(Note that I have mastered the art of making posts’ subtitles the title, as promotes engagement on substack)
I’ve been continually, simultaneously meditative and distracted for the last few months, as one does when an existential distraction (global, radical, potentially mandatory medical experimentation) recedes into the horizon. Now I would like to set some of these stray thoughts to written word; which will likely result in a series of brief and untimely posts on niche topics. Here is one.
From the comfort of umbrellas
Pro-narrative nuance-monger, and therefore arch-rival of everyone, Zeynep Tufecki, continues from time to time to flaunt an unrepentant attitude toward mainstream over-reaction to the virus from 2020 - 2021. In case the reader somehow forgets, this overreaction includes months (or years for some) of panicked sheltering from life; global, radical, potentially mandatory medical experimentation on the human race; and no small measure of secondary social fission.
At the turn of the month this wont for unrepentance manifested in the following hot take:
I highlight this rhetorical barb because it is so easy to point out the logical flaw here; Zeynep is engaging in mere sophistry. To see why, imagine for example that a town locks all its children into a basement for two years out of a mortal fear of… the rain. This imprisonment only ends upon the pretext of the discovery and deployment of a “solution” to the rain… rain-coats and umbrellas. The pro-imprisonment lobby, if criticized retrospectively, can cosset itself with the assurance that critics are minimizing the danger of the rain to children from the “comfort” of rain-coats and umbrellas. But this wouldn’t mean anything.
Or if the threat were mind-control beams, and the remedy were tin-foil hats, the same rhetorical ploy could be used to defend fear of mind-control beams. And so on, with any quaint allegory one could dream up. Ultimately the remedy, whatever its virtues, does not inherently determine anything about the scale of the problem or the appropriateness of the (pre-remedy) reaction to the problem one way or the other. This is obvious.
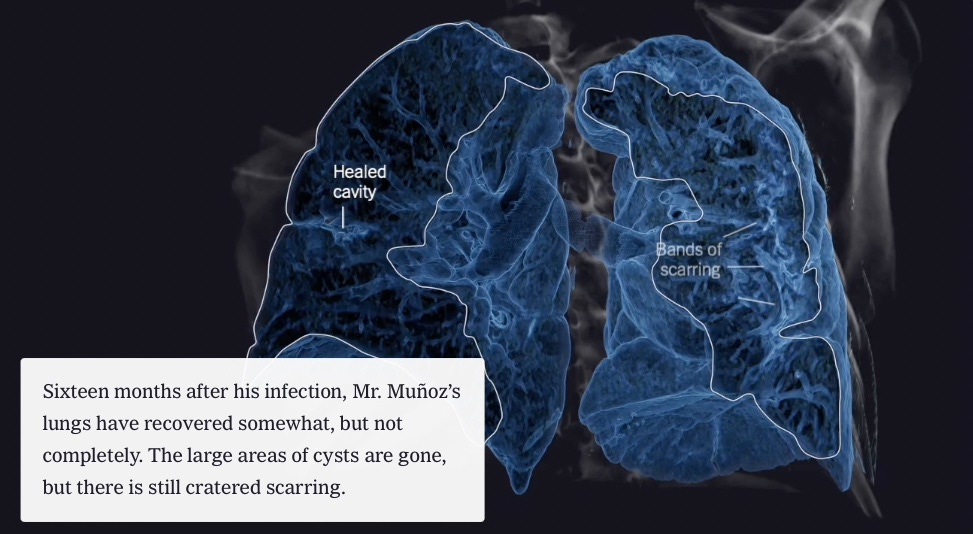
This is not to say that Zeynep’s volley of sophistry lacks a foundation in the concrete. Specifically, her prompt is the recent, computer-animation rich New York Times article highlighting three cases of extreme lung devastation in non-elderly severe Covid patients: A pregnant women near delivery and a middle-aged man in 2020, and a 30-something working man who hadn’t gotten around to vaccination in 2021, in increasing order of severity.
