
Ivermectin's The Dress Moment
Did ivermectin work in Malaysia or not?


Do I believe in ivermectin’s efficacy against severe outcomes during infection with SARS-CoV-2? Well, to do so would require me to set down my innate skepticism of human powers of perception, and of the scientific method’s ability to decipher human health and disease. If doctors recommend it within a treatment regimen that they observe to prevent severe outcomes, then what I believe is that: “Doctors recommend it within a treatment regimen that they observe to prevent severe outcomes.”
I don’t believe that the studies show it works. I don’t believe this, because I don’t think the studies would show it works even if it does work. It’s simply too complicated to establish causality, in a study setting, for a biological event (infection with SARS-CoV-2, as proxied by a positive PCR test alone, or plus-symptoms) that is unlikely to cause severe outcomes for most people to begin with.
I don’t believe in going to war over ivermectin, even if it is “the other side” that is initiating the war. And if an individual on “our own side” is “siding” with “the other side” over ivermectin, I remain agnostic on whether that indicates the individual is more likely to be a “controlled op” or the individual calling the individual a “controlled op” is.
So anyway, my take on the controversial study from Malaysia:1 It does not show ivermectin works. It maybe supports the claim that the Covid vaccines prevent severe infection, but it was not designed to do so, and so it can’t actually do so (and the authors don’t even try to make it do so).

The setup, if you haven’t already been appraised. High-risk Malaysians over 50 who test positive for the virus, with mild or moderate symptoms, are recommended for hospital care or quarantine. 500 of said healthcare-status flagged, well-observed patients were intercepted around day 5, and not after day 7, post PCR-positive. Half were given ivermectin, half stayed on the rather unimpressive-sounding NIH and WHO-based “standard” care. The primary outcome was progression to severe illness - pneumonia with hypoxia requiring oxygen supplementation, or above. The secondary outcomes were some other stuff.
There was some unevenness in the comorbidities, potentially enough to half-hide the observed result, but otherwise they were randomized well enough. Notice the difference in chronic diseases:

Given that the absolute quantity of patients who progress to symptom-defined “severe” disease is so small, we have to wonder if the observed under-performance of ivermectin in the primary outcome could potentially be driven in some part by this disparity in risk categories. Even so, the results are unimpressive:

