


IgG4 and T Cells
A new study suggests T helper mediation of IgG4 class-switching. Also, correcting some HIV details: Brian did a misinformation

This is a cross-post of a substantial update made to my “Tolerance Cometh,” post, as a new preprint upends some rather rash conclusions I made when reviewing Irrgang, et al., regarding T Cells and IgG4.
This new study takes a different approach to the question of whether T Cells are mediating IgG4 — does giving people a T helper inhibitor drug suppress post-Covid-vaccine IgG4? Yes, it does, nearly totally. This provides an illuminating insight into the mechanism of IgG4 conversion, even if it doesn’t have any implications for the effects of IgG4 on future infections, which are still of course unknown.
The update also adds some details about Pfizer’s arbitrary process for selecting the original dosage for BNT162b2, their mRNA vaccine, which are included here (as a footnote).

First, corrections on HIV
Before correcting my IgG4/T Cell statements, an alert regarding three errors made in my posts regarding the early history of HIV. These came to light thanks to discovering Jacques Pépin’s The Origin of Aids (hat tip to commenter “TCC”). The first two are minor, the second more substantial.
First, I at some point became confused on which lay term to use for the chimpanzee that is the host for the precursor to HIV — it is “central-,” not “west-African.” Apologies to anyone with west-African-chimpanzee family members.
Second (and this hasn’t been corrected in my post yet), it is no longer held that SIV-CPZ (the ancestor of HIV) is not pathogenic in central-chimpanzees. I have yet to review the study in question to see if it is really so convincing, but this is an interesting though not immediately obvious piece of evidence on the question of HIV 1M’s pathogenicity in humans, which may inform the next post on the topic.
The bigger error is that I was unaware that the absence of HIV in parts of Africa outside the Congo region up to 1980-or-so has been thoroughly demonstrated. As such, the virus spread almost exclusively in the Congo region, and all references to its spreading in Africa before 1980 have been made more precise in kind.
This revelation forced a reworking of my comments on the development of 1M’s subgroups (1M being the primary virus of the HIV epidemic, essentially synonymous with “HIV”), though not in any substantial manner so far as the import of those subgroups (i.e., that 1M must have entered humans near the beginning of the 20th Century or earlier).
I had claimed, and made a bit of a point of the claim, that 1M’s subgroups developed in geographic isolation. This, I have now realized, was because the idea of geographic isolation had short-circuited a more important intuition which I was trying to work out regarding the relative lack of recombination before 1980.
What this lack of recombination reflects, what it is an archeological record of, is not that HIV subgroups spent a long, long time being geographically isolated from each other, but that HIV while in the Congo region spent a long, long time being rare. As long as HIV is not in populations (i.e. groups of people intermingling sexually or via needles or transfusion) where the prevalence is high, then chances are not good for a co-infection, and each strain builds and builds its mutational differences in isolation, until at last (at 1980) you have eight to ten subgroups which are extraordinarily different from each other genetically and yet have managed not to recombine very much, if at all. And so the relative purity of the subgroups’ oldest (now, more consensus) mutations from their last common ancestor is an archeological record of this long period of rarity in the human reservoir of the Congo region. This point is restated in an edit made to Pt. 1.5.
This is another, though in of itself not overwhelming, point of inconsistency with the theory that HIV came from massive polio vaccine trials, as one would expect widespread contamination and a quicker transition from rare to prevalent in the Congo between the 50s and 1980, resulting in promiscuous recombination. If 1M is introduced into just one person and allowed to spread afterward for a long time primarily sexually, then the subgroups are allowed to grow genetically distinct in isolation from each other. Some more remarks regarding the question of whether 1M’s genetic diversity could instead have been developed in the polio vaccine “chimpanzee camp,” as claimed — why this isn’t plausible — are offered in the comments.
IgG4 Switching and T Cells
Irrgang, et al., (the original IgG4 study), took a look at the question of whether Th2 Helper T Cells are mediating conversion to IgG4, in accordance with the present understanding of how class-switching operates. They wound up producing an ambivalent conclusion.
Another preprint has appeared which reports the result of an accidental experiment more suited to answering the question.1
In Valk, et al. an ongoing study into Covid vaccine responses among patients receiving immunosuppressants for immune mediated inflammatory disease was used to look for any effect on eventual IgG4 conversion (found, as with Irrgang, et al. to be underway a while after the 2nd dose, and to intensify after the 3rd dose, in unmedicated controls).
They found a compellingly extreme reduction in patients receiving inhibitors for either the IL-4/IL-13 receptor or the cytokine TNF. A third drug had no such effect.
