

Post-mRNA Myocarditis: The First 180 Days
Post-mRNA Myocarditis: The First 180 Days
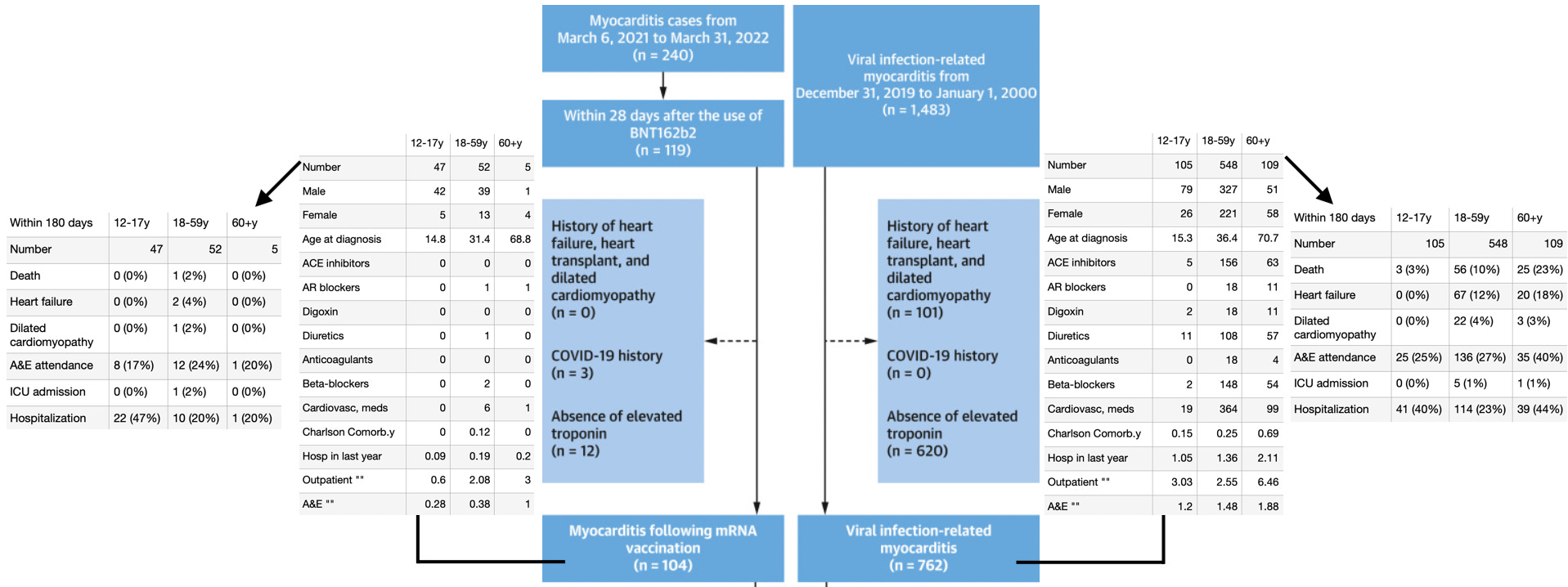
1 out of 99 myocarditis patients dead in the under 60 years old group, in a study from Hong Kong.

A new health records trawl in Hong Kong attempts to benchmark outcomes for post-Pfizer/BioNTech mRNA Covid vaccine myocarditis vs. the old-fashioned (as in pre-SARS-CoV-2) viral infection variety. The results are ambiguous, neither reassuring nor outright dire.
The study:1
Let’s jump straight in.
