, was retired in the same year, having left the Urinary Microbiome in a condition of near-absolute neglect. Nor did the Project proffer, for any of the five worlds it did visit, anything akin to Tocqueville’s dense, timeless reflections on America - it delivered, instead, a monument to the incomprehensibility of our microbial brethren, as if we should endeavor to learn these foreign realms’ languages and customs by feeding their phonebooks into computer algorithms to look for meaningful patterns between names and addresses.
Nor had the Project signaled a pivot toward warmer relations with these foreign realms: For as regards the medical revolution which seemed to be gaining steam when the Project launched, progress had mysteriously fizzled. Attempts to understand the beneficial relationship between bacteria and phages had slowed or been abandoned, and medicine’s gaze had turned toward genetic intervention into yet another language that was continually being fed into computer algorithms as a surrogate for genuine human comprehension, a path which could only “productively” lead to the destruction, not improvement, of the human medical condition. Thus, no sooner was “peace” declared in the war against microbes of the gut, mouth, etc., than hostilities were shifted to the human cell itself.
Yet in the neglected realm of the urinary tract, anti-microbial peace was never declared at all; in fact the war against the Urinary Microbiome raged on with more intensity than ever. The medical war against nature, in other words, may have narrowed its focus, but it was still growing more brutal and devastating by the day. And as for the newly discovered Urinary Microbiome, and what it might imply for the treatment of urinary disorders still being miscategorized as “infections,” well - it was simply ignored! And why not? Medicine got away with ignoring the Urinary Microbiome for over a century, why couldn’t it keep doing so for another one? But after a mere five years, the bill has already come due.
The Urinary Microbiome may be a novel frontier in research, but it has been staring medicine in the face for as long as the first attempt was made to discount it. Even at the very birth of modern epidemiology’s war on microbes, bacteria could be found in healthy urine samples just as often as in samples from patients suffering from the symptoms of disorder; yet the former samples were deemed proof of the sterility of the bladder, and the latter a symptom of the invasion of the bladder by foreign intruders who don’t belong anywhere on the human body. Thus even though bacteria could be observed in healthy urine under a microscope, the sterility of the bladder was taken as proven by how those bacteria behaved afterward. If that seems nonsensical, or stupid, that’s because it is nonsensical and stupid. If I want to prove that a car does not have gas in it, I cannot take the gas out of the car, observe that it is gas, and then point out that I can’t seem to light it if I put it in a box! It’s still gas!
It’s difficult to overstate the dismal absurdity of this farcical “proof,” and the conclusion in which it resulted, having gone unchallenged by a single individual in the subsequent 160 years of professional medicine. Doctors throughout the West have gone their entire careers accepting a truism about the human body that was based on a proof that never made sense to begin with. And not, “some” doctors. All doctors! For 160 years! And who knows what a survey of beliefs about the sterility of urine would even return today - including among urologists? We may return to 2008, to behold the state of mind prevailing in medicine then:11
Considering the anatomical location of the urethral meatus, it is surprising that urine is normally sterile. [You don’t say?] The defensive properties of uroepithelia help maintain this sterility as strategically necessary for long-term survival […] However, what is entirely curious is that infection of the urinary tract is not more common. The urethra exits so close to the rectum that it guarantees the urinary tract will forever be exposed to enormous numbers of microorganisms. Despite this peculiar design, most cases of urinary infection that occur in children arise in individuals with anatomical or functional disorders of the bladder and/or the distal collecting system of the kidney.
If it was so “surprising” that urine should be sterile, and if the supposed proof of that sterility was so laughably flawed all along, then why didn’t anyone question whether it was actually true?
Part of the reason, probably, was that it was understood to begin with that it is impossible to “prove” that healthy urinary tracts either should or should not include bacteria. Urine must travel out of the body to be examined - on its way out, it must pass through anatomy that we can see for ourselves is rich with bacteria. Thus, the presence of bacteria in voided urine is not itself what proves that it was already there, back in the bladder. Similarly, every attempt to to circumvent the normal route of exit must, in theory, itself create the risk of spoiling the resulting sample. Indeed, it was well-known that catheterization was often followed by urinary disorder; and this was taken as proof that “violation” of the bladder from without is the source of “infections” - rather than that violation of the Urinary Microbiome from without by synthetic instruments disrupts the bacteria that are already present, prompting a conversion from a harmonious polyculture to a biofilm-heavy monoculture.
This belief persisted despite the discovery, in the mid-1960s, that manual repeat self-catheterization produced fewer “infections” than professionally-administered, ultra-sterilized long term catheterization (you’d think someone would have got the message at some point!).12 In the end, since there was never going to be a way to escape this bacterial Schrödinger's box, 160 years-worth of medical professionals accepted a dogma that by their own admissions never made sense to begin with, despite the implications of what it would mean for the dogma to be incorrect. Namely: All current treatment for urinary disorder was making the problem worse.
Now the dogma has been overturned. The implications must be acknowledged.
There is not, and never was, any such thing as a “urinary infection.” Only a disruption of the normal harmony of bacterial-human affairs.
There is not, and never was, any way to attack the hardier strains of bacteria which form a monoculture when their fragile environment is disturbed, without purging the last remnants of the more delicate strains as collateral damage.