Nothing is enviable about these outcomes, to say the least, but (non-elderly) people get mortally or critically ill with lots of things at some scale. Infections go bad; lives get derailed. It happened before SARS-CoV-2, it still happens in our allegedly “comfortable” post-lockdown times. It will always happen.
And… it’s not overwhelmingly clear that the Covid vaccines substantially reduced such rare negative outcomes in the non-elderly to begin with. Suppose for example that severe efficacy in these lower-risk groups was 80%. So now 1 in X thousand instead of 5 in X thousand mid-30s welding inspectors experience the fate of Mr. Muñoz? This is the “comfort” that justifies shutting down the world to wait for?
Are we even really any better off?
For the non-elderly, far more common than severe infections with rampant lung destruction was the specter of prolonged non-recovery from infection, i.e. Long Covid. Here another pro-narrative figure whose output is nonetheless occasionally rewarding, Eric Topol, still casually and dogmatically tosses out claims of vaccine efficacy in absence of any clear evidence, as in this example from two weeks ago:
To underscore, all of the participants of this study were unvaccinated, which takes out the potential confounder impact of Covid vaccines. There are ample studies to tell us that vaccination helps protect against Long Covid, such as the prospective one published this week, which also confirmed the risk of reinfection for subsequent Long Covid.
Having followed the issue for over a year, I cannot agree that there are ample studies telling us any such thing; and in fact there are many that seem to argue little benefit.
Take the fresh-from-the-oven example Topol has cited — Thaweethai, et al.:
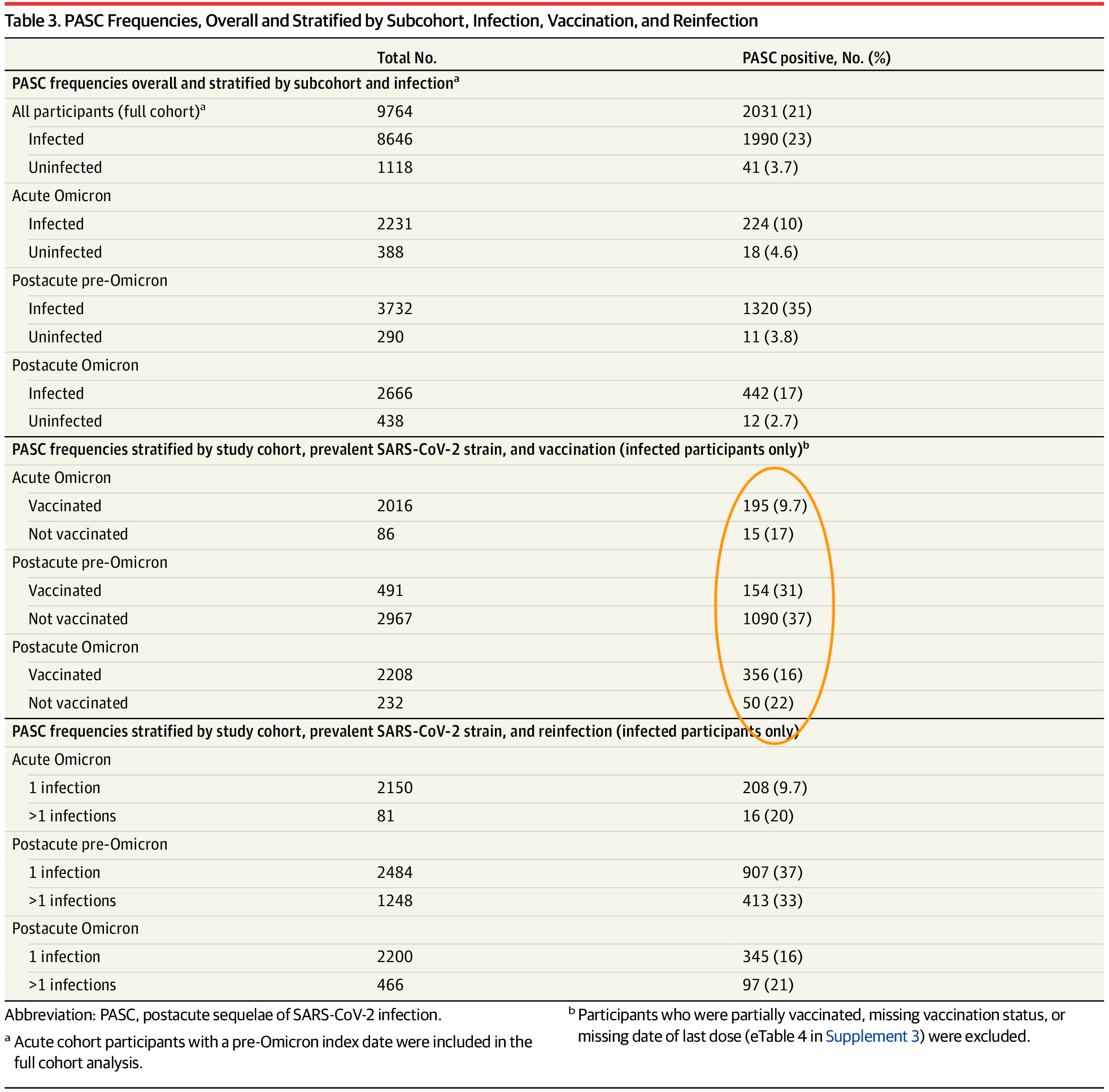
Unlike most pro-vaccine-Long-Covid-efficacy studies, Thaweethai, et al. is careful not to compare vaccinated “breakthrough” infection outcomes with outcomes before the vaccines were available, which choice (made on several other studies purporting to show a wonderful effect from vaccination) confounds matters by over-sampling early, severe infections in the era before widespread testing. And so the results — how many infected study participants go on to match the symptom clusters they develop to help distinguish likely Long Covid cases from background health problems — are simply not very impressive.
