


If It Weren't for Those Meddling Immunocompromised Kids
In which Brian finds the "chronic infection" origin trope more convincing than assumed.

Is “Magic Immunocompromised Origin” more plausible than it seemed? Pausing the project to reevaluate.
First, two interesting pre-prints:
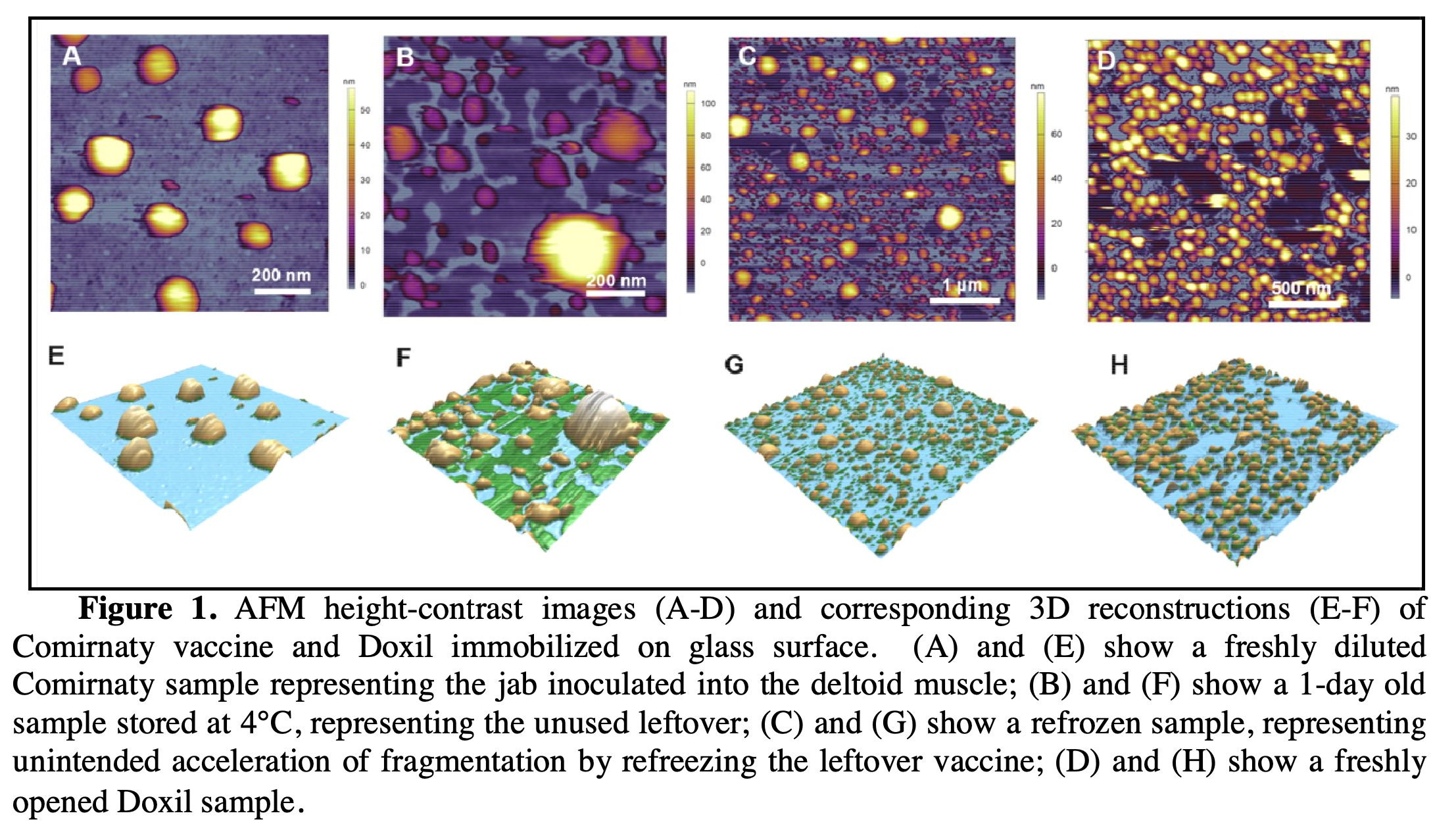
Interesting pre-print 1: Pictures of Covid vaccine LNPs.
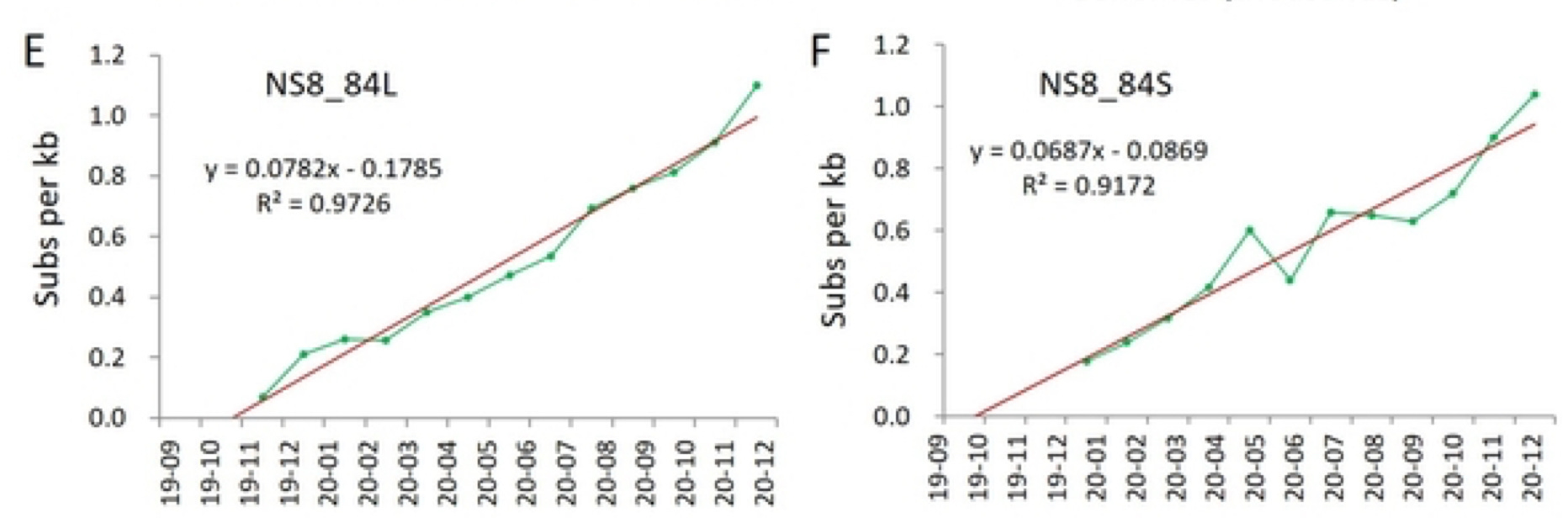
Interesting pre-print 2: Support for my recently-floated model of the “release” version of SARS-CoV-2 smoldering in China, Italy, and California, followed an Italian B.1 mutant colonizing the globe in late 2019, early 2020.1