There is not, and never was, any way to to tell whether the principle advice created from the sterility fallacy - which direction toilet tissue should be wiped - does harm, not good.
There is, and always was, a world of discovery and progress to be made in learning how to preserve unique healthy Urinary Microbiomes and banish this particularly dehumanizing brand of suffering from the Earth, that medicine could have embarked upon all along for the last 160 years!
But really, it took me months before my system got back to normal…because of the antibiotics I had been taking to ward off these things, before I started on the small doses, the flora in my stomach was a mess. And so there were all these things going on, and it took months. It took maybe 4 or 5 months for me to get my system back as well as my head back to where it was supposed to be.13
Test Toward Enemy
What was it about the end of the 20th Century that potentially created the surge in urinary disorders that would follow? Ironically, it was the dismantling of another outdated urological myth. Throughout the 90s, the standard which was adopted by accident in the late 50s was extensively reexamined. That standard - authored, again accidentally, by Edward Kass - had been designed as a Urine Culture threshold to diagnose kidney inflammation. Namely, it stated that a Urine Culture should “produce 100,000+ whatevers per bla bla bla.”
For the next 40 years it was nonetheless employed as the threshold for diagnosing symptomatic bladder inflammation - a.k.a. UTI™ - with the predictable effect that patients who were experiencing symptomatic bladder inflammation and urinary disorder were denied care due to failing to meet a standard of whatevers per bla bla bla that was never even designed for them.
It might seem that only good could come of lowering the standard, or moving to more nuanced care in general. Indeed nothing appears wrong on the face of things with the state of common practice adopted in the 90s: Recommended thresholds for “asymptomatic bladder inflammation” remained at 100,000 whatevers, but for treatment of symptomatic patients, flexible testing standards and common sense were encouraged.15 If lower test standards, in other words, are used only for symptomatic urinary disorder, there doesn’t seem any reason that previously healthy individuals would be affected - and further, the testing of urine itself would become largely a formality, and medicine would move closer to treating the presence of bacteria in urine as normal and healthy in practice. This is because the elements of regular urinalysis that are used to evaluate levels of bacteria in urine are more rapid and less exclusive than the traditional Urine Culture, which only favors certain types of bacteria (which is why the new discretionary/symptomatic Urine Culture threshold was lowered all the way to 100 whatevers in most official recommendations).
And yet after these subtle, apparently reasonable changes in the US and many other Western nations, incidence of first-time and recurring urinary disorders appears to have exploded. Thus it must be asked: Were the lower standards also being applied during “asymptomatic” urinalysis? Did the updated standards, somehow, unleash a plague of misdiagnosed “infections” among healthy women and the elderly?

How many patients are being pushed into first-time antibiotic treatment due to unnecessary screening before surgery or elder care admission? A few studies, including one published earlier this month, seem to offer a surface view of the overmedication iceberg which has pierced the hull of humanity.
Our glimpse into incidences of improper urinalysis prompted by American surgeons comes via paper posted online a few days ago, excitingly named “Prevalence, Costs, and Consequences of Low-Value Preprocedural Urinalyses in the US.”16
In this paper, the authors examine how often surgeries paid for by private insurers or Medicare were preceded by urinalysis between 2007 - 2017 - despite being categories of surgery for which preoperative urinalysis is not recommended. Thus, kidney and urological surgeries, as well as Caesarian section births, were excluded from the category of possible “nonindicated urinalyses,” and among urinalyses tests in the other categories, those issued for patients who met American Medical Association criteria were counted as indicated (namely, those with symptomatic urinary disorder). The authors’ sources are the commercial and Medicare datasets which cover the better part of the IBM Watson MarketScan database, which comprises a rolling sample of roughly 43 million patients overall.17 Their findings (emphasis added):
Among 13,169,656 [non-excluded] procedures, 25% were preceded by urinalyses within 30 days… Among procedures for which urinalyses were obtained, 89% were not indicated…
The general but rather clear picture is that most surgeries in these categories are not preceded by urinalysis, but almost all that are are possibly gratuitous. Additionally, the authors break down the rates by category of surgery, with the unsurprising result that the second-most predominately non-emergency surgery, joint replacement, leads the pack. This makes it apparent that more foresight leads to more surgeon-prompted gratuitous antibiotic mistreatment (for prostate, colorectal, and spinal surgeries, we may be less quick to condemn the surgeons’ discretion):

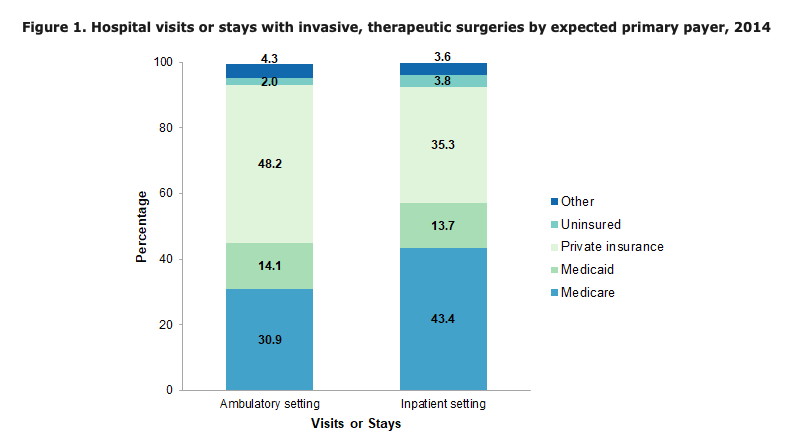
We could flesh out the authors’ results with a bit of math, since they have declined to do so. MarketScan’s commercial and Medicare rolling samples correspond to the insurance pool that comprises roughly 65% of Americans, but 80% of hospital system surgery recipients. Additionally, it might seem intuitive that patients who receive measurable treatment are over-sampled in a “treatment events database,” compared to all Americans. But actually, the authors’ resulting dataset of “13,169,656 procedures” for 11 years of medical history is almost microscopic in scale. Americans go under the knife far more than 13 million times annually - the most conservative rate in 2014 alone was over 21 million times, but that only includes surgeries directly associated with hospital systems. Other sources quote rates so high they boggle the mind.18 Thus, a crude but conservative multiplier applied to the MarketScan 11-year sample would land us somewhere around x 2, just for a per-annum rate.