“Post-acute” refers to subjects infected before enrollment; a bias for PASC (people experiencing lingering symptoms being more likely to volunteer) may exist regardless of vaccination status. Regardless of this bias and a million other unknowable variables, we have to take Topol at his word — this is the amazing “help to protect” the vaccines will grant recipients. Instead of just-over 1 in 3 experiencing PASC before Omicron, it will be just-under 1 in 3. Maybe they will halfway-protect with Omicron (though it would be helpful to know if PASC-positive unvaccinated in the Omicron sets were reinfections, which means their symptoms might have been driven by the original infection anyway). 50/50 protection! — Do you feel lucky?
More impressive results on Long Covid efficacy hale from an obscure paper out of Texas — Messiah, et al., which looks at outcomes in children seroconverting for N protein in periodic antibody tests.1 Details aside, this paper looks like what would be expected if the Covid vaccines were actually reducing most of (already rather low rates of) Long Covid in kids.
Potential bias from spanning pre- and post-vaccine eras notwithstanding, I only bring this finding up as context before predictably, irresponsibly highlighting an anecdote in the opposite valance. Consider this case report of total apparent vaccine failure:
Patient 1 and Patient 2 are two sisters, 13 and 11 years old, respectively, previously vaccinated with two doses of mRNA SARS-CoV-2 vaccine. They got a mild SARS-CoV-2 infection in March 2022 when no restrictions were applied in Italy, masking was not mandatory anymore, and Omicron was the prevalent wave. The infection was characterized by a low-grade fever for 1 day and a headache.
The sisters were symptom-free for 3 weeks; afterward, both developed extreme fatigue, joint pain, and cognitive/memory problems. Both were skilled at playing piano and had high rates at school. However, they complained that they could no longer play songs they played routinely. This situation was also confirmed by their piano teacher.
Similarly, at schools, they started presenting with memory blackouts and, during maths, could not do easy additions and multiplications. […] Six months later, given the lack of improvement, their family pediatrician referred both sisters to our post-COVID outpatient unit.
