


NorCal pregnancy study, etc.
Brief remarks on two unremarkable papers!

A new, but already outdated study purports to demonstrate that infection with SARS-CoV-2 leads to increased risk of negative outcomes in pregnancy. The actual numbers look reassuring. Not that they will be reported as such.
Meanwhile, another gaff from “our side.”

And Statistics
Another day, another manipulative pregnancy outcomes study that obscures all the raw data and makes it impossible to figure out what’s going on. Oh, wait - never mind! Today it’s a manipulative pregnancy study that makes all the data quite easy to absorb.1
For pregnant women delivering at Kaiser Northern California between March 1 2020 and March 16 2021, those who were positive for infection with SARS-CoV-2 sometime during pregnancy didn’t seem to have very different outcomes. This is unsurprising since:
Multi-state data that includes California, for all of 2020, which has been available from the CDC since June of last year, says the same thing.2
Proportionately, environmental air quality disparity shouldn’t be as much of an issue in a NorCal health system as it is for the South (where lack of access to coastal air is one of the defining markers of economic inequality3).
There were very few cases, and only one “wave,” in NorCal during the entire study period, which makes it more likely that positive tests would be “true false positives” (no actual infection) vs. “with, not from” false positives. The former would conceivably make results appear more favorable for the infected group; the latter might punish them for being PCR-screened during admission for unrelated complications. So in essence, the study design is likely to under-estimate the risks from infection, if anything.


Despite the second bullet, we could expect some skewing for environmental and other income-related factors which wouldn’t spare white residents entirely but would probably still skew the qualities of “PCR positive” as well as symptomatic or severely ill toward Hispanic and Black pregnant women.
And so, neatly reflecting all these design accidents, our “With SARS-CoV-2” group is both small, 52% Hispanic, and 70% high-neighborhood-deprivation score:

This, alone, seems likely to account for much of the observed difference in outcomes absent any fancy mathematical adjustments. Here I have noted the otherwise not-displayed values for outcomes that occurred before a positive test, as they are a bit interesting:
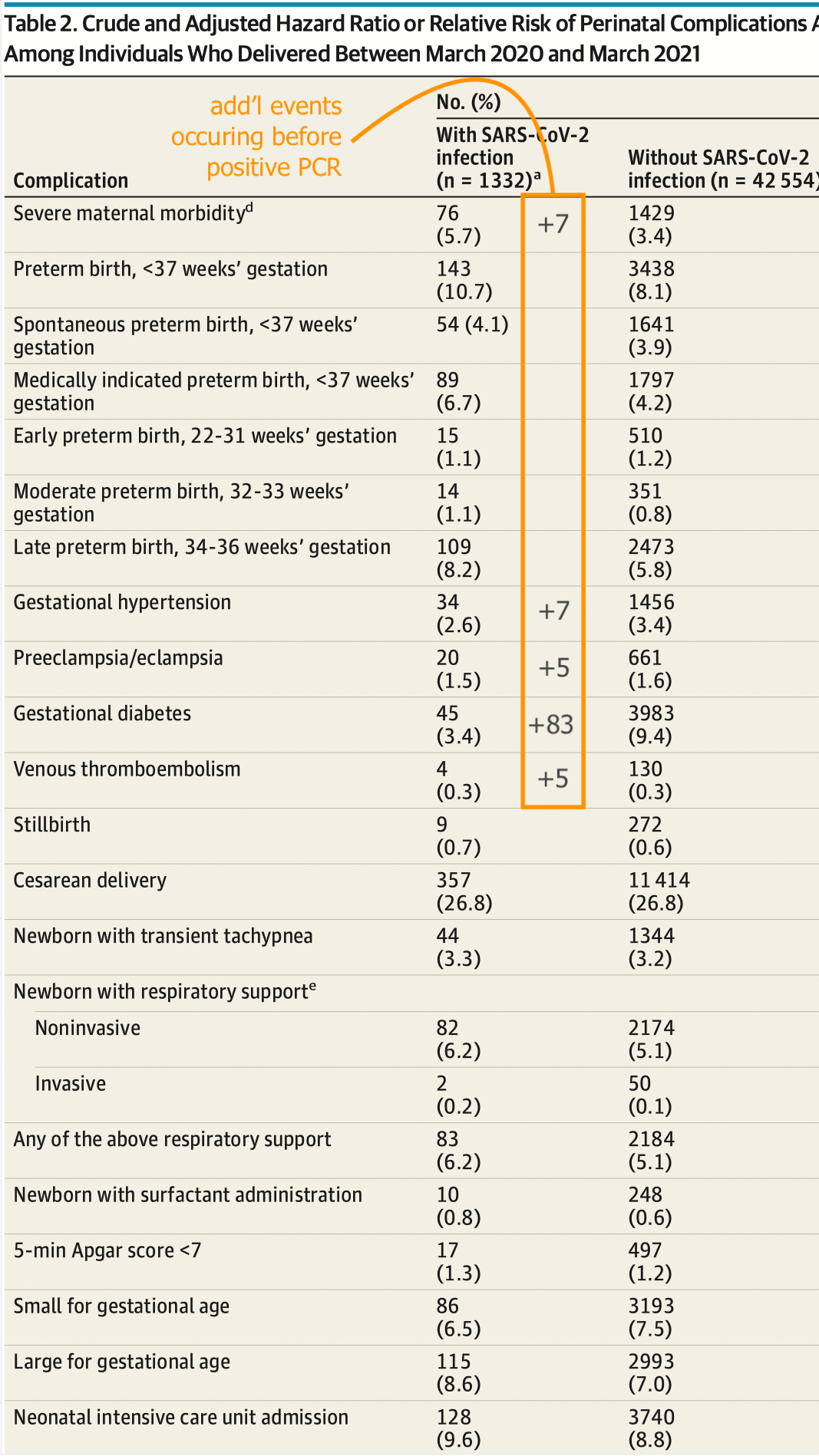
Including the values for outcomes that precede positive PCR test explains the otherwise implausible low rate of diagnosed gestational hypertension and diabetes. It also reveals a potential signal for a hidden increase in venous thromboembolism; though the absolute number of events for this outcome would remain in the single digits.
With the possible exception of “severe morbidity,” none of these results seem patently alarming when the skew toward lower income is kept in mind. As for said morbidity, respiratory distress drives almost all of the “extra” percentage of outcomes vs the non-infected group:
Subtracting those 2.1%, the “no severe morbidity” rate becomes nearly equal. And while a 2.1% rate of respiratory distress might be concerning on its own, it nonetheless puts the overall rate of “severe morbidity” in context: Rates of all other severe outcomes are quite even, aside from a .5% uptick in sepsis.
One other potentially concerning result appears in the supplemental materials, in the comparison between early and late-pregnancy diagnosis of infection. Here, the results display an uptick in stillbirths occurring some time after an early positive test. However, this could merely be a form of cutoff bias, especially given the small absolute count (6 stillbirths; see footnotes4).
And so now we might dust our hands and say, “All done.” There doesn’t seem to be anything particularly worth discussing in this paper. It doesn’t show any alarming results, and merely reinforces already-available data.
Or Not
But of course we’re not done, because of course the authors aren’t just going to publish results that don’t support encouraging pregnant women to take an experimental gene-based medicine!
So instead, they completely distort their own results by reporting in terms of hazard ratio for all pre-delivery outcomes, even though nothing in the study design supports such a decision (since only completed deliveries are being measured anyways).
By doing so, the authors can show not “the risk of something happening at all during pregnancy,” but “the risk of something happening divided by the portion of time spent between positive test and outcome, which is a fraction of overall duration of pregnancy, and so arbitrarily multiplies the risk.”
Here, I’ve highlighted only those values for which this design choice results in particularly absurd outputs:

Hazard ratios are for studies following participants until death, when it makes sense to score outcomes in a manner other than “how many people does this happen to?” (so that the effect of prolonging life can be quantified). In the context of 43,886 completed pregnancies, it’s a nonsensical metric. All that matters is whether something bad happened or not.
And yes, as we saw in the earlier version of Table 2, the fact that infection strikes in the middle of pregnancy can lower the apparent rate of outcomes after infection, by “shielding” the infected group from early events. But the authors had the values for those early events; and those values flatly refute their absurd mathematical penalty (especially since that penalty may only reinforce a “with, not from” bias anyways!).
I find it very hard to offer a neutral assessment of the authors’ decision-making here. They could see through the invalidity of their mathematical adjustment, and yet they went with it anyway. And as a result, they created a bumper crop of alarming calculations that could be used to frighten and confuse lay readers, were they to get into the hands of a less-than-scrupulous press.
But naturally, the mainstream and medical press coverage of this paper will be careful to point out the misleading nature of these reported results. From Victoria “Literally Refers to Parents Who Dare to Raise Their Children According to Their Own Medical Judgement as ‘Pro-Disease Advocates’5” Forster:

Ah. Great.