It is always best to drop bad news on a Friday evening.
On Wednesday, I embarked on an attempt to analyze the “release-build” mutations of the “Variants of Concern” for (in)consistency with mutations that appear in natural infections (meaning within existing clades that don’t parachute out of the sky).
Natural mutations tend to be heavily driven by C>U transitions, a “transition” referring to changes where o-shaped nucleotides (pyrimidines, C and U) or oo-shaped nucleotides (purines, G and A) trade identity with each-other, rather than an “o” becoming an “oo” or vice-versa (which is called a “transversion”).2 This is the case regardless of whether said mutations are “good,” or whether they “take.” They could be bad; in fact probably are. But they are still more likely to occur. (And so probable-badness could be a problem for trying to use them as a “molecular clock,” but it still seemed like a productive lead.)
So I did a spreadsheet, and the signal for the VOC builds being “unnatural” was pretty obvious; transversions equalling or outnumbering C>U transitions being the big signal. “Boom, this one’s going to blow the lid open on the whole thing,” you can picture me saying:

(Especially impressive is after BA.1 and BA.2 diverge, but before they leap into circulation and are sequenced, BA.2 recovers the “natural” C>U = 2transversions mutation signature, proving that the signature still reflects some type of mutational preference on the part of the virus.)
So, the last step, before converting the sheet to a devastating Canva™ graph, was to demonstrate that published chronic infection sequences don’t display the same signature.
Well, they… kind of do.3

Now, this doesn’t totally rescue “There should be variants” and kill “There should not be variants” with fire. Even if chronic infections can produce VOC-like mutation signatures, it still does not make sense that lowering innate immunity makes transmission-competent viruses, as opposed to generating a lot of “inbred” mutants. Nonetheless, it remains evident that chronic infections can produce VOC-like, transversion-heavy mutation signatures. The most recently-published even produces the signature nsp6 deletion shared by literally all the VOCs.4

So, I will take the weekend to thdrink on this development.
Anyway the Omicrons are still nowhere close to the “ballpark” of sequences derived from any chronic infections or mouse passage studies. That’s right! Remember the Omicronamo!

In other news, my SARS-CoV-2 sequence text file has now graduated to “version 1.1,” and includes Beta and the Omicrons. It’s at the hub:
With that: Happy weekend, and thanks for subscribing to Unglossed!
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


All roads lead back to October…

Simmonds, P. “Rampant C→U Hypermutation in the Genomes of SARS-CoV-2 and Other Coronaviruses: Causes and Consequences for Their Short- and Long-Term Evolutionary Trajectories.” mSphere. 2020 May-Jun; 5(3): e00408-20.
Choi, B. et al. “Persistence and Evolution of SARS-CoV-2 in an Immunocompromised Host.” N Engl J Med. 2020 Dec 3;383(23):2291-2293.
Lustig, G. et al. “SARS-CoV-2 evolves increased infection elicited cell death and fusion in an immunosuppressed individual.” medrxiv.org
(It doesn’t “evolve increased fusion.” It evolves very-decreased and then less-decreased fusion, vs. wild-type.)
Brian, the last several posts of yours were exceptionally interesting, but unfortunately I realized that I cannot evaluate their correctness due to not knowing enough. I try my best to follow each of them however.
Have you seen recent, and NOT so recent suggestions that the latest variant soup is driven by molnupiravir?
Cool, nice job detective. 🧐