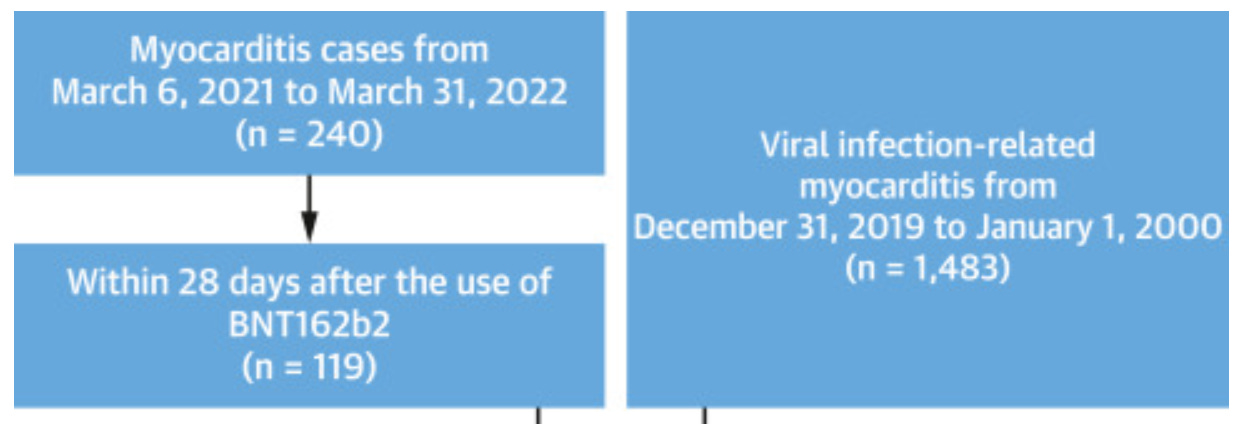
Almost exactly half of all myocarditis incidents in the Hong Kong Hospital Authority database between March, 2021 and March, 2022 were within 28 days of a Pfizer/BioNTech (BNT162b2) injection.
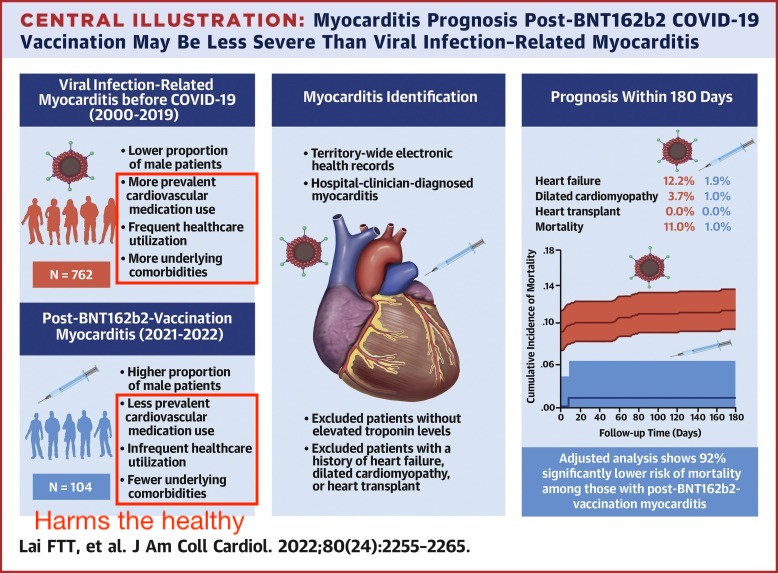
Compared to historic viral myocarditis, post-BNT162b2 myocarditis occurred in individuals with no previous record of medical dependency; it harmed the young and healthy:
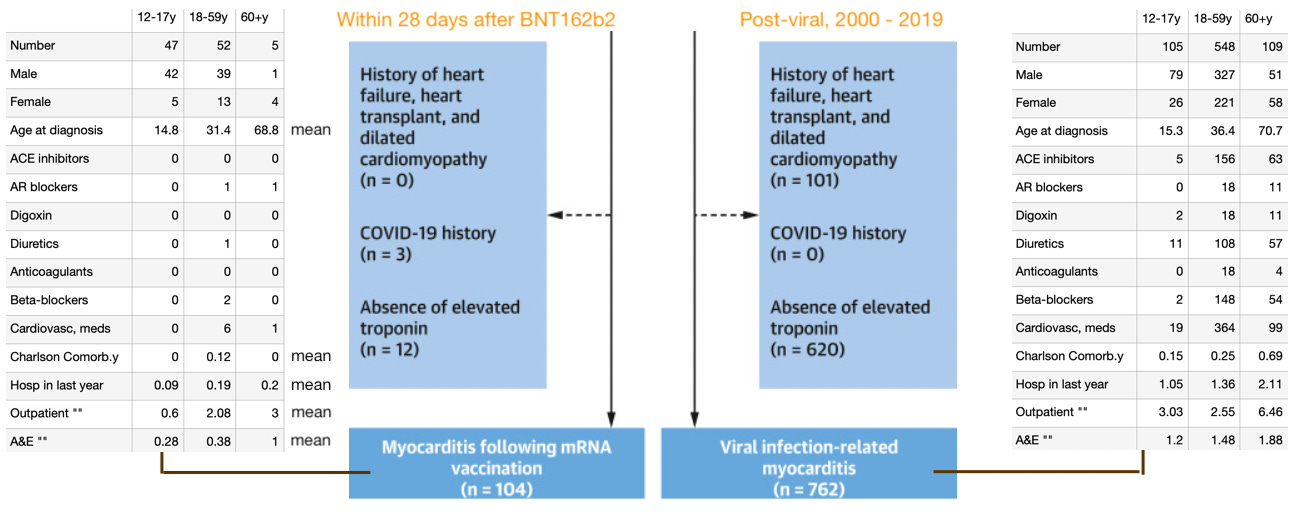
As shown above, even after removing individuals from the post-viral group with heart failure, etc., that group abounds with pre-existing indicators for heart conditions that can drive higher mortality in the study’s 180-day window; while the BNT162b2 group is nearly free of the same. For this reason, the study’s comparison between the two groups in terms of outcomes is not valid (while the comparison in terms of who is harmed, and likely disparity in years of potential life lost in the long term is damning).
And so, it is neither surprising nor reassuring that extreme outcomes like death are so frequent in the highly co-morbid post-viral group, but rare in the previously healthy post-BNT162b2 group, in the incredibly brief time-frame being measured.
With 180-day outcomes added to the previous schematic:

Remarks
It may be the case that Lai, et al., is reason to think that post-mRNA myocarditis might not reflect the dire prognosis of historic post-viral myocarditis (the 5 years to live trope). But Lai, et al. also demonstrates — if one applies even a bit of rational thought to the situation — that the likely reason for any such difference is that the vaccine is so good at damaging the hearts of the healthy.
As such, the impact — in years of life lost — will still be worse even if the prognosis appears more rosy. A 60 year-old who dies 5 years after an infection with SARS-CoV-2 lives to 65; a 15 year-old who dies 10 years after a totally unnecessary injection with an experimental gene-therapy product…
Of course, that’s all merely hypothetical anyway. The rarity of severe outcomes at 180 days is not sufficient evidence, yet, to assure the harmed that they will make it to 2026 without appearing on a headline. At the moment, the “died suddenly” trend remains a phenomenon seemingly making up its mind about how many 0s to put on the end. 1 in 1,000,000? One in 1,000? 1 in 10?
Regardless, Lai, et al. is already being weaponized as another argument in favor of pre-exonerating the vaccine (and its peddlers) for this poison’s own most obvious crime.