And, why shouldn’t they be? The patients were captured several days after onset of symptoms in most cases; if ivermectin is among other things an antiviral, it should probably be started during those several first days while the virus is doing stuff. Additionally, if it is “the protocol” (of which ivermectin is an element) that doctors ultimately have come to believe in, the protocol is not what is being tested here. Ultimately, these results cannot offer any reason to stop believing in ivermectin.
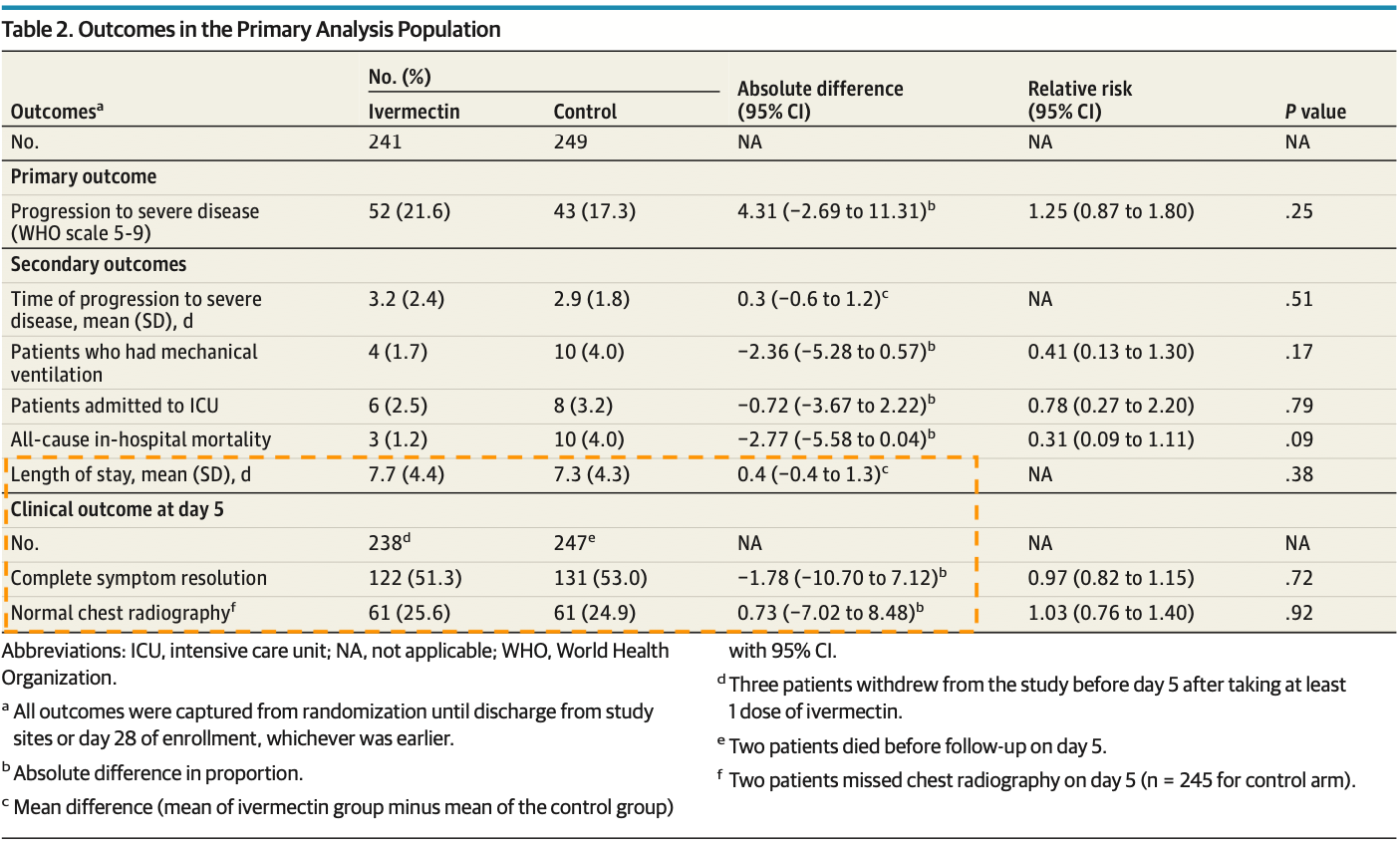
Nor, I would say, to believe in it. I do not agree that the results on ventilation, ICU, or death are impressive. These outcomes are too small to chalk up to the drug, rather than chance. I don’t care what the P values said, and whether the authors were a bit cavalier with dismissing their own secondary outcomes. Wake me when every subject of the study is showing the same effect and the effect is still declared “insignificant.” Maybe the authors’ dismissal of the death rates, despite defining death as a “secondary” outcome, makes them bad people; it doesn’t oblige me to disagree with them. Ten out of 249 control patients died during their bout with the virus. Could ivermectin have saved some? I don’t know, you don’t know. It could have been too late. Maybe these were day-7 recruits, and intervention wouldn’t have helped (two of the controls died before day 5 of observation). Maybe they needed the full protocol. Maybe we should rerun the test with them on the other side. Of course, that’s not how reality works. There are limits to what studies can reveal about the complexities and mysteries of biology, and randomization does not remove difference.
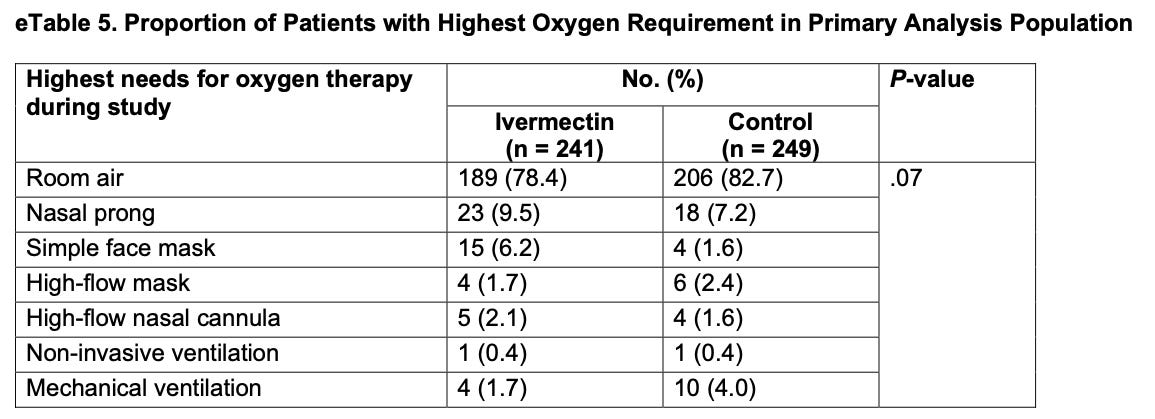
The authors probably shouldn’t have assigned the official “secondary” title to such unlikely-to-occur-much outcomes to begin with. If anything, I think these outcomes are less revealing than the extra data, which provides a more complete picture of the actual experience of infection for the two sets - and, ultimately, reinforces the ambiguous headline finding:

And perhaps most revealingly, the study reports the length of stay and day-5-of-observation recovery rate as follows:
Ivermectin, as (mis-/) applied in this study and setting, did not perform as a wonder drug. There’s no reason for anyone to change how they feel about the medication based on this. Those who believe in it should not consider this a fair test; those who do not believe in it would prefer that the drug never receives a fair test; in reality a fair test is probably impossible. What if more of the ivermectin group simply had the bad luck to face a virulent sub-strain? Who can say. People are different from each other in ways that cannot be statistically evened-out; the virus changes; numbers lie. The FLCCC will continue their work.2
On the subject of lying numbers - as mentioned, the Covid vaccines come out looking pretty good. However, interestingly, they appear to “lose” most of their apparent efficacy in the ivermectin treatment arm when it comes to severe outcomes, and in the control arm when it comes to death:

Only 12 of 130 double-dosed control patients progressed to severe illness, while 22 of 84 unvaccinated did (bear in mind, again, that these are all “high risk” and over-50 patients). That looks like efficacy against severe disease, but the dosed- and undosed- are not controlled against each other. Meanwhile, the poor performance of the Covid-vaccinated in the ivermectin cohort implies… well, that ivermectin apparently makes Covid-vaccination stop working.
A random fluke seems like the more likely explanation here. The study randomized the ivermectin and control groups by Covid-vaccination and comorbidities, but it didn’t randomize within those groups: There was nothing to stop all the high-comorbidity folks in the ivermectin set from being double-dosed, while only half the high-comorbidity patients in the control set were double-dosed. And yet, death protection was reversed, so who knows.
Maybe, just maybe… People are different from each other in ways that cannot be statistically evened-out, the virus changes, and numbers lie. Doctors should use the treatments they believe in. I’ll hang onto my skepticism about what the studies actually show.3

If you yourself have been skeptical of the research support for ivermectin, and haven’t already read Scott Alexander’s unflinching behemoth of a review of the reviews of the reviews, it’s worthwhile.
For myself, I have mostly found the studies to be ambiguous, often showing “no efficacy” because there are no severe outcomes. I also spent a long time gazing into the stats from India last year, and how they compared with state treatment guideline changes in favor of ivermectin or not, looking for something to hash a post out of. At most, Tamil Nadu’s May 7 re-reversal back to remdesivir made the delay between case peek and deaths peek longer than the ivermectin states? Anyway, I came away… ambivalent.
Wait, wait, wait. You're telling me the majority of the people in the study were vaccinated, and who knows for how long since? This study is utterly useless, as you say. The only people you could reasonably compare on testing Ivermectin would be those who were totally unvaxxed--the 75 and 84 (wherein 1 death vs 4 might mean something, but probably not enough power). Throwing vaccination in the mix, when we know it has powerful impacts on both short and mid-term immunity, negates any other results.
One of the distinctions of this virus has been the wide range of outcomes associated with a wide range of conditions. Further, the disease changes considerably as it progresses. So it acts like many different diseases, each responding best to tailored treatments. Enormously complex. Apparently there is no "magic" solution that works in all people, for all conditions, at all times during disease progression.
That single molecule quest is always the single-minded focus of medical orthodoxy. It only works for simple ailments, yet medical orthodoxy demands it. For example, we've spent trillions searching for a magic pill for Alzheimer's and so far have nothing. Doctors who successfully treat it are actively shunned, by other doctors as well as corrupt media.
Some doctors manage those complex variations with subtle indications better than others. But their skill becomes artificially restricted by arbitrary prohibitions. Ivermectin is not a one med fits all solution, but it works well in some situations. It's criminal to prohibit its use by competent doctors. Some docs are good enough that they can work around those criminal prohibitions. Dr Zelenko for example assembled a protocol not yet prohibited using over the counter pills and skilled supervision. He has had two years of nearly perfect success. Apparently the missing ingredient in Malaysia was competent doctors.
It's also criminal to withhold effective medicines from half your patients to prove a point to bored academics. The fetish of worshiping formal investigations during a lethal pandemic is a sickness unique to our pampered western society. Throughout history, we learned what worked from experience, and shared those experiences with others. Denying experience will be our undoing.