Except, of course, that our yearly surgery rate needs to exclude kidney surgeries, urological surgeries, and Caesarian section births. The authors, apparently jealous of the MarketScan data which they paid to access and play around with, do not forward the corresponding rates for those surgeries, leaving us with no handy way to discount them when translating the MarketScan sample to a yearly rate. Additionally, the 20% of annual surgeries not paid for by Medicare or private insurance may occur under conditions that do not match the MarketScan sample. Additionally, part of the apparent under-sampling in the study is due to the authors’ limited set of 14 categories, which exclude some of the most common procedures, such optical surgery. The 25% x 89% gratuitous preoperative urinalysis rate in the authors’ 14 categories therefor might not carry over to all surgeries overall; the true overall rate might be much lower, or even higher. Lastly, there is the possibility that a significant portion of preoperative urinalysis was mis-flagged by the authors as “nonindicated” simply because the corresponding diagnosis code didn’t make it into the MarketScan data.19
The study is, overall, less a thorough crime scene investigation than it is a vague report of the observations of limited security camera footage. Thus, any attempt to extrapolate from these results to an absolute annual rate of patients subjected to unnecessary antibiotic treatment by surgical malpractice is quite perilous.
But let’s try anyway!
To err on the side of caution, we will offer an extreme discount for the rate of gratuitous preoperative urinalysis prevailing among the ~20% of Americans undergoing surgery annually who pay via other means (namely, Medicaid or off-insurance).20 We’ll use… eh… 25,000,000… for the going annual rate of non-excluded surgeries in the 2007-2017 timespan. Finally, the rate of resulting antibiotics treatment we will use is reconstructed from the study’s “Figure” diagram above, since the study text itself does not provide a value; the discounted rate recycles the ratio from the first outcome.21
Ultra-vague guess of US annual gratuitous preoperative urinalysis rate, 2007 - 2017:
.8(25,000,000 x .25 x .89) + .2(25,000,000 x .125 x .59) = 4,818,750
Resulting annual antibiotics regimens targeting surgery-prompted misdiagnosed UTIs:
.8(25,000,000 x .023) + .2(25,000,000 x .008) = 500,000
Half a million surgery-prompted gratuitous antibiotic assaults on the Urinary Microbiome per year, on the dot. Magnificently tidy, it must be said. (For caveats applicable to this extrapolation of the study’s results, see footnote 6!)
This presentation of the results, horrifying as it is, is unduly favorable to the surgeons who are recommending preoperative urinalysis for inappropriate categories of surgery. They are the apparent outliers in their fields; and those who drive the most recommendations bear a disproportionate share of responsibility for the resulting harm. However, there is actually no way to tell if this statistical artifact is due to individual surgeons who issue gratuitous urinalysis routinely, or a widespread pattern of selective gratuitous urinalysis; and no way to deem which would be more ethically troubling.

The second front in the possible secret 21st Century medical campaign against “asymptomatic UTIs™” centers on the elderly. Here our glimpse of the situation uses studies which are more out-of-date, and narrowly-focused, than the paper regarding surgeries.
The first hails from Toronto, in 2015.22 In this, 403 primarily elderly patients who passed through emergency care and then transitioned to general care at a local health center were tracked. The authors find that urine testing was ordered in absence of symptoms or kidney-related-injury for 211 of them. What’s more, positive urinalysis results prompted an increased rate of subsequent full Urine Culture; but even among those with negative urinalysis results Urine Culture was ordered nearly half of the time (either simultaneously or sequentially).
What makes such a prospect terrifying to an American reader is that under the new, lower standards of the 21st Century, elderly women test “positive” at a rate of something like 90% in urinalysis regardless of symptoms.23 And many elderly patients of both sexes are incapable of displaying symptoms to begin with, meaning that the only possible treatment they may receive is for “asymptomatic” disorder.
Like infants, elderly patients who suffer from dementia or other impairments to communication are treated as incapable of manifesting all of the actual symptoms of urinary disorder, which are intrinsically subjective: Whether they feel frequent urge to urinate, or pain during urination is unknowable; and so to their care-takers, the results of urinalysis tests and Urine Cultures become “the patient’s voice.” Elderly patients who suffer from dementia, under this paradigm, are theoretically subjected to unnecessary and forced antibiotic courses just for having a normal level of bacteria in their urine for their age.