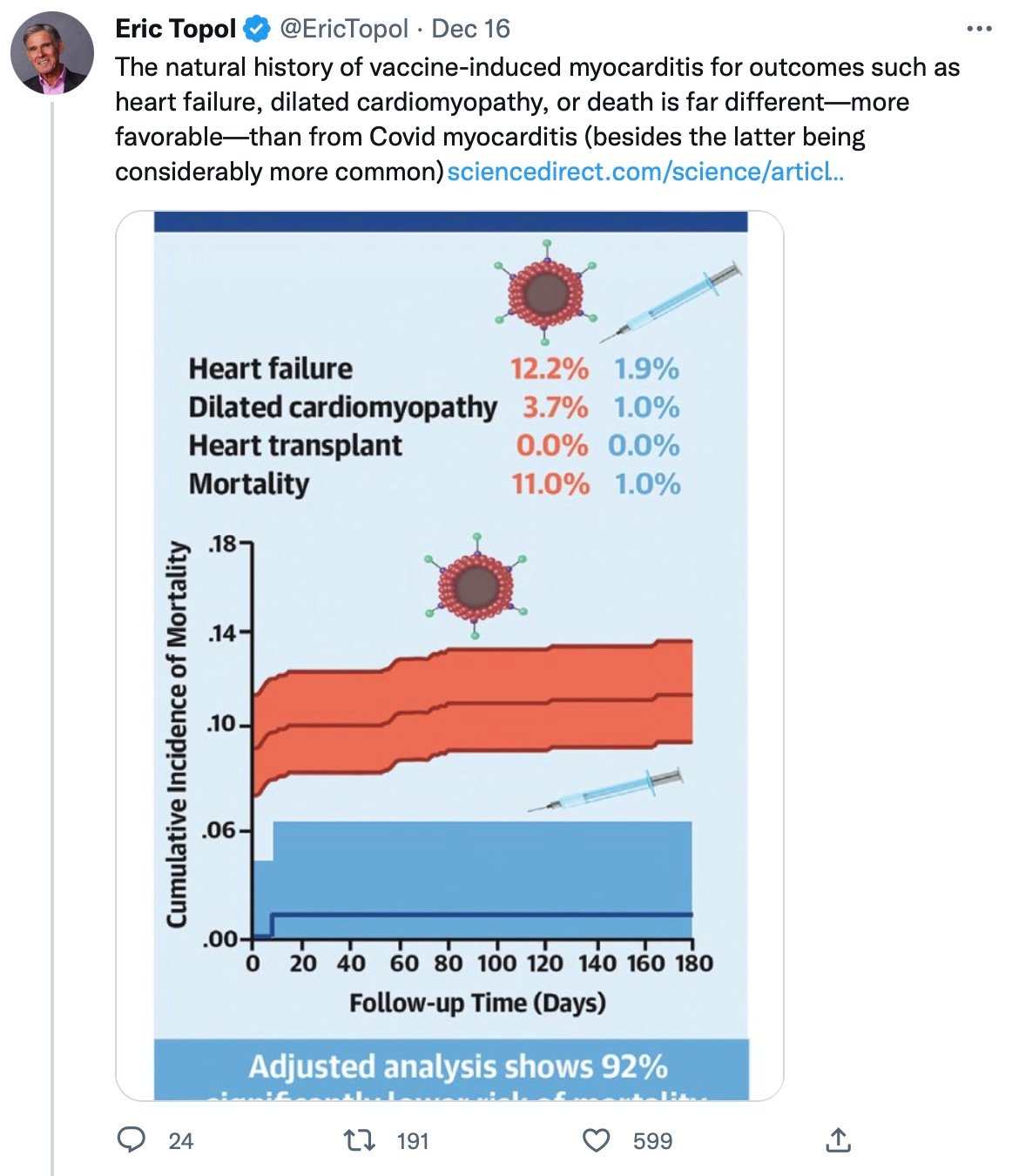
By post-infection myocarditis being “considerably more common,” Eric Topol presumably means “if you consider only all people together, old and young, and stonewall the clear and repeated findings of higher rates in young males forever” (repeat a lie often enough, as they say).