I’ll Trust Whatever I Want to
Ah, but the MSM-aligned science journalists aren’t the only ones serving up flawed study reviews, today. If the reader has already had the misfortune to slog through the flawed review coming from “our side,”7 the notes below may help to clear up confusion created by the misrepresentation.
The study in question is also quite outdated, so I’ll be brief:8
Events which are attached to a corresponding value for person-days essentially function as a rate. Thus, increasing the number of person-days cannot increase the rate calculated by another denominator. So if rate A is higher than B, and increasing person-days results in making rate B higher than A, you have messed up your math. The same holds for B+C. As long as rate B is lower than A, adding it to C cannot make C higher than A when it was not before.
If B is higher than C, but lower than A, than rate B+C will be lower than rate A+C. So any combination of B+C is still a better trade than A+C. So B protects against the normal exposure risk of A for however many person-days are spent inside of it. There are more bullets in the “foxhole” than in the path to the “bunker.”
That’s all really intuitive. I don’t understand how one messes that up.
Bar-On, et al. used shell-game-esque definitions in their first report on post-booster outcomes in August.9 In both cases, the studies are more-or-less transparent with actual infection rates, but seem coy about severe outcome rates in the immediate wake of injection. So the likely reason they pick these weird windows is to hide a signal for Adverse Events. Doesn’t seem like some big mystery.

Ferrara, A. et al. “Perinatal Complications in Individuals in California With or Without SARS-CoV-2 Infection During Pregnancy.” JAMA Intern Med.
Last reviewed in “Updated Pregnancy Snippet.”
Whereas a substantial portion of low-income residents in NorCal reside in San Francisco, Alameda, northern San Mateo, or Santa Clara county, where the air is more or less great.
Since the study is only measuring outcomes among completed pregnancies, and stillbirths may precede normal deliveries by many weeks, the true denominator of eventual live births is incomplete for both groups. Measuring outcomes for “<21 weeks” additionally adds a penalty based on the end-of-window skew in cases created by the winter 2020/2021 wave.

(link anchor)
“el gato malo.” “NEJM proves that covid vaccine study methodologies are rigged.” (2022, March 21.) bad cattitude.
The tagline, “sometimes a study winds up proving something far more interesting than it intended,” is more or less the only valid conclusion in the essay.
One more item on the plus side: Judging from the port layout, the “Would you look at that” meme cat is operating a mid-2012 13” MBP. Same as my own machine.
Bar-On, Y. et al. “Protection against Covid-19 by BNT162b2 Booster across Age Groups.” The New England Journal of Medicine.
I consider The Cat to be mostly a muckraker (although I'm not positive that's the word I'm looking for). I've caught a few things where he misrepresents (or leaves out key information) on a subject or an event in order to agitate. But it does get lots of comments and it does keep readers agitated so - success! 😜
Thanks for pointing out the flaw in Gato's post. How did he possibly make that mistake???
It makes me worry about him a little.
What matters in this kind of analysis is the comparison between the pre booster rate (double vax) and the post-booster-pre-effect rate ("early prebooster"), which in this case are basically the same rate. So there's really no effect here. Who knows what's going on in the other days they excluded, that is a little fishy, but it's unlikely to be so bad as to make the shots ineffective... perhaps less effective though.
A fair way to calculate this would probably add the raw count of excess pre-boster events, that are over and above the pre-existing doublevax rate, to the raw booster counts, and use the original denominator for boosted days. That we we only put the extra events on boosting's tab.
A few people in his comments section also called this out.
I hope he retracts it, he retracted another post recently, although I didn't actually see a problem with it (I didn't look too hard though).