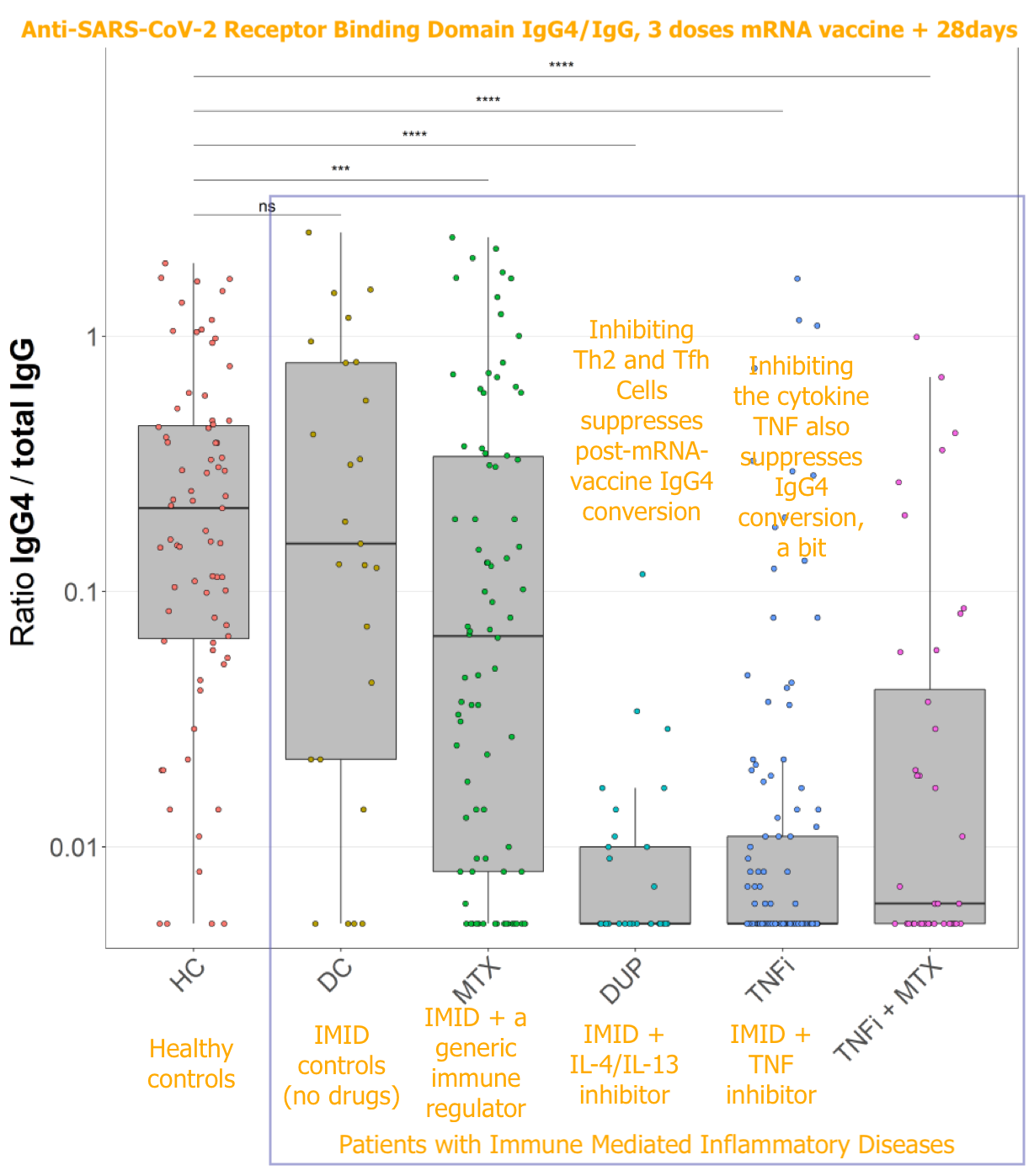
IL-4 is a cytokine associated with proliferation of Th2 and T follicular helper (Tfh) cells during immune responses, and is implicated in T helper mediation of IgG4 class-switching. That blocking IL-4/IL-13 blunts IgG4 conversion demonstrates, rather convincingly, that T Cells are mediating post-mRNA IgG4 class switching.
The authors point out that persistent Tfh cells have been observed after mRNA vaccination. In the referenced study,2 SARS-CoV-2 spike-sensitive Tfh cells are plentiful in both lymph nodes and blood after BNT162b2 (Pfizer) vaccination, and these persist for the entire observation window (up to 200 days after the first dose). This study involved a small cohort of young adults, but results were consistent.
Persistence of Tfh cells in the blood was nonetheless featured by a decline from initial highs; whereas lymph node germinal center Tfh populations remained high, suggesting prolonged development and maturation of the anti-spike immune response after the second dose, before any additional doses. This is once again in line with the model I have proposed for IgG4 conversion — as much more the result of the long-term effect of the first doses, rather than a consequence of the booster. Of course, boosters can only hurt further — but if the 2nd dose’s effects on IgG4 take time to show up, then there is no reason to assume that even 1 dose alone could not also cause IgG4.3
Back to Valk, et al., the (substantial, but less-so) efficacy of TNF inhibition is less obviously consistent with what is known about IgG4 conversion as TNF is a more generic cytokine employed by a gamut of immune cell types. Suffice it to say that our understanding of the immune system is incomplete.