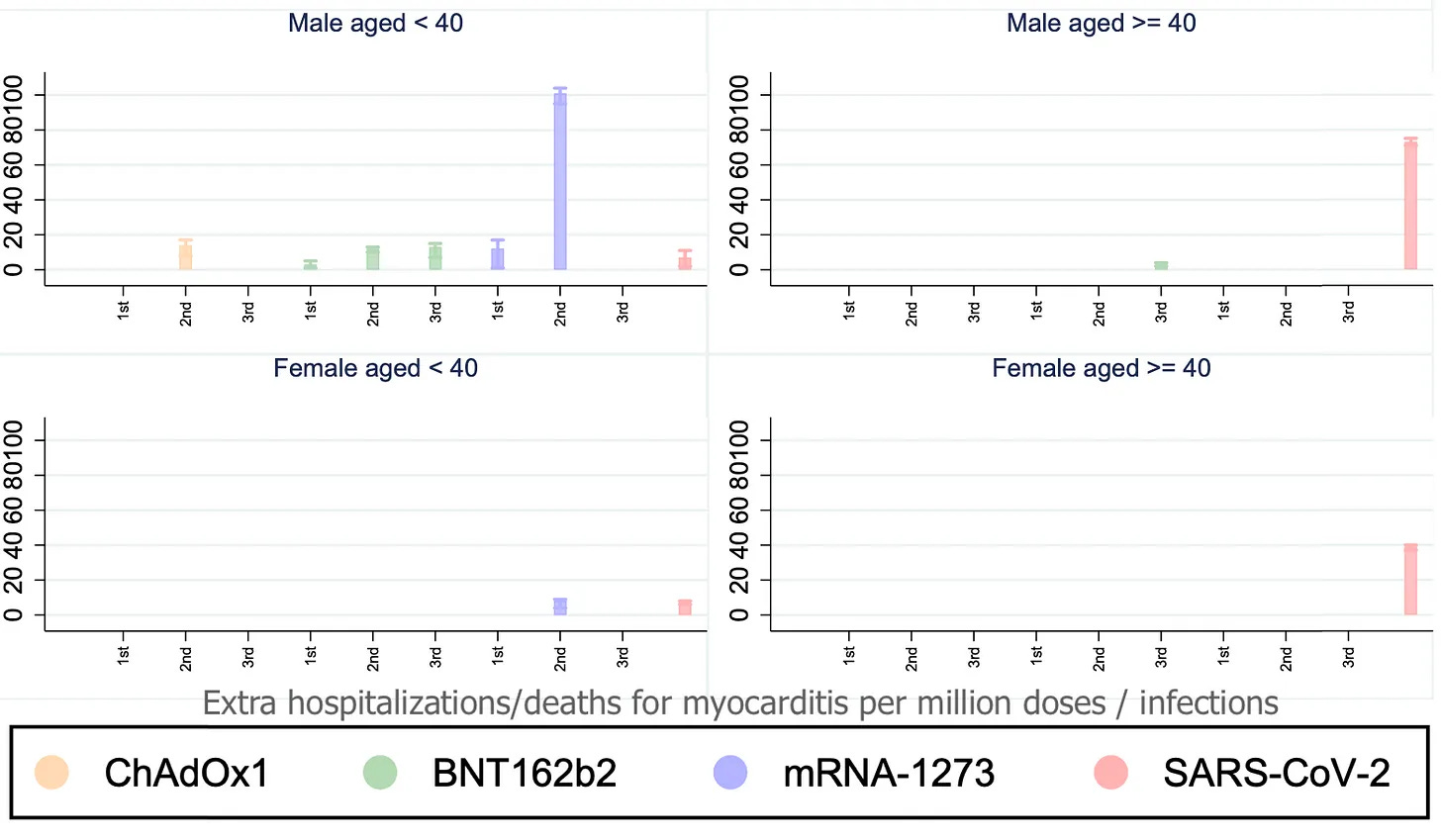
Or perhaps he means, if you only consider inaccurate health record trawls that may be distorted from who-knows-what sorts of biases, rather than the only direct, prospective assessments of the real rate after injection, which include a horrifying 3.5% (for myo- and peri-carditis) among teen boys:

Or perhaps he means, if you only consider the right-most panel of Lai, et al.’s summary graphic, and leave out the one on the left, which highlights in plain view the exact same confounding variables I have pointed out in this post:
We’ve come a long way from the Aztecs, whose priests used to justify carving out the hearts of the young with fantasies of sun gods and elaborate rituals. Ours use statistical obfuscation and tossed-off tweets.
If you derived value from this post, please drop a few coins in your fact-barista’s tip jar.


Another substack article about this:
"The Virus" 11 Times More Dangerous than Pfizer Jab, The Atlantic Quotes New "Study"
https://live2fightanotherday.substack.com/p/the-virus-9-times-more-dangerous
We know that T-cells cannot activate B-cells to produce antibodies when a person has low calcifediol levels (20ng/ml or lower it seems.)
What if that also prevents them from removing the shed S-protein from their blood stream (because macrophages etc cannot find them) and thus causes more blood clots and more attacks on important organs.
Has anyone measured the serum levels of calcifediol in those who died suddenly? Is there a negative correlation?