Thus, the picture afforded by an initial reading of the Toronto study is one of horror; of elderly patients regularly having their Urinary Microbiomes destroyed by destructive medication, merely for the crime of having needed medical help after a fall. The study indeed finds that most of the urinalysis tests and Urine Cultures came back positive. In the end, only 21 of the 211 improper screenings, or 9%, lead to a positive Urine Culture - but that doesn’t stop staff from administering antibiotics 25 times (12% of all improper screenings). As very confusingly laid out within the study:

As a result of this urinary inquisition, 25 elderly patients were given unnecessary antibiotics, whether due to a positive urinalysis result, or a Urine Culture, or neither! However, Canada’s health systems have since launched a campaign to make the process for performing urinalysis on patients in Long Term Care more selective and symptom-focused, including upon contact with the emergency care system.24 It’s possible that the over-prescribing observed in the study has already been corrected. Let us hope so.
The view from the US, however, is equally bleak, and far more recent.
Here our study is from 2019, and is more oblique - it does not offer a focused view of urinalysis-initiated patterns of mistreatment of the elderly, as it only looks at Urine Culture-positive outcomes. Whether the Urine Culture positive are, as above, only a part of a two-pronged push to medicalize healthy elderly urinary tracts is left partly to the imagination.25 Examining records from 46 hospitals in Michigan, the authors identified 7,252 patients who received a positive Urine Culture.
2,772 of them, of course, had been given the test despite not displaying any qualifying symptoms for urinary disorder. In other words, they became, at the moment the test result turned positive, “patients with asymptomatic bacteriuria.”
How many of the 2,772 inappropriately-screened patients were given antibiotics? 2,259 (81%).
How many were suffering from dementia? 560 (20%).
How many were women? 2,138 (78.2%).
With such lopsided and undeniable results, the authors struggle to fill the more perfunctory portions of their report with nuance. The “conclusion” and the “introduction” both read as equally rote, despondent, and directionless. From the introduction, therefor:
Despite national guidelines recommending against antibiotic therapy for [Asymptomatic Bacteriuria], high treatment rates persist.
Indeed. This sentence, notably, links to four other papers in the study footnotes, which also examine over-screening patterns for “asymptomatic bacteriuria” among the elderly from various health systems in 2012, 2015, and 2017.
But perhaps one way to reduce over-screening for “asymptomatic bacteriuria,” would have been for all these researchers to start calling it what it is: Healthy elderly urinary function.
Not a single doctor is willing to explore anything but finding more antibiotics.26
The War of Words
It might seem impossible at first to understand how a field within modern medicine, with its fetish for brevity, could evolve such a convoluted architecture of terminology that “asymptomatic latin gibberish” has become a synonym for normal, healthy conditions.
Until you realize, it’s incredibly easy to understand: Urology has been operating for over 150 years on a backwards premise. Every “advancement” in understanding in that entire time, therefor, has only led to the addition of more novel “corrective” fictions.
Earlier, we mentioned that while the field at large seems unperturbed by the ongoing Revolt of Women, individual urologists have rushed to the streets of social media, to try to shore up support for their crumbling castle of harms. These individuals, now vocally embracing the criticism of the error of their ways, are simultaneously attempting to weave the Urinary Microbiome into the latest updates to their fictions. But are any of them coming up with a new vocabulary of urinary health that doesn’t merely protect the same old mistakes? And could any of them be so bold as to disavow the lie at the heart of all their errors - that urinary disorders are a product of bacterial “infection,” not bacterial disruption?
For our first figurehead of the attempt to call women back into the tattering folds of credentialed urological care, the answer is a resounding no. This would be James Malone-Lee, a four-decade veteran urologist, who joined Twitter three years ago and has spent the intervening time in a hopeless battle of words against the Revolt of Women. Malone-Lee’s attempt to rehabilitate urology after its two decades of malfeasance has been ongoing for nearly half of that timespan, and is encapsulated in the book released earlier this year, Cystitis Unmasked.28
One of the intervening care-trends in the last two decades revealed by Malone-Lee’s work, is that even after the Kass Threshold became counter-recommended for symptomatic urinary disorders in the ‘90s, actual urologists (in the UK, at least) still displayed little interest in listening to women who were complaining of symptoms. Thus while possible millions of women with healthy urinary systems have been subjected to unnecessary and destructive antibiotic courses in the last 23 years, other possible millions with symptomatic disorders have been denied validation and sincere attempts at care, still trapped in the absurdly high Urine Culture threshold that dates back to the late 50s and was never designed for urinary tract care.
The manifestation of this preservation of the ingrained habits of the late 20th Century, naturally, is the rise of yet another novel and meaningless term in urology: “Interstitial Cystitis.”
This phenomenon appears to be particularly prominent in Malone-Lee’s homeland, where the nationalized health care system seems to favor minimalist treatment, even for children, just as often as overmedicating. Thus, a satisfactorily representative definition for the fictional condition of Interstitial Cystitis (and the top result in a Google search for the term) is provided by the UK’s National Health Service:29
Interstitial cystitis is a poorly understood bladder condition that causes long-term pelvic pain and problems peeing.