In balancing rosy statistics vs. harrowing anecdotes on the scales, the question is ultimately what “comfort” from rare bad outcomes we can possibly be enjoying from the Covid vaccines; haven’t we simply used a (possibly mildly helpful) remedy as pretext to stop caring? The eternal cruelty of fate still stalks in the shadows.
The cost of comfort
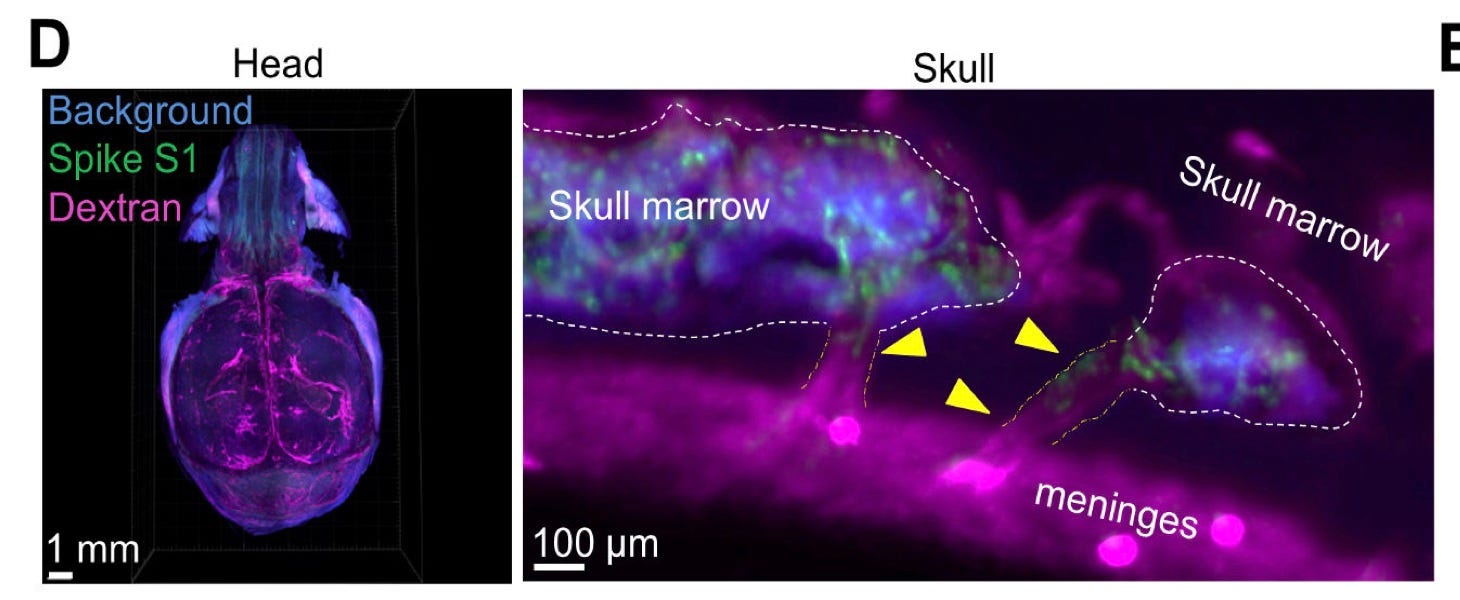
For those still interested in the bargain, all that is necessary to attain this barely-detectable, superpositional protection/non-protection from Long Covid is an injection that will instruct your body to pump out loads of spike protein. Topol, simultaneously reviewing the sensational pre-print finding that injected spike protein lodges itself in the skull of mice, assures his reader that no resemblance between the biodistribution of injected spike protein and circulating spike protein from mRNA-transfection can be presumed:
Of note, this work cannot be misconstrued to relate to Covid vaccines, a theoretical issue that would need to be separately explored.
