A new paper has come out which fits the mold of, “Paper suggests SARS-CoV-2 destroys the immune system like HIV” — it has stirred up a lot of attention on twitter. But, the paper rests on, and merely seeks to theorize about the mechanism for, a profound misunderstanding of what it takes as the suggested link between SARS-CoV-2 and HIV; akin to a paper trying to figure out why the common cold causes AIDS (which it doesn’t).
Background (optional read)
Since 2020, several papers have been uploaded or published which can be read to suggest that SARS-CoV-2, the (usually) cold virus which causes (sometimes) acute, severe Covid 19 or Long Covid, possesses similarities with HIV in either form or function. These have occasionally fed into speculative posts among lay commentators, within the Covid-skeptic space, amplifying the attention given to these papers.
The papers which have been amplified, generally, rest on taking something that isn’t especially remarkable about SARS-CoV-2 and discussing it in a way that fosters such later hyper-attention. Such as, that the spike protein shares epitopes with one or two unimportant entries out of the entire, vast library of HIV sequences ever performed; or that coronaviruses might be absorbed into immune cells via receptors designed to generically react to viral proteins; etc. In other words, none have been convincing of a reason to worry that “Covid is AIDS” is a likely problem.
For comparison, another human virus, Hepatitis B, is related to HIV:
The retroviruses that causes AIDS and the Hepadnavirus that causes hepatitis B share a common ancestry (see Table 1) based on homology of important nucleotide and amino acid sequences. There are shared features in their genomic organizations, unique reverse transcription of nucleic acid during the replication cycle, and striking similar modes of transmission. The Hepadnaviruses may be simplified retroviruses that might have evolved through genetic deletion and modification from a primordial retrovirus. The two viruses differ in that HIV integrates into the host cell genome and targets the immune system, while hepatitis B targets the liver.1
But the Hepatitis B virus does not cause AIDS; so extensive homology with HIV is obviously not sufficient. It certainly therefore isn’t alarming if, between another virus, SARS-CoV-2, two or three epitopes might be similar with HIV. Meanwhile, SARS-CoV-2 does not integrate with the host cell genome in a wholesale, in-tact, and reversible manner as part of the replication cycle. And when it comes to the question of targeting immune cells, this too wouldn’t be sufficient by itself to cause alarm — for other viruses, like Measles or CMV, do this as well, without causing AIDS. Besides, it has only been hinted in these various papers that perhaps SARS-CoV-2 winds up infecting immune cells at a low rate (but only perhaps), not that it is even like Measles in terms of “targeting” the immune system.
We can thus describe the motif of these inquiries as, “Could SARS-CoV-2 be 1/1000 as similar to HIV as Hepatitis is?”
The new paper
The new paper differs from this trend by directly attaching the alarmist insinuation that “Covid is AIDS” to the title, and by being even less convincing than what has come before:
The thesis for “why SARS-CoV-2 might cause AIDS,” however, rests not even on the on a “Could SARS-CoV-2 be 1/1000 as similar to HIV as Hepatitis is?” inquiry, but instead an amazing confusion of the transient immune cell depletion of acute infection with long-term cell depletion:
Lymphopenia as a major immunological abnormality that occurs in the majority (72%) of severe COVID-19 patients, can cause general immunosuppression facilitating viral persistence […]
Lymphopenia, a low amount of T and B Cells, is only a “major abnormality” if it occurs without acute infection, as a long-term baseline; it is completely normal, on the other hand, during an infection. Almost any infection will result in leukopenia, which is a lowering of all white blood cells, which includes T and B cells. I need only quote from wikipedia:
Low white cell count may be due to acute viral infections, such as a cold or influenza.
The new paper is describing the fact that people with acute SARS-CoV-2 infections have low white blood cells as evidence that they have suddenly developed AIDS. As opposed to the more parsimonious conclusion that they, yes, have an acute SARS-CoV-2 infection, which is like any infection in this regard, such as common colds.
The white blood cells normally present in the blood will “go to work” during an infection; they are not in the blood anymore because they are wherever the infecting-thing is, trying to remove it, so that you do not die. The resulting short-term lack of them in the blood during an acute SARS-CoV-2 infection is not abnormal.
From this profound mistake, the authors go on to their thesis for just why SARS-CoV-2 “causes AIDS”; which we may skip, because it is only an unconvincing and computer-modeled argument for “Could SARS-CoV-2 be 1/1000 as similar to HIV as Hepatitis is?” Who knows, maybe! It shouldn’t worry us.
So what happens to immune cells long term after infection with SARS-CoV-2?
As acute immune cell depletion is common with any infection, we should only start to worry if SARS-CoV-2 is causing a long term “baseline” of leukopenia or specifically of the depletion of CD4 T Cells.
A recent paper offers a profile of the immune cell counts of 106 individuals 10 weeks and 10 months after infections which occurred in 2020, before the vaccines:
It is nice that this has just arrived to supplement a new discussion of the “Covid is AIDS” controversy, even if strange that outcomes from 10 months after the very earliest infections with SARS-CoV-2 (not focused on Long Covid patients) should only just now be published. How many trillions of dollars have been spent in responding to and researching this virus?
The study examines the immune cell counts of recovered individuals with mild or severe infections with SARS-Cov-2, compared with a set of uninfected controls sampled in parallel. The controls are a nice touch, because they rule out measurement artifacts or weird effects from lockdowns (e.g. reduced exercise etc.). Not included in the comparison are infected individuals who still have high antibody levels at the 10 month mark, as these may have experienced a reinfection. So, the resulting sample of 106 should only represent the long-term effects of a single first-time infection. Only 14 of these were considered to be experiencing long-term symptoms.