In other words, “Interstitial Cystitis” is… symptomatic urinary disorder. “Interstitial Cystitis” and “Asymptomatic Bacteriuria” are merely two sides of the same Urinary Microbiome-denying fictional coin: The two-century-old myth that urine ought to be sterile demands that low-Culture-result patients experiencing pain cannot have anything wrong in their Urinary Tract relating to bacteria, and that high-Culture-result patients in perfect health cannot not have something wrong: In both cases the clear fact that the given patient disproves the myth is simply waved away!
And the fictional construction surrounding this coin and binding its shape and structure, of course, is that original fiction: “Urinary Tract Infection.” For patients landing on the rim, destructive broad-spectrum antibacterial regimens are applied in the hopes of dislodging the patient onto one or the other sides of the coin; for patients landing on the ASB side, aggressive application of test results is used to portray the patient’s previously healthy, polycultural microbiome as a disease in need of medication; for patients trapped on the IC side, outdated, inappropriately-high thresholds are used to dismiss the idea that anything might be dangerously out of harmony within their current microbiome at all.
The fabrication of the “Interstitial Cystitis” fiction is still an important exhibit in our court-martial of modern urology. It reflects the fact that the more patient-centered recommendations for symptomatic urinary disorder promulgated in the 90s were found by most urologists to be, frankly, unworkably sensitive to the testimony of women, and outrightly rejected. Trapped in their 160 year-old and frankly demented antimicrobial superstitions, 21st Century urologists attempting to “treat” urinary disorders experienced by younger women, whether as a result of prior antibiotics-use or not, have frequently defaulted to the same misogynistic paradigms that prevailed in the dark ages of modern medicine. In other words, female genital anatomy itself was, once again, defined as the primary pathology for the complaints of women. “Look, toots - maybe if you hadn’t gone and put your bladder so close to your vagina, you wouldn’t be bothering me with all these imaginary problems all the time!”
Malone-Lee’s attempt to unravel these misogynistic tropes, therefor, and re-center the experience and testimony of the female patient in care for urinary disorder, should garner him praise. For younger female patients in the UK and abroad who have had their debilitating symptoms of urinary disorder dismissed by other urologists, he has been a lifeline; an advocate; and a knight in shining armor. When his clinic was closed from on-high after one patient experienced organ failure, nearly four thousand current and former patients petitioned in protest.30 Dr Malone-Lee has been a savior for women in the UK neglected by other urologists, even if an imperfect one. From one Amazon user review of his recently published text:
I was diagnosed with IC and my pain [levels] were so extreme, nothing seemed to be working and doctors refused to prescribe me opiates due to the opioid hysteria happening right now. They would not believe how bad my pain was while I cried my eyes out in front of them, they merely treated me like a drug seeker. I was very close to taking *permanent* measures that would stop my pain for sure.
My pain would be so bad that most of the day I couldn't even think straight, you don't really know what that is like until you go through it. It is not living, only suffering.
I was desperate to find an answer and I saw hope in Prof. Malone Lee however I could not afford to go to England for treatment. Eventually I was able to get antibiotics to treat my infection, and I was very lucky that just a 3 months course and my pain almost has completely gone away (some people may need a year or more).
No degree of statistical manipulation can dispossess Malone-Lee of the credit for the relief offered to this woman by his battle against urology-at-large’s habit of dismissing female patient reports of urinary distress.
But on the other hand, when not weighted for age, female patient concerns over under-treatment for urinary disorders have been completely eclipsed by alarm over over-treatment in the last two decades. Returning once again to the focus group study with which we opened this essay, concerns over having symptoms relegated to figments of the imagination, or being made to wait until Urine Culture results are in, are still prevalent among women, but only rank at the bottom of contemporary patient priorities according to the authors’ transcript analysis.

Given, once again, the suffocating existential anxiety which even “moderate” urinary pain or restriction are capable of inspiring, the fact that over-treatment ranks higher in the concerns of modern female patients is damning. So, as regards Malone-Lee’s attempt to correct for two decades of dismissing reported symptoms of disorder, it must be asked, why he is simultaneously so gung-ho for antibiotics?
Malone-Lee’s success, and his mistake, both lie in the same approach: Rather than using short-course, broad-spectrum antibiotics to attempt to sterilize the interior of the bladder, he favors long-term, narrow-spectrum courses that give the bladder lining time to renew and shed prior bacterial biofilms. These films are the “reservoirs” that many phage-enhanced strains of bacteria form, in response to quorum-sensing signals that indicate either monocultural abundance or sudden population collapse - and they constitute the key reason that antibiotics alone can never hope to return human microbiomes to health at all (instead, they only reset the field and allow for blind luck to do what it will).
Malone-Lee, in the end, remains trapped in the same 160 year-old error that strand the colleagues he wishes to attack: That urinary disorder must be exclusively caused by bacteria or human tissue, rather than an outcome of the departure from harmony among the two. In defining biofilms as the enemy that his antibiotic regimen must “overcome,” he fails to recognize what is staring him in the face: The problem is not the resilience of hardier bacteria, which can never be overcome, but the failure of more delicate bacteria to thrive and outcompete them.