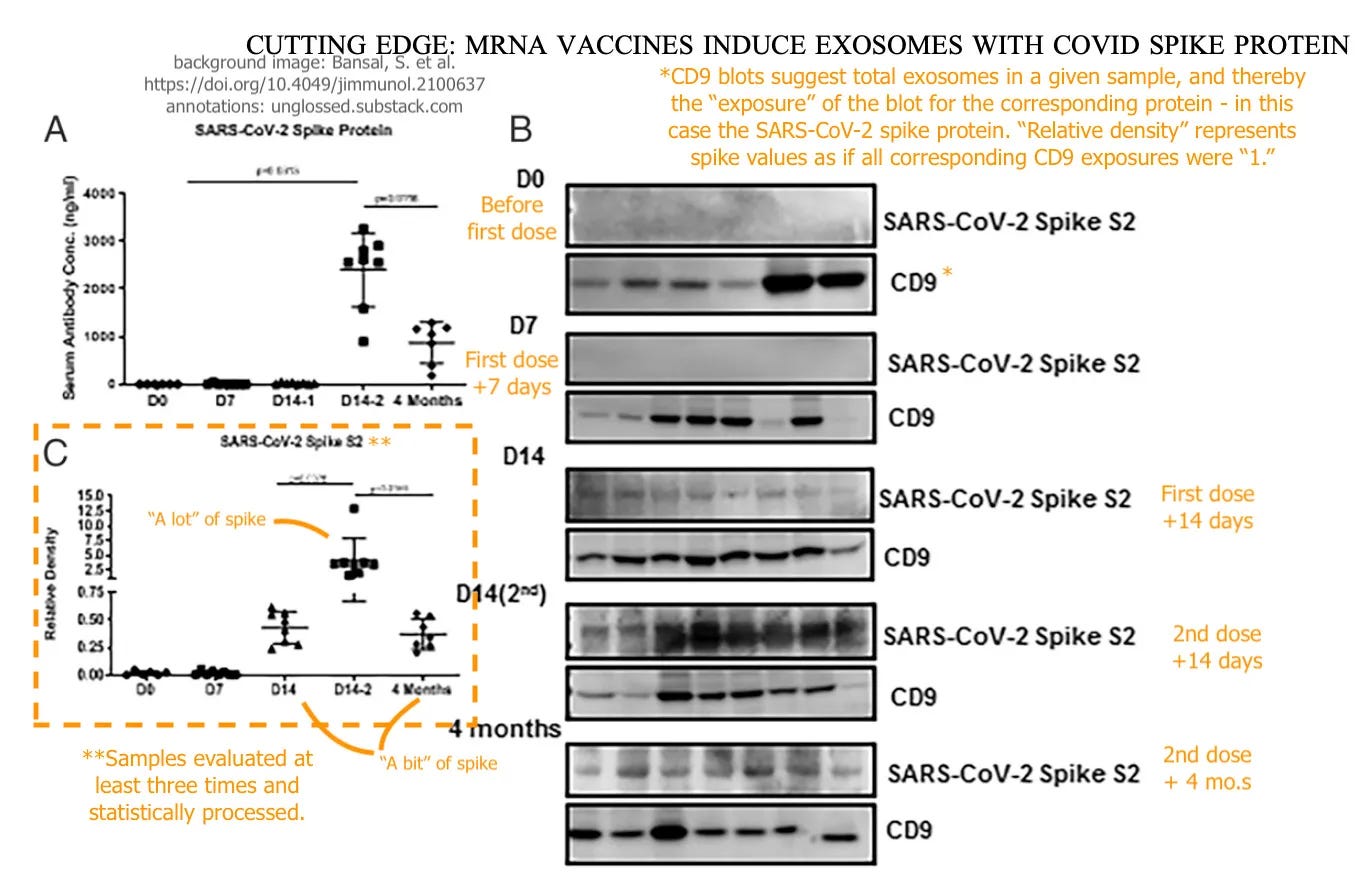
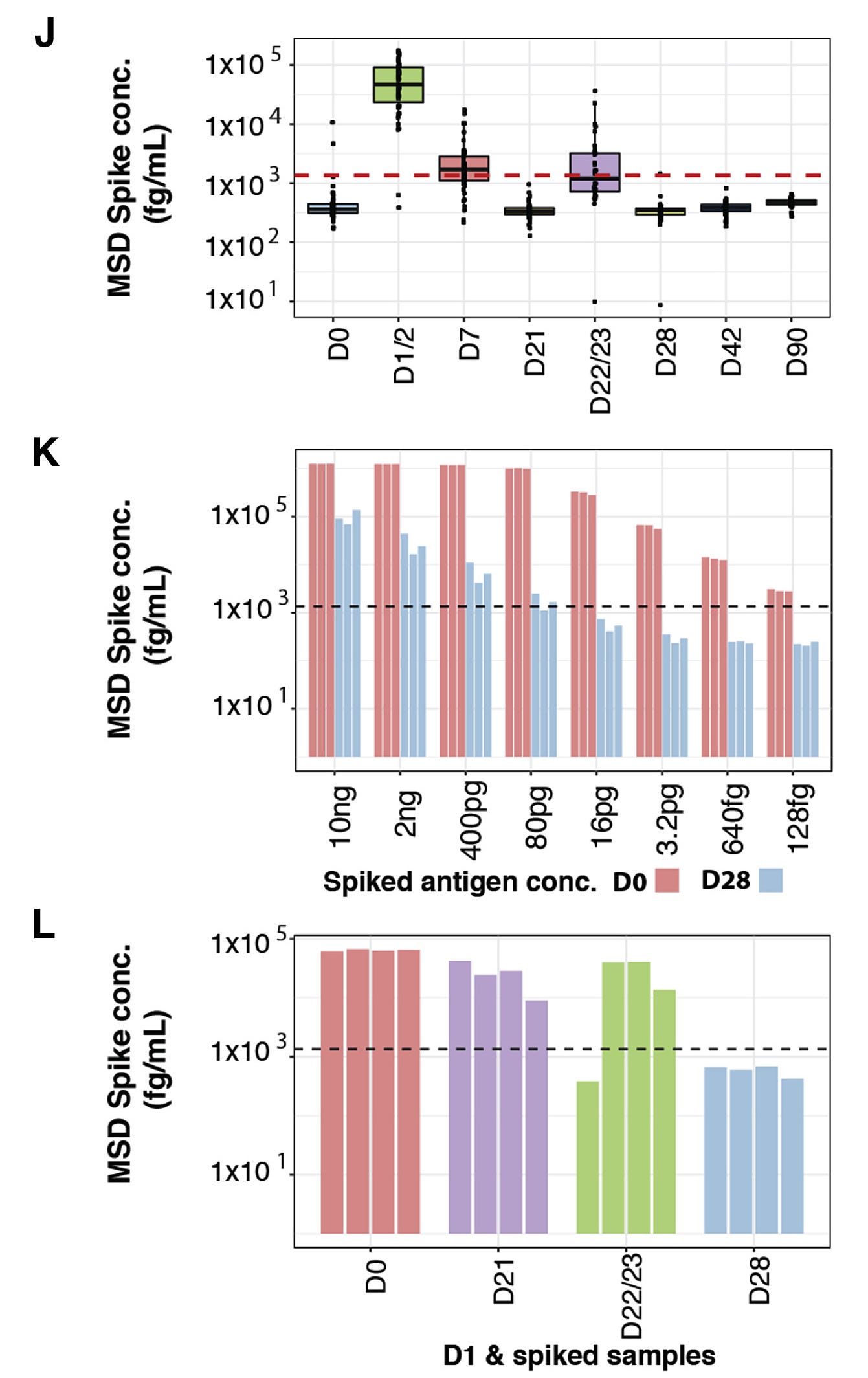
There is so much irony to be mined from Topol’s dismissing of a theoretical danger from an experimental medicine via insisting on the lack of any “exploration” of the danger; but irony lacks pleasure at this point. It should simply be said that Topol has taxed the bounds of the term “theoretical,” given that humans transfected with the mRNA vaccines have been demonstrated in multiple studies to have circulating spike protein in their blood for weeks and months.