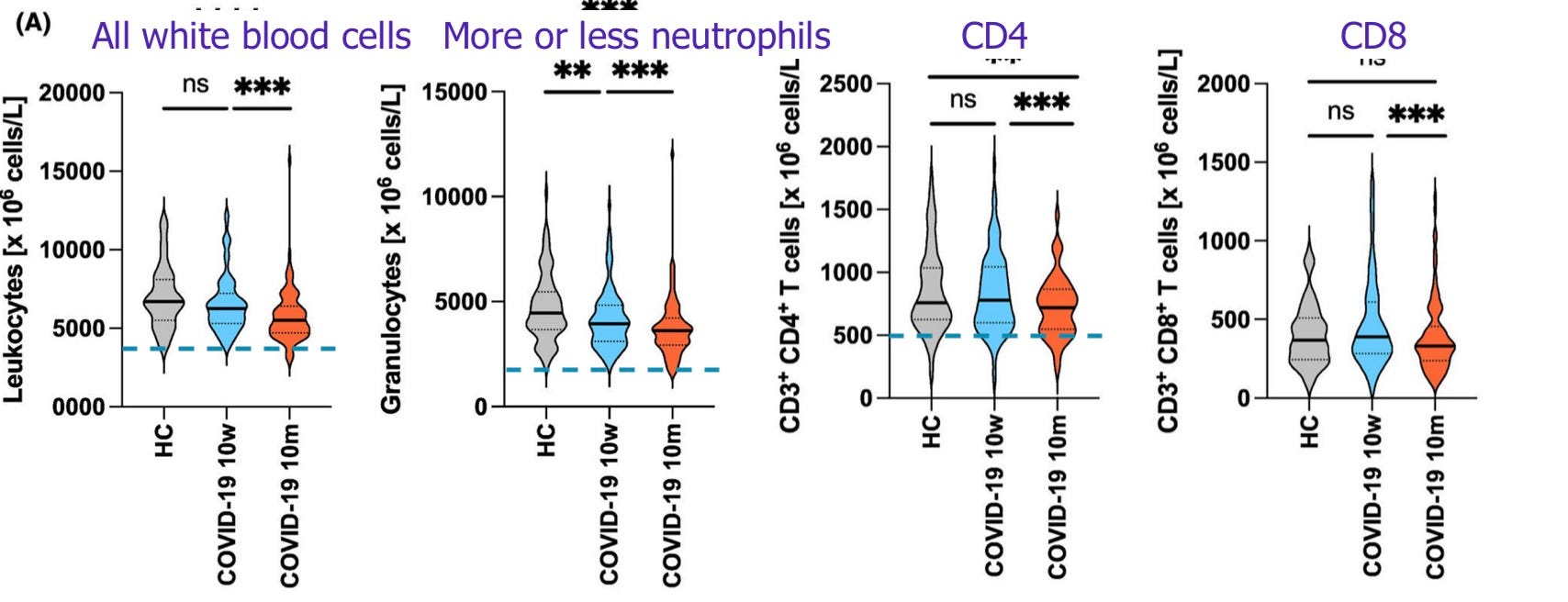
Kratzer, B. et al. results:
Indeed, there is a long-term depletion of white blood cells, especially neutrophils and some types of T Cells, at month 10. As neutrophils are the most abundant white blood cell, they drive most of the overall depletion.
However, the majority of recovered individuals are still within normal ranges for the relevant types of immune cells and for overall cells. Few have counts that qualify as leukopenia, neutropenia, etc.
CD4 cells specifically are only reduced at 10 months in a minority of recovered, and somewhat elevated in others.
Some of the results. “HC” are uninfected controls with generally similar background health characteristics as the recovered cohort. Dashed lines represent thresholds for below “normal”.
In conclusion, infection with SARS-CoV-2 does lead to some changes in immune cell populations, and this includes a reduction persistent at 10 months of circulating immune cells which remains within the normal, healthy range.
Changes to immune markers are not unique to SARS-CoV-2, and have been observed after other infections and vaccines — so called “non-specific effects.”2 They are not by themselves suggestive of immune dysfunction, immunodeficiency, or AIDS.
I have been feeling guilty about not reading this properly ever since it came out. I did read it for the conclusion. The problem is that covid really does form reservoirs in the brain and other organs and people don't seem to clear it, so perhaps these immune system recoveries are not permanent. Also I am seeing loss of mental capacity in people I know, and when I check the obits in the area I grew up there are so many people dying in their 60s, and that is not normal (they are not drug deaths; these are people with jobs and families and functional lives; they are cancer and heart disease deaths in startling numbers). So I am still doing my best to keep my household from catching covid; so far so good. We can't spare the IQ points and I don't want some weird ailment like my mom's sudden pancreatic insufficiency; I have never known anyone with that before.









Covid does not result in AIDS...
But Covid Vaccines aka The Rat Juice --- most definitely results in VAIDS
I have been feeling guilty about not reading this properly ever since it came out. I did read it for the conclusion. The problem is that covid really does form reservoirs in the brain and other organs and people don't seem to clear it, so perhaps these immune system recoveries are not permanent. Also I am seeing loss of mental capacity in people I know, and when I check the obits in the area I grew up there are so many people dying in their 60s, and that is not normal (they are not drug deaths; these are people with jobs and families and functional lives; they are cancer and heart disease deaths in startling numbers). So I am still doing my best to keep my household from catching covid; so far so good. We can't spare the IQ points and I don't want some weird ailment like my mom's sudden pancreatic insufficiency; I have never known anyone with that before.