While Malone-Lee’s approach is of indisputable value to the women who have had their symptoms ignored by other doctors, it is no substitute for a genuine advance in therapy that accomplishes true Urinary Microbiome restoration. Additionally, it can only be guessed whether this treatment regimen is throwing his patients’ other microbiomes into disorder, or whether it is reasonably easy for the Urinary Microbiome to actually be weened off of such persistent, pathway-targeted medication. Indeed, when Malone-Lee’s clinic was shut down in 2015, 199 of 221 current patients experienced a deterioration in symptoms - revealing the extent to which his therapy cultivates medical dependence, at least in the short term.31
And despite the accolades of the patients to whom he has previously offered relief, in recent years he has found his backwards, pro-antibiotic ideas roundly rejected by women in the UK, indicating that his work does not offer relief quickly enough for those who are in pain, whether he likes it or not. In response, he has taken to Twitter, where he joins an echo chamber of other urologists who are mostly ignored by the users they have arrived to lecture. Here, he spends his days incoherently imploring the women who are not seeing his tweets to cease leaping at experimental surgical cures, and simultaneously, to cease gainsaying experimental vaccines.
Still, Malone-Lee is a sympathetic figure. His sincere devotion to the well-being of his patients pervades his work. His adamant faith in low-and-slow antibiotic regimens is inflected by a recognition that at the turn of the century, something went deeply wrong with the West’s treatment of urinary disorder. And his dismay over the flocking of young women suffering from recurrent urinary disorders to radical surgeries - namely fulguration, a horrifyingly microbiome-destructive procedure designed to burn away tumors in the bladder lining - is compellingly sincere.
If Malone-Lee is trapped in the sterilization fallacy, our avatar of hope for actually rescuing the field of urology from its own hostility to the female Urinary Microbiome will therefor take the form of Dr. Rachel Rubin. Here, once again, we find a urologist who has plunged into social media to call back the women fleeing the castle of mainstream medicine, only to become mired in a professional echo-chamber. Yet although this gives her Twitter feed the feel of a spambot posting to other spambots, the spam itself offers positive signs of a possible correction to the Original Sin of Urology. Rubin, and some of her peers, seem to actually be on to something:

Although Rubin seems reluctant to attack the core mistake itself - the hostility toward bacteria in the urinary tract - her Twitter feed evangelizes one of the most promising contemporary frontiers of treatment for women suffering from or susceptible to urinary disorder: The application of vaginal estrogen creams.
There is, of course, still one substantial line of criticism against this sudden, exciting “discovery” of the potential for manually-applied estrogen creams to alleviate genitourinary disorders among women: It comprises a frontier or research which is three decades old.32 Vaginal estrogen creams were already showing promise in the 90s, before the abandonment of the Kass Threshold which possibly led to an inadvertent plague of overmedication among the elderly. Using Rubin as our example of a potential for urology to correct the mistakes of the past, also highlights once again the depths of ignorance and neglect prevailing among the rest of her field.
Still, the promotion of estrogen creams holds great promise, at least for post-menopausal women. Returning to the landmark results of the “Bladder is Not Sterile” study from five years ago, it seems that the promotion and nourishment of estrogen-philic Lactobacillus strains within the Urinary Microbiome, specifically, may be the key to preventing and alleviating many, if not most or all, incidences of urinary disorder among women. If estrogen creams are indeed the next frontier in urinary disorder therapy, a golden age of post-menopausal patient care may be just around the corner.
Yet will these benefits extend to younger women, whose urinary disorders may be the result of incredibly complicated interactions between synthetic fabrics, other environmental toxins, and their genitourinary microbiome? It remains to be seen. Discovering an individualizable path to Urinary Microbiome restoration may prove a vast and difficult research challenge; one that still takes decades to bear fruit.
But at least urology could begin to try.

The Revolt of Women
Despite the dismal prospects for further research which faced the newly-discovered Urinary Microbiome in 2016, progress in the last 5 years has been encouraging. A paper released earlier this year offers an overview of the intervening research. Entitled “Urinary Microbiome: Yin and Yang of the Urinary Tract,” the paper offers hope and optimism where a glimpse into the past can encourage only dismay.33 It is beautifully-written, and littered with references to other promising studies. Within the text of the “Yin and Yang” paper, the pending progress in our understanding of the human microbiome still seems as vast and imminently history-altering as it did back in 2008.
Moreover, if our review of the attempt by individual urologists to co-opt the Revolt of Women against urology has painted a picture of medical hopelessness, it has only added cause to believe that a true revolution in treatments of urinary disorders is inevitable. For, so long as the farcical myth that the flourishing of bacteria in the urinary tract constitutes a state of “infection” is allowed to prevail, no progress is possible: And so long as the intuitive revolt prevailing among Western women of all ages, which insists that their genitourinary anatomy is not a medical flaw, but a biological wonder, wages war against that myth, a final shift toward progress in modern female urinary health is nothing short of inevitable.

Patient comment from Scott, V. et al. “Fear and Frustration among Women with Recurrent Urinary Tract Infections: Findings from Patient Focus Groups.” (2021.) The Journal of Urology.
ibid.