Röltgen, et al. Fig. 7. This is a complicated presentation of the data; K and L are meant to demonstrate that the negative results on Day 28 (7 days post-dose-2) are potentially due to antibodies masking circulating spike, as some amounts of additional spike can be added to blood without being detected.
Theoretically, spike protein floating around in the blood after mRNA-transfection will not lodge itself into the skull the same way directly injected spike does because of impossible-to-fathom magical properties of nature. Putatively, it is safe to bet on a relationship; nothing about this is “misconstruing” anything.
This ends my jotting of thoughts; the reader is spared a meta-commentary conclusion about generic vaccine hubris.
Among kids enrolled for periodic antibody detection and surveys of self-reported long term symptoms, only 12 of the 551 kids (2.18%) who seroconvert for the Nucleocapsid protein (indicating infection) while categorized as vaccinated report long term symptoms, vs. 67 of 1,089 unvaccinated kids (6.15%). Although sampling combines the pre-and-post-vaccine eras, apparent efficacy cannot be entirely explained by a bias for Omicron infections (i.e. efficacy by procrastination), as post-Omicron long-termers outnumber all vaccinated long-termers. (Tables 1 and 2).
It takes a while to get used to Brian Mowrey’s writing style (seriously, Brian? “Putatively” instead of “probably”, “supposedly”, “ostensibly”, “seemingly”, “clearly”, …?) but there isn’t a better critical thinker out there who can put the uncritical thinkers (your Topol’s, Tufecki’s, et al) down so succinctly (okay: “concisely”?). And, for a guy who knows that analogies are more descriptive than argumentative, I definitely love it when Brian uses them to make his case—because he does it so well. Unbelievably well. And consistently. Example:
I highlight this rhetorical barb because it is so easy to point out the logical flaw here; Zeynep is engaging in mere sophistry. To see why, imagine for example that a town locks all its children into a basement for two years out of a mortal fear of… the rain. This imprisonment only ends upon the pretext of the discovery and deployment of a “solution” to the rain… rain-coats and umbrellas. The pro-imprisonment lobby, if criticized retrospectively, can cosset itself with the assurance that critics are minimizing the danger of the rain from the “comfort” of rain-coats and umbrellas. But this wouldn’t mean anything.
Dang. That’s some good stuff, Brian. Your brainiac rating is still a 10.
'Of note, this work cannot be misconstrued to relate to Covid vaccines, a theoretical issue that would need to be separately explored.' Maybe next time explore the theoretical issues that involve brains and deaths and major side effects before injecting a billion people? I mean or inject them first and just try and figure out it in the autopsies. Either way.









Restack with a (sorry) minor dig:
It takes a while to get used to Brian Mowrey’s writing style (seriously, Brian? “Putatively” instead of “probably”, “supposedly”, “ostensibly”, “seemingly”, “clearly”, …?) but there isn’t a better critical thinker out there who can put the uncritical thinkers (your Topol’s, Tufecki’s, et al) down so succinctly (okay: “concisely”?). And, for a guy who knows that analogies are more descriptive than argumentative, I definitely love it when Brian uses them to make his case—because he does it so well. Unbelievably well. And consistently. Example:
I highlight this rhetorical barb because it is so easy to point out the logical flaw here; Zeynep is engaging in mere sophistry. To see why, imagine for example that a town locks all its children into a basement for two years out of a mortal fear of… the rain. This imprisonment only ends upon the pretext of the discovery and deployment of a “solution” to the rain… rain-coats and umbrellas. The pro-imprisonment lobby, if criticized retrospectively, can cosset itself with the assurance that critics are minimizing the danger of the rain from the “comfort” of rain-coats and umbrellas. But this wouldn’t mean anything.
Dang. That’s some good stuff, Brian. Your brainiac rating is still a 10.
'Of note, this work cannot be misconstrued to relate to Covid vaccines, a theoretical issue that would need to be separately explored.' Maybe next time explore the theoretical issues that involve brains and deaths and major side effects before injecting a billion people? I mean or inject them first and just try and figure out it in the autopsies. Either way.
Great post Brian.