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Valk, AM. et al. “Suppressed IgG4 class switching in dupilumab- and TNF inhibitor-treated patients after repeated SARS-CoV-2 mRNA vaccination.” medrxiv.org
The conflict-of-interests statement on this preprint is quite substantial, with two tangential references to Pfizer. Given that it elucidates aspects of an unexpected problem with the mRNA vaccines, it serves as an example of why I don’t fret and scold over on-paper conflicts of interests as a generic issue. It’s hardly as hazardous to the truth in scientific research as ordinary human confirmation bias.
Mudd PA. et al. “SARS-CoV-2 mRNA vaccination elicits a robust and persistent T follicular helper cell response in humans.” Cell. 2022 Feb 17;185(4):603-613.e15
It seems obvious that the mRNA vaccines both deliver too much (nucleotide-modified) mRNA, calling into question the “need” for a second dose to begin with. Though this isn’t necessarily what drives the long duration of germinal center responses, it’s worth noting that other differences vs. the vector vaccines wouldn’t seemingly last very long, e.g. the pro-inflammatory nature of the LNPs. At all events, mRNA overkill is a reason to suspect that just one dose may be enough to induce IgG4.
Amount of mRNA was intentionally maximized, at least in the development of Pfizer (I have done less reading for Moderna’s process, but obviously they went beyond Pfizer in amount of mRNA anyway). It was not set to meet any “just enough” standard.
To summarize Pfizer’s Clinical Overview (accessible by searching “clinical” at https://phmpt.org/pfizer-16-plus-documents/), BNT162b2 was trialed at different doses (1, 3, 10, 20, 30μg) with 12 young and 12 older subjects, in parallel with BNT162b1 which only had a young cohort; as well, 60 and 100μg formulations were tested for BNT162b1, but due to higher side-effects after the first dose, these were not re-used nor trialed in BNT162b2.
The top-line statement of the rationale for choosing 30μg was that it had “robust immunogenicity in both younger and older Phase 1 participants” (section 2.5.1.2.5); but as no standard for “robust” is ever formulated in advance or retrospect, this statement simply means that 30μg made a bit more antibodies than the others — which isn’t any different from simply saying “bigger dose best, ung ung.” As such the Phase 1 immunogenicity comparison with lower doses was irrelevant; the highest that could not obviously cause more side-effects was chosen, and no attempt was made to set a standard for “just enough protection.”
This is revealed by a few quotes in section 2.5.4.4, e.g. “For younger BNT162b2 recipients at the 10 to 30 μg dose levels, Day 85 neutralizing GMTs ranged from 1.3- to 1.9-fold that of [post-infection antibodies.]” — Therefore, the difference between 10 and 30 wasn’t that great, and a post-infection benchmark suggested that 10 is as good as natural immunity.
Also, “For BNT162b2, by 7 days after Dose 2 (Day 29) GMTs had increased substantially in younger participants who received doses of ≥3 μg and in older participants who received 20 μg.” — From the perspective of a one-size-fits-all standard — “robust immunogenicity in both younger and older” — 20 seemingly should have been the final choice; but for the young, 3. That is, had there been anything like a real option to choose something less than 30, which there was not.
Finally, “On Day 43 (3 weeks after Dose 2 of BNT162b2), neutralizing GMTs in the younger groups decreased at the 3, 20 and 30 μg levels. Thereafter, neutralizing GMTs remained stable up to Day 85…” — Therefore, 30 μg wasn’t chosen because of any substantial difference in durability of immune response.
This leaves only one detail that can justify the decision to maximize the dosage — a higher boost after Dose 2 — but this applies to BNT162b1.
Full marks for correcting previous offerings when new data are found. The random selection of dosages mention in the references shouts loudly that such a casual approach may, just may have had a more deliberate intent.
Of interest is a, so far, single non reviewed - so unconfirmed report that the mRNA materials used in the trials and subsequently offered to all the trial participants differed perhaps significantly to the mRNA materials injected in the roll out to the public. If this is confirmed or in any way correctly substantiated then what the general public were injected with was completely without trial and informed consent was impossible. That the trial results were not available for that mRNA material the first 'type' produced and only began dribbling out around March 2022 well after the massive push with the 'unknown' second production mix or type, the implications of what can only be described as probably deliberate actions to deceive are huge.
Before anyone starts yelling about this however caution requires that all this MUST be very carefully examined and confirmed before conclusions can be drawn. The picture is not looking good but is unclear. The inplications, horrendous.
Wait. Do I have this correct? Big Pharma has a drug that can ameliorate the problems caused by the modRNA gene therapy that was forced on lots of people?