I suspect the yearly cost of care is actually higher, despite the drop in prices for antibiotics, given that costs two decades ago were already almost just as high. But all sources give values consistently near the ~$2 billion mark.
The trend in the first decade of the millennium in the US was a ~50% increase, if we use hospitalization costs as a proxy for overall care costs. See: Simmering, J. et al. “The Increase in Hospitalizations for Urinary Tract Infections and the Associated Costs in the United States, 1998–2011.” Open Forum Infectious Disease. The authors, however, suggest that this is due to higher sampling - i.e., that less severe UTI cases were resulting in hospital visits, though this conclusion is arrived by a bizarre comparison with other hospitalization cost increase trends. Additionally, they suggest that the rise in admissions is driven by antibiotic resistance, rather than by the abandonment of the Kass threshold.
Another view of the rise in urinary disorders in the West is provided by the somewhat enigmatic chart offered by the UK’s National Institute for Health and Care Excellence (acronym-ed as “NICE,” rather than the more accurate “NIHCE”), reprinted by James Malone-Lee (and not available outside of the UK) seems to indicate that visits had nearly tripled from circa 1998 to 2014. See: Malone-Lee, J. “Confronting The Urinalysis Tyrant.” (2021, March 9.) BJGP Life.
I found it odd that no more recent annual cost trends seemed to be available for the US; but I was satisfied that further precision was not required in order to intimate roughly a doubling, at minimum, in incidences of (mis)treatment for UTIs in the last two decades.
See Mayo, A. “Amazon delivery drivers say there's a 'giant war' between them and the company as they struggle to meet package quotas.” (2021 August 5.) Business Insider:
"I resort to peeing in bottles, and women urinate through funnels into bottles, just so I'm able to get done with my deliveries," Valerie G, a driver for one of Amazon's Delivery Service Partners (DSP), told Insider. "Those conditions are extremely unsanitary, and we are there with all those packages and our own urine and bodily fluids. That's unsanitary for the customers receiving the packages."
Even if the likely relative delicacy of the Urinary Microbiome might warrant more cautious thought.
A necessary linguistic simplification. Potentially excessive surgical screening has “just come to light.” Clearly excessive elderly care screening has been observed for over a decade.
Testimony from “Polly” in Boseley, Sarah. Devlin, Hannah. “'In pain all the time': will there ever be a cure for chronic, life-changing UTIs?” (2019, February 20.) The Guardian.
Almost more ridiculous than the fact that the Project left out the urinary tract, is the omission of the respiratory tract!
Thomas-White, K. et al. (2016.) “The bladder is not sterile: History and current discoveries on the urinary microbiome.” Current Bladder Dysfunct Reports. 2016 Mar; 11(1): 18–24.
The presentation offered two years earlier, involving some of the same authors, is Hilt, E. “Urine is Not Sterile: The Urinary Microbiota of Overactive Bladder Patients.”
However, a dip back into my bookmarks in September led to re-encounter with an even earlier study acknowledging the urinary microbiome, that I had saved and forgotten.
See: Lewis, D. et al. (2013.) “The human urinary microbiome; bacterial DNA in voided urine of asymptomatic adults.” Frontiers in Cellular and Infection Microbiology.
Zasloff, M. “Antimicrobial Peptides, Innate Immunity and the Normally Sterile Urinary Tract.” (2007.) Journal of the American Society of Nephrology.
(Thomas-White, K. et al.)
(Patient comment from Scott, V. et al.)
(index link anchor)
See Orenstein, R. Wong, E. “Urinary Tract Infections in Adults.” (1999.) AFP Journal.
Shenoy, E. et al., “Prevalence, Costs, and Consequences of Low-Value Preprocedural Urinalyses in the US.” JAMA Internal Medicine.
IBM’s marketing material for MarketScan is elusive about how many Americans are actually included within their ongoing dataset. At times (including on the current site) it alludes to a figure over 200 million, but the real-time figure (offered in the document linked by the study authors - https://www.ibm.com/downloads/cas/0NKLE57Y) for 2017 is much lower:
In the most recent full data year, MarketScan databases contain healthcare data for more than 43.6 million covered individuals— large enough to allow creation of a nationally representative data sample of Americans with employer-provided health insurance.
The commercial and Medicare datasets are only a portion of these, and the marketing materials do not offer a discrete value for the patients included within. On the other hand, surgery rates for the patients within these sets may be higher than for other Americans; and rates of preoperative urinalysis might be quite higher (or lower) as well. Hopefully any potential biases are accounted for by our use of the AHRQ 2014 surgery rate, rather than the more outlandish figures quoted by other sources, and by our 50% discount for non-sampled surgeries.
See Steiner, C. et al. “Surgeries in Hospital-Based Ambulatory Surgery and Hospital Inpatient Settings, 2014.” Agency for Healthcare Research and Quality.
Total surgeries for 2014 alone are given as 21,777,800 (whereas “visits” corresponding to surgery number at 17,162,700). This is also the source for the claim that joint replacement is the second-most predominately non-emergency surgery. But it must be noted that gratuitous urinalysis preceding breast surgery is nonetheless rare:
The following procedures were among the most common invasive, therapeutic ambulatory surgeries:
Lens and cataract procedures (99.9 percent performed in AS settings)
Excision of semilunar cartilage of knee (98.7 percent in AS) […]
Inguinal and femoral hernia repair (91.9 percent in AS)
Incision or fusion of joint, destruction of joint lesion (80.5 percent in AS)
Operating room (OR) procedures of skin and breast (78.7 percent in AS)
Meanwhile, an alternate estimate for total annual surgeries in the US is given at https://stanfordhealthcare.org/medical-clinics/surgery-clinic/patient-resources/surgery-statistics.html - which claims the count for surgeries in 2009 was 48 million, citing CDC statistics which have since been relocated.
But there’s also the possibility that tons of urinalysis events didn’t, either! As regards the speculation that codes were mis- or non-entered (and therefor a greater portion of preoperative urinalysis events were, in fact, legitimately indicated), it’s really not so implausible, and would explain the higher prevalence of testing before joint surgery (which targets, besides athletes, the elderly) and spine surgery (which targets patients who might have already experienced the onset of urinary disorder symptoms as a result of catheterization). This would mean that preoperative urinalysis leading to antibiotic treatment is incidental to already-presenting symptomatic urinary disorder, and not actually very prevalent among asymptomatic patients. This traps us in a chicken-and-egg quandary: Is urinalysis being responsibly employed due the higher prevalence of observed urinary disorder symptoms among the elderly and paralyzed, or is the awareness of the prevalence leading to an irresponsible over-employment of urinalysis (which reinforces the expectation)?
So, let the record state that the annual gratuitous urinalysis rate calculation offered in this essay has been thoroughly caveated!
(Steiner, et al.) The crude value of 80% for annual in-category surgeries sampled by the MarketScan commercial and Medicare databases (and thus 20% for in-category surgeries not sampled, for which the gratuitous antibiotic outcome rate is discounted 50%) is derived from the following chart representing within-hospital-system surgeries:
The values for antibiotic treatment per category were reconstructed using pixel counts, leading to 303,987. The overall rate was thus 303,987 / 13,169,656 = .0231
1223466x.023+337833x.014+420773x.046+4403884x.024+1751905x.028+1416164x.041+243169x.017+930359x.012+309690x.01+123139x.064+1282003x.025+129584x.017+293527x.012+304160x.01 = 303,987
Deriving this value was no odyssey, but it was still a bit of work. Why wasn’t the antibiotic administration rate included in the study text? Why are the authors doing so little with all of their data? It’s not like access the study is currently free, you know. I paid $30 for it!
Yin, P. et al. “Urinalysis Orders Among Patients Admitted to the General Medicine Service.” (2015.) JAMA Internal Medicine.
(placeholder for lost citation)
Pety, L. “Risk Factors and Outcomes Associated With Treatment of Asymptomatic Bacteriuria in Hospitalized Patients.” (2019.) JAMA Internal Medicine.
Urinalysis tests were ordered for almost all observed patients, but the study does not include info on outcomes for other patients who may have had a positive urinalysis test without a positive Urine Culture. However, it does provide a value for how many Urine Culture tests had “abnormal urinalysis” as the documented reason for ordering the culture: 666.
(Patient comment from Scott, V. et al.)
(index link anchor)
See https://www.amazon.com/Cystitis-Unmasked-James-Malone-lee/dp/1910079634/. Additionally, for a condensed summary of Malone-Lee’s mission see: “Confronting The Urinalysis Tyrant.” (2021.) British Journal of General Practice Life.
“London Trust reverses decision to shut LUTS clinic.” (2015, November 20.) Leigh Day.
Swamy, S. et al. “Cross-over data supporting long-term antibiotic treatment in patients with painful lower urinary tract symptoms, pyuria and negative urinalysis.” (2019.) NIH National Library of Medicine.
See Raz, R. Stamm, E. “A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections.” (1993.) New England Journal of Medicine.
Perez-Carrasco, V. et al. “Urinary Microbiome: Yin and Yang of the Urinary Tract.” (2021.) Frontiers in Cellular and Infection Microbiology.
I have to say I'm surprised at the small number of comments, especially after almost a year.
I read this with great interest. I'm old as dirt now, but in the late 80s and early 90s I had recurring UTIs. I don't remember ever getting tested. But if you've never had a UTI you just don't know how all-encompassing the discomfort, even though not painful per se, can be. So my doctor would prescribe me an antibiotic. This led to several years of bouncing back-and-forth between 'bladder infections' and yeast infections. It was fairly obvious that treatment for one would set off the other.
When I told my doctor about this, he (of course it was a he) casually waved it off with a "Yeah, that happens."
Aside from the cavalier attitude which annoyed me even then, I don't really blame him; as you point out, they didn't know any better in those days and he just wanted to shut me up with a prescription. I have to say the antibiotics always granted fairly prompt relief, so I figured he knew what he was doing.
It's really good news that somebody finally may be figuring some of this out. Overuse of antibiotics has a lot more to answer for than just resistant bacterial strains. I've spent the last decade focusing on the health of my interior bugs.
Just skimmed this so far, look forward to reading the whole thing. My mother was treated so irresponsibly for UTI that some types of antibiotics no longer work for her. This scares me because as she gets older and will see more health issues, it decreases the pool of antibiotics they will be able to use for her.